Drug Detail:Nucala (Mepolizumab [ mep-oh-liz-ue-mab ])
Drug Class: Interleukin inhibitors
Highlights of Prescribing Information
NUCALA (mepolizumab) for injection, for subcutaneous use
NUCALA (mepolizumab) injection, for subcutaneous use
Initial U.S. Approval: 2015
Indications and Usage for Nucala
NUCALA is an interleukin-5 (IL-5) antagonist monoclonal antibody (IgG1 kappa) indicated for:
- •
- Add-on maintenance treatment of adult and pediatric patients aged 6 years and older with severe asthma and with an eosinophilic phenotype. (1.1)
- •
- Add-on maintenance treatment of adult patients 18 years and older with chronic rhinosinusitis with nasal polyps (CRSwNP). (1.2)
- •
- The treatment of adult patients with eosinophilic granulomatosis with polyangiitis (EGPA). (1.3)
- •
- The treatment of adult and pediatric patients aged 12 years and older with hypereosinophilic syndrome (HES) for ≥6 months without an identifiable non-hematologic secondary cause. (1.4)
Limitations of use: Not for relief of acute bronchospasm or status asthmaticus. (1.1)
Nucala Dosage and Administration
- •
- Severe asthma in patients aged 12 years and older: 100 mg administered subcutaneously once every 4 weeks. (2.1)
- •
- Severe asthma in patients aged 6 to 11 years: 40 mg administered subcutaneously once every 4 weeks. (2.1)
- •
- CRSwNP: 100 mg administered subcutaneously once every 4 weeks. (2.2)
- •
- EGPA: 300 mg as 3 separate 100-mg injections administered subcutaneously once every 4 weeks. (2.3)
- •
- HES: 300 mg as 3 separate 100-mg injections administered subcutaneously once every 4 weeks. (2.4)
Dosage Forms and Strengths
- •
- For injection: 100 mg of lyophilized powder in a single-dose vial for reconstitution. (3)
- •
- Injection: 100 mg/mL, single-dose prefilled autoinjector or single-dose prefilled syringe. (3)
- •
- Injection: 40 mg/0.4 mL, single-dose prefilled syringe. (3)
Contraindications
History of hypersensitivity to mepolizumab or excipients in the formulation. (4)
Warnings and Precautions
- •
- Hypersensitivity reactions (e.g., anaphylaxis, angioedema, bronchospasm, hypotension, urticaria, rash) have occurred after administration of NUCALA. Discontinue NUCALA in the event of a hypersensitivity reaction. (5.1)
- •
- Do not use to treat acute bronchospasm or status asthmaticus. (5.2)
- •
- Herpes zoster infections have occurred in patients receiving NUCALA. Consider vaccination if medically appropriate. (5.3)
- •
- Do not discontinue systemic or inhaled corticosteroids abruptly upon initiation of therapy with NUCALA. Decrease corticosteroids gradually, if appropriate. (5.4)
- •
- Treat patients with pre-existing helminth infections before therapy with NUCALA. If patients become infected while receiving treatment with NUCALA and do not respond to anti-helminth treatment, discontinue NUCALA until parasitic infection resolves. (5.5)
Adverse Reactions/Side Effects
Most common adverse reactions (incidence ≥5%):
- •
- Asthma: Headache, injection site reaction, back pain, and fatigue. (6.1)
- •
- CRSwNP: Oropharyngeal pain and arthralgia. (6.2)
- •
- EGPA and HES: Most common adverse reactions are similar to asthma. (6.3, 6.4)
To report SUSPECTED ADVERSE REACTIONS, contact GlaxoSmithKline at 1-888-825-5249 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 3/2023
Full Prescribing Information
1. Indications and Usage for Nucala
1.1 Maintenance Treatment of Severe Asthma
NUCALA is indicated for the add-on maintenance treatment of adult and pediatric patients aged 6 years and older with severe asthma and with an eosinophilic phenotype [see Use in Specific Populations (8.4), Clinical Studies (14.1)].
Limitations of Use
NUCALA is not indicated for the relief of acute bronchospasm or status asthmaticus.
1.2 Maintenance Treatment of Chronic Rhinosinusitis with Nasal Polyps
NUCALA is indicated for the add-on maintenance treatment of chronic rhinosinusitis with nasal polyps (CRSwNP) in adult patients 18 years of age and older with inadequate response to nasal corticosteroids.
2. Nucala Dosage and Administration
NUCALA is for subcutaneous use only.
2.1 Severe Asthma
Adults and Adolescents Aged 12 Years and Older
The recommended dosage of NUCALA in adults and adolescents aged 12 years and older is 100 mg administered once every 4 weeks by subcutaneous injection into the upper arm, thigh, or abdomen [see Dosage and Administration (2.5, 2.6)].
Pediatric Patients Aged 6 to 11 Years
The recommended dosage of NUCALA for injection in pediatric patients aged 6 to 11 years is 40 mg administered once every 4 weeks by subcutaneous injection into the upper arm, thigh, or abdomen [see Dosage and Administration (2.5, 2.6)].
