Drug Detail:Entereg (Alvimopan [ al-vi-moe-pan ])
Drug Class: Peripheral opioid receptor antagonists
Highlights of Prescribing Information
ENTEREG® (alvimopan) capsules, for oral use
Initial U.S. Approval: 2008
WARNING: POTENTIAL RISK OF MYOCARDIAL INFARCTION WITH LONG-TERM USE: FOR SHORT-TERM HOSPITAL USE ONLY
See full prescribing information for complete boxed warning.
- Increased incidence of myocardial infarction was seen in a clinical trial of patients taking alvimopan for long-term use. (5.1)
- ENTEREG is available only through a restricted program for short-term use (15 doses) called the Alvimopan REMS Program. (5.1, 5.2)
Indications and Usage for Entereg
ENTEREG is an opioid antagonist indicated to accelerate the time to upper and lower gastrointestinal recovery following surgeries that include partial bowel resection with primary anastomosis. (1)
Entereg Dosage and Administration
- For hospital use only. (2)
- The recommended dosage is 12 mg administered 30 minutes to 5 hours prior to surgery followed by 12 mg twice daily beginning the day after surgery until discharge for a maximum of 7 days. Patients should not receive more than 15 doses of ENTEREG. (2)
Dosage Forms and Strengths
Capsules: 12 mg (3)
Contraindications
Patients who have taken therapeutic doses of opioids for more than 7 consecutive days prior to taking ENTEREG. (4)
Warnings and Precautions
- Myocardial Infarction: A higher number of myocardial infarctions was reported in patients treated with ENTEREG 0.5 mg twice daily compared with placebo in a 12-month study in patients treated with opioids for chronic non-cancer pain, although a causal relationship with long-term use has not been established. (5.1)
- Gastrointestinal Adverse Reactions in Opioid Tolerant Patients: Patients recently exposed to opioids may be more sensitive to the effects of ENTEREG and experience gastrointestinal adverse reactions (e.g., abdominal pain, nausea and vomiting, and diarrhea). (5.3)
- Patients with Severe Hepatic Impairment: Increased risk of serious adverse reactions due to higher plasma concentrations; use is not recommended. (5.4, 8.6)
- Patients with End-Stage Renal Disease: No studies have been conducted; use is not recommended. (5.5,8.7)
- Patients with Complete Gastrointestinal Obstruction: No studies have been conducted in patients with complete gastrointestinal obstruction or in patients who have surgery for correction of complete bowel obstruction; use is not recommended. (5.6)
- Patients with Pancreatic and Gastric Anastomoses: No studies have been conducted; use is not recommended. (5.7)
Adverse Reactions/Side Effects
Most common adverse reaction (≥1.5%): dyspepsia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp & Dohme LLC at 1-877-888-4231 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
Use In Specific Populations
- Hepatic Impairment: Monitor patients with mild-to-moderate impairment for gastrointestinal adverse reactions. (8.6)
- Renal Impairment: Monitor patients with mild-to-severe impairment for gastrointestinal adverse reactions. (8.7)
- Race/Ethnicity: Monitor Japanese patients for gastrointestinal adverse reactions. (8.8)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2022
Full Prescribing Information
WARNING: POTENTIAL RISK OF MYOCARDIAL INFARCTION WITH LONG-TERM USE: FOR SHORT-TERM HOSPITAL USE ONLY
There was a greater incidence of myocardial infarction in alvimopan-treated patients compared to placebo-treated patients in a 12-month clinical trial, although a causal relationship has not been established. In short-term trials with ENTEREG®, no increased risk of myocardial infarction was observed [see Warnings and Precautions (5.1)].
Because of the potential risk of myocardial infarction with long-term use, ENTEREG is available only through a restricted program for short-term use (15 doses) under a Risk Evaluation and Mitigation Strategy (REMS) called the Alvimopan REMS Program [see Warnings and Precautions (5.1, 5.2)].
1. Indications and Usage for Entereg
ENTEREG is indicated to accelerate the time to upper and lower gastrointestinal recovery following surgeries that include partial bowel resection with primary anastomosis.