2.2 Chronic Rhinosinusitis with Nasal Polyps
The recommended dosage of NUCALA is 100 mg administered once every 4 weeks by subcutaneous injection into the upper arm, thigh, or abdomen [see Dosage and Administration (2.5, 2.6)].
2.3 Eosinophilic Granulomatosis with Polyangiitis
The recommended dosage of NUCALA is 300 mg administered once every 4 weeks by subcutaneous injection as 3 separate 100-mg injections into the upper arm, thigh, or abdomen [see Dosage and Administration (2.5, 2.6)]. Administer individual 100-mg injections at least 5 cm (approximately 2 inches) apart.
2.4 Hypereosinophilic Syndrome
The recommended dosage of NUCALA is 300 mg administered once every 4 weeks by subcutaneous injection as 3 separate 100-mg injections into the upper arm, thigh, or abdomen [see Dosage and Administration (2.5, 2.6)]. Administer individual 100-mg injections at least 5 cm (approximately 2 inches) apart.
2.5 Preparation and Administration of NUCALA for Injection Vial
NUCALA for injection should be reconstituted and administered by a healthcare professional. In line with clinical practice, monitoring of patients after administration of biologic agents is recommended [see Warnings and Precautions (5.1)].
Reconstitution Instructions
- 1.
- Reconstitute NUCALA for injection in the vial with 1.2 mL of Sterile Water for Injection, USP, preferably using a 2- or 3-mL syringe and a 21-gauge needle. The reconstituted solution will contain a concentration of 100 mg/mL mepolizumab. Do not mix with other medications.
- 2.
- Direct the stream of Sterile Water for Injection vertically onto the center of the lyophilized powder, which may have a cake-like appearance. Gently swirl the vial for 10 seconds with a circular motion at 15-second intervals until the powder is dissolved.
Note: Do not shake the reconstituted solution during the procedure as this may lead to product foaming or precipitation. Reconstitution is typically complete within 5 minutes after the Sterile Water for Injection has been added, but it may take additional time. - 3.
- If a mechanical reconstitution device (swirler) is used to reconstitute NUCALA for injection, swirl at 450 rpm for no longer than 10 minutes. Alternatively, swirling at 1,000 rpm for no longer than 5 minutes is acceptable.
- 4.
- Visually inspect the reconstituted solution for particulate matter and clarity before use. The solution should be clear to opalescent and colorless to pale yellow or pale brown, essentially particle free. Small air bubbles, however, are expected and acceptable. If particulate matter remains in the solution or if the solution appears cloudy or milky, the solution must not be administered.
- 5.
- If the reconstituted solution is not used immediately:
- 1.
- store below 30°C (86°F),
- 2.
- do not freeze, and
- 3.
- discard if not used within 8 hours of reconstitution.
Administration of 100-mg Dose
- 1.
- For subcutaneous administration, preferably using a 1-mL polypropylene syringe fitted with a disposable 21- to 27-gauge x 0.5-inch (13-mm) needle.
- 2.
- Just before administration, remove 1 mL of reconstituted NUCALA for injection. Do not shake the reconstituted solution during the procedure as this could lead to product foaming or precipitation.
- 3.
- Administer the 1-mL injection (equivalent to 100 mg of mepolizumab) subcutaneously into the upper arm, thigh, or abdomen.
Administration of 40-mg Dose
- 1.
- For subcutaneous administration, preferably using a 1-mL polypropylene syringe fitted with a disposable 21- to 27-gauge x 0.5-inch (13-mm) needle.
- 2.
- Just before administration, remove 0.4 mL of reconstituted NUCALA for injection. Do not shake the reconstituted solution during the procedure as this could lead to product foaming or precipitation.
- 3.
- Administer the 0.4-mL injection (equivalent to 40 mg of mepolizumab) subcutaneously into the upper arm, thigh, or abdomen.
Each vial of NUCALA for injection should be used for a single patient, and any remainder of the contents should be discarded.
2.6 Preparation and Administration of NUCALA Injection Prefilled Autoinjector and Prefilled Syringes
NUCALA injection is intended for use under the guidance of a healthcare provider.
The 100-mg/mL prefilled autoinjector and 100-mg/mL prefilled syringe are only for use in adults and adolescents aged 12 years and older. A patient may self-inject or the patient caregiver may administer NUCALA injection 100 mg/mL subcutaneously after the healthcare provider determines it is appropriate.
The 40-mg/0.4-mL prefilled syringe is only for use in children aged 6 to 11 years and must be administered by the healthcare provider or the patient caregiver. The patient caregiver may administer NUCALA injection 40 mg/0.4 mL subcutaneously after the healthcare provider determines it is appropriate.
Provide proper training in subcutaneous injection technique and on the preparation and administration of NUCALA injection prior to use [see Instructions for Use].
- 1.
- Remove the prefilled autoinjector or prefilled syringe from the refrigerator and allow it to sit at room temperature for 30 minutes prior to injection. Do not warm NUCALA injection in any other way.
- 2.
- Prior to administration, visually inspect the window of the prefilled autoinjector or the prefilled syringe for particulate matter or discoloration. NUCALA injection should be clear to opalescent, colorless to pale yellow to pale brown in color. Do not use NUCALA injection if the product exhibits discoloration, cloudiness, or particulate matter. Do not use the NUCALA prefilled autoinjector or prefilled syringe if dropped on a hard surface.
- 3.
- Administer the subcutaneous injection into the thigh or abdomen, avoiding the 5 cm (approximately 2 inches) around the navel. The upper arm can also be used if a caregiver administers the subcutaneous injection.
- 4.
- For use in EGPA and HES, ensure injection sites for each subcutaneous injection are separated by at least 5 cm (approximately 2 inches).
- 5.
- Never give injections into areas where the skin is tender, bruised, red, or hard.
- 6.
- If a dose is missed, administer a dose as soon as possible. Thereafter, the patient can resume dosing on the usual day of administration. If the next dose is already due, then administer as planned.
3. Dosage Forms and Strengths
For injection
- •
- 100 mg white to off-white lyophilized powder in a single-dose vial for reconstitution.
Injection
- •
- 100 mg/mL as a clear to opalescent, colorless to pale yellow to pale brown solution in a single-dose prefilled autoinjector.
- •
- 100 mg/mL as a clear to opalescent, colorless to pale yellow to pale brown solution in a single-dose prefilled glass syringe.
- •
- 40 mg/0.4 mL as a clear to opalescent, colorless to pale yellow to pale brown solution in a single-dose prefilled glass syringe.
4. Contraindications
NUCALA is contraindicated in patients with a history of hypersensitivity to mepolizumab or excipients in the formulation [see Warnings and Precautions (5.1), Description (11)].
5. Warnings and Precautions
5.1 Hypersensitivity Reactions
Hypersensitivity reactions (e.g., anaphylaxis, angioedema, bronchospasm, hypotension, urticaria, rash) have occurred following administration of NUCALA. These reactions generally occur within hours of administration, but in some instances can have a delayed onset (i.e., days). In the event of a hypersensitivity reaction, NUCALA should be discontinued [see Contraindications (4)].
5.2 Acute Asthma Symptoms or Deteriorating Disease
NUCALA should not be used to treat acute asthma symptoms or acute exacerbations. Do not use NUCALA to treat acute bronchospasm or status asthmaticus. Patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with NUCALA.
5.3 Opportunistic Infections: Herpes Zoster
Herpes zoster has occurred in subjects receiving NUCALA 100 mg in controlled clinical trials [see Adverse Reactions (6.1)]. Consider vaccination if medically appropriate.
5.4 Reduction of Corticosteroid Dosage
Do not discontinue systemic or inhaled corticosteroids (ICS) abruptly upon initiation of therapy with NUCALA. Reductions in corticosteroid dosage, if appropriate, should be gradual and performed under the direct supervision of a physician. Reduction in corticosteroid dosage may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
5.5 Parasitic (Helminth) Infection
Eosinophils may be involved in the immunological response to some helminth infections. Patients with known parasitic infections were excluded from participation in clinical trials. It is unknown if NUCALA will influence a patient’s response against parasitic infections. Treat patients with pre-existing helminth infections before initiating therapy with NUCALA. If patients become infected while receiving treatment with NUCALA and do not respond to anti-helminth treatment, discontinue treatment with NUCALA until infection resolves.
6. Adverse Reactions/Side Effects
The following adverse reactions are described in greater detail in other sections:
- •
- Hypersensitivity reactions [see Warnings and Precautions (5.1)]
- •
- Opportunistic infections: herpes zoster [see Warnings and Precautions (5.3)]
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in practice.
6.1 Clinical Trials Experience in Severe Asthma
Adult and Adolescent Patients Aged 12 Years and Older
A total of 1,327 patients with severe asthma were evaluated in 3 randomized, placebo-controlled, multicenter trials of 24 to 52 weeks’ duration (Trial 1, NCT01000506; Trial 2, NCT01691521; and Trial 3, NCT01691508). Of these, 1,192 had a history of 2 or more exacerbations in the year prior to enrollment despite regular use of high-dose ICS plus additional controller(s) (Trials 1 and 2), and 135 patients required daily oral corticosteroids (OCS) in addition to regular use of high-dose ICS plus additional controller(s) to maintain asthma control (Trial 3). All patients had markers of eosinophilic airway inflammation [see Clinical Studies (14.1)]. Of the patients enrolled, 59% were female, 85% were White, and ages ranged from 12 to 82 years. Mepolizumab was administered subcutaneously or intravenously once every 4 weeks; 263 patients received NUCALA (mepolizumab 100 mg subcutaneous) for at least 24 weeks. Serious adverse events that occurred in more than 1 patient and in a greater percentage of patients receiving NUCALA 100 mg (n = 263) than placebo (n = 257) included 1 event, herpes zoster (2 patients vs. 0 patients, respectively). Approximately 2% of patients receiving NUCALA 100 mg withdrew from clinical trials due to adverse events compared with 3% of patients receiving placebo.