2. Entereg Dosage and Administration
For hospital use only. The recommended adult dosage of ENTEREG is 12 mg administered 30 minutes to 5 hours prior to surgery followed by 12 mg twice daily beginning the day after surgery until discharge for a maximum of 7 days. Patients should not receive more than 15 doses of ENTEREG.
ENTEREG can be taken with or without food [see Clinical Pharmacology (12.3)].
3. Dosage Forms and Strengths
12 mg blue, hard-gelatin capsules with "ADL2698" printed on both the body and the cap of the capsule.
4. Contraindications
ENTEREG is contraindicated in patients who have taken therapeutic doses of opioids for more than 7 consecutive days immediately prior to taking ENTEREG [see Warnings and Precautions (5.3)].
5. Warnings and Precautions
5.1 Potential Risk of Myocardial Infarction with Long-Term Use
There were more reports of myocardial infarctions in patients treated with alvimopan 0.5 mg twice daily compared with placebo-treated patients in a 12-month study of patients treated with opioids for chronic non-cancer pain (alvimopan 0.5 mg, n = 538; placebo, n = 267). In this study, the majority of myocardial infarctions occurred between 1 and 4 months after initiation of treatment. This imbalance has not been observed in other studies of ENTEREG in patients treated with opioids for chronic pain, nor in patients treated within the surgical setting, including patients undergoing surgeries that included bowel resection who received ENTEREG 12 mg twice daily for up to 7 days (the indicated dose and patient population; ENTEREG 12 mg, n = 1,142; placebo, n = 1,120). A causal relationship with alvimopan with long-term use has not been established.
ENTEREG is available only through a program under a REMS that restricts use to enrolled hospitals [see Warnings and Precautions (5.2)].
5.2 Alvimopan REMS Program
ENTEREG is available only through a program called the Alvimopan REMS Program that restricts use to enrolled hospitals because of the potential risk of myocardial infarction with long-term use of ENTEREG [see Warnings and Precautions (5.1)].
Notable requirements of the Alvimopan REMS Program include the following:
ENTEREG is available only for short-term (15 doses) use in hospitalized patients. Only hospitals that have enrolled in and met all of the requirements for the Alvimopan REMS program may use ENTEREG.
To enroll in the Alvimopan REMS Program, an authorized hospital representative must acknowledge that:
- hospital staff who prescribe, dispense, or administer ENTEREG have been provided the educational materials on the need to limit use of ENTEREG to short-term, inpatient use;
- patients will not receive more than 15 doses of ENTEREG; and
- ENTEREG will not be dispensed to patients after they have been discharged from the hospital.
Further information is available at www.alvimopanREMS.com or 1-800-278-0340.
5.3 Gastrointestinal-Related Adverse Reactions in Opioid-Tolerant Patients
Patients recently exposed to opioids are expected to be more sensitive to the effects of mu-opioid receptor antagonists, such as ENTEREG. Since ENTEREG acts peripherally, clinical signs and symptoms of increased sensitivity would be related to the gastrointestinal tract (e.g., abdominal pain, nausea and vomiting, diarrhea). Patients receiving more than 3 doses of an opioid within the week prior to surgery were not studied in the postoperative ileus clinical trials. Therefore, if ENTEREG is administered to these patients, they should be monitored for gastrointestinal adverse reactions. ENTEREG is contraindicated in patients who have taken therapeutic doses of opioids for more than 7 consecutive days immediately prior to taking ENTEREG [see Contraindications (4)].
5.4 Risk of Serious Adverse Reactions in Patients with Severe Hepatic Impairment
Patients with severe hepatic impairment may be at higher risk of serious adverse reactions (including dose-related serious adverse reactions) because up to 10-fold higher plasma concentrations of alvimopan have been observed in such patients compared with patients with normal hepatic function. Therefore, the use of ENTEREG is not recommended in this population [see Use in Specific Populations (8.6)].
5.5 End-Stage Renal Disease
No studies have been conducted in patients with end-stage renal disease. ENTEREG is not recommended for use in these patients [see Use in Specific Populations (8.7)].
5.6 Risk of Serious Adverse Reactions in Patients with Complete Gastrointestinal Obstruction
No studies have been conducted in patients with complete gastrointestinal obstruction or in patients who have surgery for correction of complete bowel obstruction. ENTEREG is not recommended for use in these patients.
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Potential Risk of Myocardial Infarction with Long-Term Use [see Warnings and Precautions (5.1)]
- Gastrointestinal-Related Adverse Reactions in Opioid-Tolerant Patients [see Warnings and Precautions (5.3)]
- Risk of Serious Adverse Reactions in Patients with Severe Hepatic Impairment [see Warnings and Precautions (5.4)]
- Risk of Serious Adverse Reactions in Patients with Complete Gastrointestinal Obstruction [see Warnings and Precautions (5.6)]
- Risk of Serious Adverse Reactions in Pancreatic and Gastric Anastomoses [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be compared directly with rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. The adverse event information from clinical trials does, however, provide a basis for identifying the adverse events that appear to be related to drug use and for approximating rates.
The data described below reflect exposure to ENTEREG 12 mg in 1,793 patients in 10 placebo-controlled studies. The population was 19 to 97 years old, 64% were female, and 84% were Caucasian; 64% were undergoing a surgery that included bowel resection. The first dose of ENTEREG was administered 30 minutes to 5 hours before the scheduled start of surgery and then twice daily until hospital discharge (or for a maximum of 7 days of postoperative treatment).
Among ENTEREG-treated patients undergoing surgeries that included a bowel resection, the most common adverse reaction (incidence ≥1.5%) occurring with a higher frequency than placebo was dyspepsia (ENTEREG, 1.5%; placebo, 0.8%). Adverse reactions are events that occurred after the first dose of study medication treatment and within 7 days of the last dose of study medication or events present at baseline that increased in severity after the start of study medication treatment.
7. Drug Interactions
7.1 Effects of Alvimopan on Intravenous Morphine
Coadministration of alvimopan does not appear to alter the pharmacokinetics of morphine and its metabolite, morphine-6-glucuronide, to a clinically significant degree when morphine is administered intravenously. Dosage adjustment for intravenously administered morphine is not necessary when it is coadministered with ENTEREG.
7.2 Effects of Concomitant Acid Blockers or Antibiotics
A population pharmacokinetic analysis suggests that the pharmacokinetics of alvimopan were not affected by concomitant administration of acid blockers (proton pump inhibitors (PPIs), histamine-2 (H2) receptor antagonists) or antibiotics. No dosage adjustments are necessary in patients taking acid blockers or antibiotics with ENTEREG.
8. Use In Specific Populations
8.5 Geriatric Use
Of the total number of patients in 6 clinical efficacy studies treated with ENTEREG 12 mg or placebo, 46% were 65 years of age and over, while 18% were 75 years of age and over. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. No dosage adjustment based on increased age is required [see Clinical Pharmacology (12.3)].
8.6 Hepatic Impairment
ENTEREG is not recommended for use in patients with severe hepatic impairment.
Dosage adjustment is not required for patients with mild-to-moderate hepatic impairment. Patients with mild-to-moderate hepatic impairment should be closely monitored for possible adverse reactions (e.g., diarrhea, gastrointestinal pain, cramping) that could indicate high alvimopan or 'metabolite' concentrations, and ENTEREG should be discontinued if adverse reactions occur [see Warnings and Precautions (5.4), Clinical Pharmacology (12.3)].
8.7 Renal Impairment
ENTEREG is not recommended for use in patients with end-stage renal disease. Dosage adjustment is not required for patients with mild-to-severe renal impairment, but they should be monitored for adverse reactions. Patients with severe renal impairment should be closely monitored for possible adverse reactions (e.g., diarrhea, gastrointestinal pain, cramping) that could indicate high alvimopan or 'metabolite' concentrations, and ENTEREG should be discontinued if adverse reactions occur [see Clinical Pharmacology (12.3)].