The incidence of adverse reactions in the first 24 weeks of treatment in the 2 confirmatory efficacy and safety trials (Trials 2 and 3) with NUCALA 100 mg is shown in Table 1.
|
Adverse Reaction |
NUCALA (Mepolizumab 100 mg Subcutaneous) (n = 263) % |
Placebo (n = 257) % |
|
Headache |
19 |
18 |
|
Injection site reaction |
8 |
3 |
|
Back pain |
5 |
4 |
|
Fatigue |
5 |
4 |
|
Influenza |
3 |
2 |
|
Urinary tract infection |
3 |
2 |
|
Abdominal pain upper |
3 |
2 |
|
Pruritus |
3 |
2 |
|
Eczema |
3 |
<1 |
|
Muscle spasms |
3 |
<1 |
52-Week Trial: Adverse reactions from Trial 1 with 52 weeks of treatment with mepolizumab 75 mg intravenous (IV) (n = 153) or placebo (n = 155) and with ≥3% incidence and more common than placebo and not shown in Table 1 were: abdominal pain, allergic rhinitis, asthenia, bronchitis, cystitis, dizziness, dyspnea, ear infection, gastroenteritis, lower respiratory tract infection, musculoskeletal pain, nasal congestion, nasopharyngitis, nausea, pharyngitis, pyrexia, rash, toothache, viral infection, viral respiratory tract infection, and vomiting. In addition, 3 cases of herpes zoster occurred in patients receiving mepolizumab 75 mg IV compared with 2 patients in the placebo group.
Systemic Reactions, including Hypersensitivity Reactions: In Trials 1, 2, and 3 described above, the percentage of patients who experienced systemic (allergic and non-allergic) reactions was 3% in the group receiving NUCALA 100 mg and 5% in the placebo group. Systemic allergic/hypersensitivity reactions were reported by 1% of patients in the group receiving NUCALA 100 mg and 2% of patients in the placebo group. The most commonly reported manifestations of systemic allergic/hypersensitivity reactions reported in the group receiving NUCALA 100 mg included rash, pruritus, headache, and myalgia. Systemic non-allergic reactions were reported by 2% of patients in the group receiving NUCALA 100 mg and 3% of patients in the placebo group. The most commonly reported manifestations of systemic non-allergic reactions reported in the group receiving NUCALA 100 mg included rash, flushing, and myalgia. A majority of the systemic reactions in patients receiving NUCALA 100 mg (5/7) were experienced on the day of dosing.
Injection Site Reactions: Injection site reactions (e.g., pain, erythema, swelling, itching, burning sensation) occurred at a rate of 8% in patients receiving NUCALA 100 mg compared with 3% in patients receiving placebo.
Long-term Safety: Nine hundred ninety-eight patients received NUCALA 100 mg in ongoing open-label extension studies, during which additional cases of herpes zoster were reported. The overall adverse event profile has been similar to the severe asthma trials described above.
Pediatric Patients Aged 6 to 11 Years
The safety data for NUCALA is based upon 1 open-label clinical trial that enrolled 36 patients with severe asthma aged 6 to 11 years. Patients received 40 mg (for those weighing <40 kg) or 100 mg (for those weighing ≥40 kg) of NUCALA administered subcutaneously once every 4 weeks. Patients received NUCALA for 12 weeks (initial short phase). After a treatment interruption of 8 weeks, 30 patients received NUCALA for a further 52 weeks (long phase). The adverse reaction profile for patients aged 6 to 11 years was similar to that observed in patients aged 12 years and older.
6.2 Clinical Trials Experience in Chronic Rhinosinusitis with Nasal Polyps
A total of 407 patients with CRSwNP were evaluated in 1 randomized, placebo-controlled, multicenter, 52-week treatment trial. Patients received NUCALA 100 mg or placebo subcutaneously once every 4 weeks. Patients had recurrent CRSwNP with a history of prior surgery and were on nasal corticosteroids for at least 8 weeks prior to screening [see Clinical Studies (14.2)]. Of the patients enrolled, 35% were female, 93% were White, and ages ranged from 18 to 82 years. Approximately 2% of patients receiving NUCALA 100 mg withdrew from study treatment due to adverse events compared with 2% of patients receiving placebo.
Table 2 summarizes adverse reactions that occurred in ≥3% of NUCALA-treated patients and more frequently than in patients treated with placebo in the CRSwNP trial.
| CRSwNP = Chronic Rhinosinusitis with Nasal Polyps. | ||
|
Adverse Reaction |
NUCALA (Mepolizumab 100 mg Subcutaneous) (n = 206) % |
Placebo (n = 201) % |
|
Oropharyngeal pain |
8 |
5 |
|
Arthralgia |
6 |
2 |
|
Abdominal pain upper |
3 |
2 |
|
Diarrhea |
3 |
2 |
|
Pyrexia |
3 |
2 |
|
Nasal dryness |
3 |
<1 |
|
Rash |
3 |
<1 |
Systemic Reactions, including Hypersensitivity Reactions
In the 52-week trial, the percentage of patients who experienced systemic (allergic [type I hypersensitivity] and other) reactions was <1% in the group receiving NUCALA 100 mg and <1% in the placebo group. Systemic allergic (type I hypersensitivity) reactions were reported by <1% of patients in the group receiving NUCALA 100 mg and no patients in the placebo group. The manifestations of systemic allergic (type I hypersensitivity) reactions included urticaria, erythema, and rash and 1 of the 3 reactions occurred on the day of dosing. Other systemic reactions were reported by no patients in the group receiving NUCALA 100 mg and <1% of patients in the placebo group.
Injection Site Reactions
Injection site reactions (e.g., erythema, pruritus) occurred at a rate of 2% in patients receiving NUCALA 100 mg compared with <1% in patients receiving placebo.
6.3 Clinical Trials Experience in Eosinophilic Granulomatosis with Polyangiitis
A total of 136 patients with EGPA were evaluated in 1 randomized, placebo-controlled, multicenter, 52-week treatment trial. Patients received 300 mg of NUCALA or placebo subcutaneously once every 4 weeks. Patients enrolled had a diagnosis of EGPA for at least 6 months prior to enrollment with a history of relapsing or refractory disease and were on a stable dosage of oral prednisolone or prednisone of greater than or equal to 7.5 mg/day (but not greater than 50 mg/day) for at least 4 weeks prior to enrollment [see Clinical Studies (14.3)]. Of the patients enrolled, 59% were female, 92% were White, and ages ranged from 20 to 71 years. No additional adverse reactions were identified to those reported in the severe asthma trials.
Systemic Reactions, including Hypersensitivity Reactions
In the 52-week trial, the percentage of patients who experienced systemic (allergic and non‑allergic) reactions was 6% in the group receiving 300 mg of NUCALA and 1% in the placebo group. Systemic allergic/hypersensitivity reactions were reported by 4% of patients in the group receiving 300 mg of NUCALA and 1% of patients in the placebo group. The manifestations of systemic allergic/hypersensitivity reactions reported in the group receiving 300 mg of NUCALA included rash, pruritus, flushing, fatigue, hypertension, warm sensation in trunk and neck, cold extremities, dyspnea, and stridor. Systemic non-allergic reactions were reported by 1 (1%) patient in the group receiving 300 mg of NUCALA and no patients in the placebo group. The reported manifestation of systemic non-allergic reactions reported in the group receiving 300 mg of NUCALA was angioedema. Half of the systemic reactions in patients receiving 300 mg of NUCALA (2/4) were experienced on the day of dosing.
Injection Site Reactions
Injection site reactions (e.g., pain, erythema, swelling) occurred at a rate of 15% in patients receiving 300 mg of NUCALA compared with 13% in patients receiving placebo.
6.4 Clinical Trials Experience in Hypereosinophilic Syndrome
A total of 108 adult and adolescent patients aged 12 years and older with HES were evaluated in a randomized, placebo‑controlled, multicenter, 32-week treatment trial. Patients with non-hematologic secondary HES or FIP1L1‑PDGFRα kinase-positive HES were excluded from the trial. Patients received 300 mg of NUCALA or placebo subcutaneously once every 4 weeks. Patients must have been on a stable dose of background HES therapy for the 4 weeks prior to randomization [see Clinical Studies (14.4)]. Of the patients enrolled, 53% were female, 93% were White, and ages ranged from 12 to 82 years. No additional adverse reactions were identified to those reported in the severe asthma trials.
Systemic Reactions, including Hypersensitivity Reactions
In the trial, no systemic allergic (type I hypersensitivity) reactions were reported. Other systemic reactions were reported by 1 (2%) patient in the group receiving 300 mg of NUCALA and no patients in the placebo group. The reported manifestation of other systemic reaction was multifocal skin reaction experienced on the day of dosing.
Injection Site Reactions
Injection site reactions (e.g., burning, itching) occurred at a rate of 7% in patients receiving 300 mg of NUCALA compared with 4% in patients receiving placebo.
6.5 Immunogenicity
In adult and adolescent patients with severe asthma receiving NUCALA 100 mg, 15/260 (6%) had detectable anti-mepolizumab antibodies. Neutralizing antibodies were detected in 1 patient with asthma receiving NUCALA 100 mg. Anti-mepolizumab antibodies slightly increased (approximately 20%) the clearance of mepolizumab. There was no evidence of a correlation between anti-mepolizumab antibody titers and change in eosinophil level. The clinical relevance of the presence of anti-mepolizumab antibodies is not known. In the clinical trial of children aged 6 to 11 years with severe asthma receiving NUCALA 40 or 100 mg, 2/35 (6%) had detectable anti‑mepolizumab antibodies during the initial short phase of the trial. No children had detectable anti-mepolizumab antibodies during the long phase of the trial.
In patients with CRSwNP receiving NUCALA 100 mg, 6/196 (3%) had detectable anti-mepolizumab antibodies. No neutralizing antibodies were detected in any patients with CRSwNP.