8.8 Race/Ethnicity
No dosage adjustment is necessary in Black, Hispanic, and Japanese patients. However, the exposure to ENTEREG in Japanese healthy male subjects was approximately 2-fold greater than in Caucasian subjects. Japanese patients should be closely monitored for possible adverse reactions (e.g., diarrhea, gastrointestinal pain, cramping) that could indicate high alvimopan or 'metabolite' concentrations, and ENTEREG should be discontinued if adverse reactions occur [see Clinical Pharmacology (12.3)].
11. Entereg Description
ENTEREG capsules contain alvimopan, an opioid antagonist. Chemically, alvimopan is the single stereoisomer [[2(S)-[[4(R)-(3-hydroxyphenyl)-3(R),4-dimethyl-1-piperidinyl]methyl]-1-oxo-3-phenylpropyl]amino]acetic acid dihydrate. It has the following structural formula:
Alvimopan is a white to light beige powder with a molecular weight of 460.6, and the empirical formula is C25H32N2O4∙2H2O. It has a solubility of <0.1 mg/mL in water or buffered solutions between pH 3.0 and 9.0, 1 to 5 mg/mL in buffered solutions at pH 1.2, and 10 to 25 mg/mL in aqueous 0.1 N sodium hydroxide. At physiological pH, alvimopan is zwitterionic, a property that contributes to its low solubility.
ENTEREG capsules for oral administration contain 12 mg of alvimopan on an anhydrous basis suspended in the inactive ingredient polyethylene glycol.
12. Entereg - Clinical Pharmacology
12.1 Mechanism of Action
Alvimopan is a selective antagonist of the cloned human μ-opioid receptor with a Ki of 0.4 nM (0.2 ng/mL) and no measurable opioid-agonist effects in standard pharmacologic assays. The dissociation of [3H]-alvimopan from the human μ-opioid receptor is slower than that of other opioid ligands, consistent with its higher affinity for the receptor. At concentrations of 1 to 10 µM, alvimopan demonstrated no activity at any of over 70 non-opioid receptors, enzymes, and ion channels.
Postoperative ileus is the impairment of gastrointestinal motility after intra-abdominal surgery or other, non-abdominal surgeries. Postoperative ileus affects all segments of the gastrointestinal tract and may last from 5 to 6 days, or even longer. This may potentially delay gastrointestinal recovery and hospital discharge until its resolution. It is characterized by abdominal distention and bloating, nausea, vomiting, pain, accumulation of gas and fluids in the bowel, and delayed passage of flatus and defecation. Postoperative ileus is the result of a multifactorial process that includes inhibitory sympathetic input and release of hormones, neurotransmitters, and other mediators (e.g., endogenous opioids). A component of postoperative ileus also results from an inflammatory reaction and the effects of opioid analgesics. Morphine and other μ-opioid receptor agonists are universally used for the treatment of acute postsurgical pain; however, they are known to have an inhibitory effect on gastrointestinal motility and may prolong the duration of postoperative ileus.
Following oral administration, alvimopan antagonizes the peripheral effects of opioids on gastrointestinal motility and secretion by competitively binding to gastrointestinal tract μ-opioid receptors. The antagonism produced by alvimopan at opioid receptors is evident in isolated guinea pig ileum preparations in which alvimopan competitively antagonizes the effects of morphine on contractility. Alvimopan achieves this selective gastrointestinal opioid antagonism without reversing the central analgesic effects of μ-opioid agonists.
12.2 Pharmacodynamics
In an exploratory study in healthy subjects, alvimopan 12 mg administered twice a day reduced the delay in small and large bowel transit induced by codeine 30 mg administered 4 times a day, as measured by gastrointestinal scintigraphy. In the same study, concomitant alvimopan did not reduce the delay in gastric emptying induced by codeine.
12.3 Pharmacokinetics
Following oral administration of alvimopan, an amide hydrolysis compound is present in the systemic circulation, which is considered a product exclusively of intestinal flora metabolism. This compound is referred to as the 'metabolite'. It is also a mu-opioid receptor antagonist with a Ki of 0.8 nM (0.3 ng/mL).