In patients with EGPA receiving 300 mg of NUCALA, 1/68 (<2%) had detectable anti-mepolizumab antibodies. No neutralizing antibodies were detected in any patients with EGPA.
In adult and adolescent patients with HES receiving 300 mg of NUCALA, 1/53 (2%) had detectable anti-mepolizumab antibodies. No neutralizing antibodies were detected in any patients with HES.
The reported frequency of anti-mepolizumab antibodies may underestimate the actual frequency due to lower assay sensitivity in the presence of high drug concentration. The data reflect the percentage of patients whose test results were positive for antibodies to mepolizumab in specific assays. The observed incidence of antibody positivity in an assay is highly dependent on several factors, including assay sensitivity and specificity, assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease.
6.6 Postmarketing Experience
In addition to adverse reactions reported from clinical trials, the following adverse reactions have been identified during postapproval use of NUCALA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. These events have been chosen for inclusion due to either their seriousness, frequency of reporting, or causal connection to NUCALA or a combination of these factors.
Immune System Disorders
Hypersensitivity reactions, including anaphylaxis.
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
The data on pregnancy exposure are insufficient to inform on drug-associated risk. Monoclonal antibodies, such as mepolizumab, are transported across the placenta in a linear fashion as pregnancy progresses; therefore, potential effects on a fetus are likely to be greater during the second and third trimester of pregnancy. In a prenatal and postnatal development study conducted in cynomolgus monkeys, there was no evidence of fetal harm with IV administration of mepolizumab throughout pregnancy at doses that produced exposures up to approximately 9 times the exposure at the maximum recommended human dose (MRHD) of 300 mg subcutaneous (see Data).
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Disease-Associated Maternal and/or Embryofetal Risk: In women with poorly or moderately controlled asthma, evidence demonstrates that there is an increased risk of preeclampsia in the mother and prematurity, low birth weight, and small for gestational age in the neonate. The level of asthma control should be closely monitored in pregnant women and treatment adjusted as necessary to maintain optimal control.
Data
Animal Data: In a prenatal and postnatal development study, pregnant cynomolgus monkeys received mepolizumab from gestation Days 20 to 140 at doses that produced exposures up to approximately 9 times that achieved with the MRHD (on an AUC basis with maternal IV doses up to 100 mg/kg once every 4 weeks). Mepolizumab did not elicit adverse effects on fetal or neonatal growth (including immune function) up to 9 months after birth. Examinations for internal or skeletal malformations were not performed. Mepolizumab crossed the placenta in cynomolgus monkeys. Concentrations of mepolizumab were approximately 2.4 times higher in infants than in mothers up to Day 178 postpartum. Levels of mepolizumab in milk were ≤0.5% of maternal serum concentration.
In a fertility, early embryonic, and embryofetal development study, pregnant CD-1 mice received an analogous antibody, which inhibits the activity of murine interleukin-5 (IL-5), at an IV dose of 50 mg/kg once per week throughout gestation. The analogous antibody was not teratogenic in mice. Embryofetal development of IL-5–deficient mice has been reported to be generally unaffected relative to wild-type mice.
8.2 Lactation
Risk Summary
There is no information regarding the presence of mepolizumab in human milk, the effects on the breastfed infant, or the effects on milk production. However, mepolizumab is a humanized monoclonal antibody (IgG1 kappa), and immunoglobulin G (IgG) is present in human milk in small amounts. Mepolizumab was present in the milk of cynomolgus monkeys postpartum following dosing during pregnancy [see Use in Specific Populations (8.1)]. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for NUCALA and any potential adverse effects on the breastfed infant from mepolizumab or from the underlying maternal condition.
8.4 Pediatric Use
Severe Asthma
The safety and effectiveness of NUCALA for severe asthma, and with an eosinophilic phenotype, have been established in pediatric patients aged 6 years and older.
Use of NUCALA in adolescents aged 12 to 17 years is supported by evidence from adequate and well-controlled trials in adults and adolescents. A total of 28 adolescents aged 12 to 17 years with severe asthma were enrolled in the Phase 3 asthma trials. Of these, 25 were enrolled in the 32-week exacerbation trial (Trial 2, NCT01691521) and had a mean age of 14.8 years. Patients had a history of 2 or more exacerbations in the previous year despite regular use of medium- or high-dose ICS plus additional controller(s) with or without OCS and had blood eosinophils of ≥150 cells/mcL at screening or ≥300 cells/mcL within 12 months prior to enrollment. [See Clinical Studies (14.1).] Patients had a reduction in the rate of exacerbations that trended in favor of NUCALA. Of the 19 adolescents who received NUCALA, 9 received 100 mg and the mean apparent clearance in these patients was 35% less than that of adults. The safety profile observed in adolescents was generally similar to that of the overall population in the Phase 3 studies [see Adverse Reactions (6.1)].
Use of NUCALA in pediatric patients aged 6 to 11 years with severe asthma, and with an eosinophilic phenotype, is supported by evidence from adequate and well-controlled trials in adults and adolescents with additional pharmacokinetic, pharmacodynamic, and safety data in children aged 6 to 11 years. A single open-label clinical trial (NCT02377427) was conducted in 36 children aged 6 to 11 years (mean age: 8.6 years, 31% female) with severe asthma. Enrollment criteria were the same as for adolescents in the 32-week exacerbation trial (Trial 2). Based upon the pharmacokinetic data from this trial, a dose of 40 mg subcutaneous every 4 weeks was determined to have similar exposure to adults and adolescents administered a dose of 100 mg subcutaneous [see Clinical Pharmacology (12.3)].
The effectiveness of NUCALA in pediatric patients aged 6 to 11 years is extrapolated from efficacy in adults and adolescents with support from pharmacokinetic analyses showing similar drug exposure levels for 40 mg administered subcutaneously every 4 weeks in children aged 6 to 11 years compared with adults and adolescents [see Clinical Pharmacology (12.3)]. The safety profile and pharmacodynamic response observed in this trial for children aged 6 to 11 years were similar to that seen in adults and adolescents [see Adverse Reactions (6.1), Clinical Pharmacology (12.2)].
The safety and effectiveness in pediatric patients aged younger than 6 years with severe asthma have not been established.
Chronic Rhinosinusitis with Nasal Polyps
The safety and effectiveness in patients aged younger than 18 years with CRSwNP have not been established.
Eosinophilic Granulomatosis with Polyangiitis
The safety and effectiveness in patients aged younger than 18 years with EGPA have not been established.
Hypereosinophilic Syndrome
The safety and effectiveness of NUCALA for HES have been established in adolescent patients aged 12 years and older. The safety and effectiveness in pediatric patients aged younger than 12 years with HES have not been established.
Use of NUCALA for this indication is supported by evidence from an adequate and well-controlled study (NCT02836496) in adults and adolescents and an open-label extension study (NCT03306043). One adolescent received NUCALA during the controlled study and this patient and an additional 3 adolescents received NUCALA during the open-label extension study [see Clinical Studies (14.4)]. The 1 adolescent treated with NUCALA in the 32-week trial did not have a HES flare or an adverse event reported. All adolescents received 300 mg of NUCALA for 20 weeks in the open-label extension.
8.5 Geriatric Use
Clinical trials of NUCALA did not include sufficient numbers of patients aged 65 years and older that received NUCALA (n = 79) to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitant disease or other drug therapy. Based on available data, no adjustment of the dosage of NUCALA in geriatric patients is necessary, but greater sensitivity in some older individuals cannot be ruled out.
10. Overdosage
There is no specific treatment for an overdose with mepolizumab. If overdose occurs, the patient should be treated supportively with appropriate monitoring as necessary.
11. Nucala Description
Mepolizumab is a humanized IL-5 antagonist monoclonal antibody. Mepolizumab is produced by recombinant DNA technology in Chinese hamster ovary cells. Mepolizumab has a molecular weight of approximately 149 kDa.
NUCALA for injection is a sterile, preservative-free, white to off-white, lyophilized powder in a single-dose vial for subcutaneous injection after reconstitution. Upon reconstitution with 1.2 mL of Sterile Water for Injection, USP, the resulting concentration is 100 mg/mL and delivers 1 mL [see Dosage and Administration (2.5)]. Each vial delivers 100 mg of mepolizumab, polysorbate 80 (0.67 mg), sodium phosphate dibasic heptahydrate (7.14 mg), and sucrose (160 mg), with a pH of 7.0.
The vial stopper is not made with natural rubber latex.
NUCALA injection is a sterile, preservative-free, clear to opalescent, colorless to pale yellow to pale brown solution for subcutaneous use.
NUCALA injection is supplied in a single-dose, 1-mL, prefilled autoinjector with a fixed 29‑gauge, half-inch needle and in a single-dose, 1-mL, prefilled syringe with a fixed 29‑gauge, half-inch needle with a needle guard. Each 1 mL delivers 100 mg mepolizumab, citric acid monohydrate (0.95 mg), EDTA disodium dihydrate (0.019 mg), polysorbate 80 (0.20 mg), sodium phosphate dibasic heptahydrate (4.16 mg), and sucrose (120 mg), with a pH of 6.3.
NUCALA injection is supplied in a single-dose, 0.4-mL, prefilled syringe with a fixed 29-gauge, half-inch needle with a needle guard. Each 0.4 mL delivers 40 mg mepolizumab, citric acid monohydrate (0.38 mg), EDTA disodium dihydrate (0.0074 mg), polysorbate 80 (0.08 mg), sodium phosphate dibasic heptahydrate (1.66 mg), and sucrose (48 mg), with a pH of 6.3.
The prefilled autoinjector and prefilled syringe are not made with natural rubber latex.