14. Clinical Studies
The efficacy of ENTEREG in the management of postoperative ileus was evaluated in 6 multicenter, randomized, double-blind, parallel-group, placebo-controlled studies: 5 US studies (Studies 1-4 and 6) and 1 non–US study (Study 5). Patients 18 years of age or older undergoing partial large or small bowel resection surgery with primary anastomosis for colorectal or small bowel disease, total abdominal hysterectomy, or radical cystectomy for bladder cancer (in this procedure, resected segments of bowel are used for reconstruction of the urinary tract) under general anesthesia were randomly assigned to receive oral doses of ENTEREG 12 mg or matching placebo. The initial dose was administered at least 30 minutes and up to 5 hours prior to the scheduled start of surgery for most patients, and subsequent doses were administered twice daily beginning on the first postoperative day and continued until hospital discharge or a maximum of 7 days. There were no limitations on the type of general anesthesia used, but intrathecal or epidural opioids or anesthetics were prohibited.
All patients in the US studies were scheduled to receive intravenous patient-controlled opioid analgesia. In the non–US study, patients were scheduled to receive opioids either by intravenous patient-controlled opioid analgesia or bolus parenteral administration (intravenous or intramuscular). In all studies, there was no restriction on the type of opioid used or the duration of intravenous patient-controlled opioid analgesia. A standardized accelerated postoperative care pathway was implemented: early nasogastric tube removal (before the first postoperative dose); early ambulation (day following surgery); early diet advancement (liquids offered the day following surgery for patients undergoing bowel resection and by the third day following surgery for patients undergoing radical cystectomy; solids by the second day following surgery for patients undergoing bowel resection and by the fourth day following surgery for patients undergoing radical cystectomy), as tolerated.
Patients who received more than 3 doses of an opioid (regardless of route) during the 7 days prior to surgery and patients with complete bowel obstruction or who were scheduled for a total colectomy, colostomy, or ileostomy were excluded.
The primary endpoint for all studies was time to achieve resolution of postoperative ileus, a clinically defined composite measure of both upper and lower gastrointestinal recovery. Although both 2-component (GI2: toleration of solid food and first bowel movement) and 3-component (GI3: toleration of solid food and either first flatus or bowel movement) endpoints were used in all studies, GI2 is presented as it represents the most objective and clinically relevant measure of treatment response in patients undergoing surgeries that include a bowel resection. The time from the end of surgery to when the discharge order was written represented the length of hospital stay. In the 6 studies, 1,058 patients who underwent a surgery that included a bowel resection received placebo (not including 157 for total abdominal hysterectomy) and 1,096 patients received ENTEREG 12 mg (not including 143 for total abdominal hysterectomy).
The efficacy of ENTEREG following total abdominal hysterectomy has not been established. Therefore, the following data are presented only for surgeries that included a bowel resection (i.e., bowel resection or radical cystectomy).
Bowel Resection or Radical Cystectomy: A total of 2,154 patients underwent a surgery that included a bowel resection. The average age was 62 years, 54% were males, and 89% were Caucasian. The most common indications for surgery were colon or rectal cancer/malignancy, bladder cancer, and diverticular disease. In the non–US bowel resection study (Study 5), average daily postoperative opioid consumption was approximately 50% lower and the use of non-opioid analgesics substantially higher, as compared with the US bowel resection studies (Studies 1-4) for both treatment groups. During the first 48 hours postoperatively, the use of non-opioid analgesics was 69% compared with 4% for the non–US and US bowel resection studies, respectively. In each of the 6 studies, ENTEREG accelerated the time to recovery of gastrointestinal function, as measured by the composite endpoint GI2, and time to discharge order written as compared with placebo. Hazard ratios greater than 1 indicate a higher probability of achieving the event during the study period with treatment with ENTEREG than with placebo. Table 1 provides the Hazard Ratios, Kaplan Meier means, medians, and mean and median treatment differences (hours) in gastrointestinal recovery between ENTEREG and placebo.
| Study No.* | ENTEREG 12 mg | Placebo | Treatment Difference | Hazard Ratio (95% CI) |
|||
|---|---|---|---|---|---|---|---|
| Mean† | Median | Mean† | Median | Means† | Medians | ||
|
|||||||
| 1 | 92.0 | 80.0 | 111.8 | 96.6 | 19.8 | 16.6 | 1.533 (1.293, 1.816) |
| 2 | 105.9 | 98.0 | 132.0 | 115.2 | 26.1 | 17.2 | 1.625 (1.256, 2.102) |
| 3 | 116.4 | 101.8 | 130.3 | 116.8 | 14.0 | 15.0 | 1.365 (1.057, 1.764) |
| 4 | 106.7 | 101.4 | 119.9 | 113.3 | 13.2 | 11.9 | 1.400 (1.035, 1.894) |
| 5 | 98.2 | 92.8 | 108.8 | 95.9 | 10.6 | 3.1 | 1.299 (1.070, 1.575) |
| 6 | 132.7 | 117.0 | 164.2 | 145.6 | 31.5 | 28.5 | 1.773 (1.359, 2.311) |
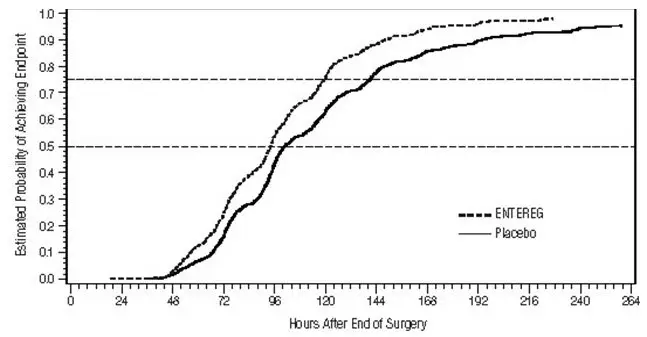
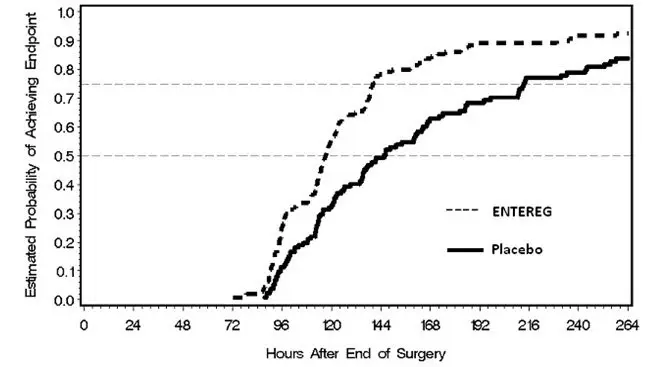
The Kaplan Meier estimate probabilities of patients receiving ENTEREG who achieved GI2 were numerically higher at all times throughout the study observation period compared with those of patients receiving placebo (see Figures 1 and 2).
| Figure 1: Time to GI2 Based on Results from Studies 1 through 5 |
|---|
 |
| Figure 2: Time to GI2 Based on Results from Study 6 |
|---|
 |
In Studies 1–4, the differences between ENTEREG and placebo patient groups in median time to 'discharge order written' ranged from 6 to 22 hours, in favor of ENTEREG patients. The group differences in mean time to 'discharge order written' ranged from 13 to 21 hours. In Study 6, the median time difference was 19 hours in favor of ENTEREG patients (mean time difference 22 hours).
ENTEREG did not reverse opioid analgesia as measured by visual analog scale pain intensity scores and/or amount of postoperative opioids administered across all 6 studies.
There were no sex-, age-, or race-related differences in treatment effect.
The incidence of anastomotic leak was low and comparable in patients receiving either ENTEREG or placebo (0.7% and 1.0%, respectively).
16. How is Entereg supplied
ENTEREG capsules, 12 mg, are blue, hard-gelatin capsules printed with "ADL2698" on both the body and the cap of the capsule. ENTEREG capsules are available in unit-dose packs of 30 capsules (30 doses) (NDC 67919-020-10) for hospital use only.

| ENTEREG
alvimopan capsule |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Merck Sharp & Dohme LLC (118446553) |