12. Nucala - Clinical Pharmacology
12.1 Mechanism of Action
Mepolizumab is an IL-5 antagonist (IgG1 kappa). IL-5 is the major cytokine responsible for the growth and differentiation, recruitment, activation, and survival of eosinophils. Mepolizumab binds to IL-5 with a dissociation constant of 100 pM, inhibiting the bioactivity of IL-5 by blocking its binding to the alpha chain of the IL-5 receptor complex expressed on the eosinophil cell surface. Inflammation is an important component in the pathogenesis of asthma, CRSwNP, EGPA, and HES. Multiple cell types (e.g., mast cells, eosinophils, neutrophils, macrophages, lymphocytes) and mediators (e.g., histamine, eicosanoids, leukotrienes, cytokines) are involved in inflammation. Mepolizumab, by inhibiting IL-5 signaling, reduces the production and survival of eosinophils; however, the mechanism of mepolizumab action in asthma, CRSwNP, EGPA, and HES has not been definitively established.
12.2 Pharmacodynamics
The pharmacodynamic response (blood eosinophil reduction) following repeat doses of mepolizumab administered subcutaneously or intravenously was evaluated in adult subjects with asthma and blood eosinophil levels >200 cells/mcL. Subjects received 1 of 4 mepolizumab treatments (administered every 28 days for a total of 3 doses): 12.5 mg subcutaneous, 125 mg subcutaneous, 250 mg subcutaneous, or 75 mg IV. Sixty-six of the 70 randomized subjects completed the trial. Compared with baseline levels, blood eosinophils decreased in a dose-dependent manner. A reduction in blood eosinophil levels was observed in all treatment groups by Day 3 (48 hours post-dose). On Day 84 (4 weeks post‑last dose), the observed geometric mean reduction from baseline in blood eosinophils was 64%, 78%, 84%, and 90% in the 12.5-mg subcutaneous, 75-mg IV, 125-mg subcutaneous, and 250-mg subcutaneous treatment groups, respectively. The model-predicted subcutaneous doses providing 50% and 90% of maximal reduction of blood eosinophils at Day 84 were estimated to be 11 and 99 mg, respectively. These results, along with the clinical efficacy data from the dose-ranging exacerbation trial in adult and adolescent subjects with severe asthma (Trial 1) supported the evaluation of mepolizumab 75 mg IV and 100 mg subcutaneous in the confirmatory severe asthma trials [see Clinical Studies (14.1)]. Following subcutaneous administration of mepolizumab 100 mg every 4 weeks for 32 weeks in adult and adolescent subjects with severe asthma (Trial 2), blood eosinophils were reduced to a geometric mean count of 40 cells/mcL, which corresponds to a geometric mean reduction of 84% compared with placebo.
The pharmacodynamic response (blood eosinophil reduction) was also evaluated in children aged 6 to 11 years with severe asthma. Following subcutaneous administration of mepolizumab 40 mg every 4 weeks for 52 weeks, blood eosinophils were reduced to a geometric mean count of 48 cells/mcL. This corresponds to a geometric mean reduction from baseline of 85%.
The magnitude of reduction in adults, adolescents, and children was observed within 4 weeks of treatment and was maintained throughout the treatment periods.
For adults with CRSwNP, following subcutaneous administration of mepolizumab 100 mg every 4 weeks for 52 weeks, blood eosinophils were reduced to a geometric mean count of 60 cells/mcL. There was a geometric mean reduction of 83% compared with placebo. This magnitude of reduction was observed within 4 weeks of treatment and was maintained throughout the treatment period [see Clinical Studies (14.2)].
For adults with EGPA, following subcutaneous administration of mepolizumab 300 mg every 4 weeks for 52 weeks, blood eosinophils were reduced to a geometric mean count of 38 cells/mcL. There was a geometric mean reduction of 83% compared with placebo, and this magnitude of reduction was observed within 4 weeks of treatment [see Clinical Studies (14.3)].
For adults and adolescents with HES, following subcutaneous administration of mepolizumab 300 mg every 4 weeks for 32 weeks, blood eosinophils were reduced to a geometric mean count of 70 cells/mcL. There was a geometric mean reduction of 92% compared with placebo [see Clinical Studies (14.4)].
12.3 Pharmacokinetics
Following subcutaneous dosing in adult subjects with asthma, mepolizumab exhibited approximately dose‑proportional pharmacokinetics over a dose range of 12.5 to 250 mg. The pharmacokinetic properties of mepolizumab observed in subjects with CRSwNP (adults), EGPA (adults), or HES (adults and adolescents) were similar to the pharmacokinetic properties observed in subjects with severe asthma (adults and adolescents).
Subcutaneous administration of mepolizumab 300 mg had approximately 3 times the systemic exposure of mepolizumab 100 mg.
Absorption
Following 100-mg subcutaneous administration in the upper arm of adult and adolescent subjects with asthma, the bioavailability of mepolizumab was estimated to be approximately 80%.
Following repeat subcutaneous administration once every 4 weeks, there was approximately a 2-fold accumulation at steady state.
Distribution
The population central volume of distribution of mepolizumab in adult subjects with asthma is estimated to be 3.6 L for a 70-kg individual.
Elimination
Following subcutaneous administration of mepolizumab in adult subjects with asthma, the mean terminal half-life (t1/2) ranged from 16 to 22 days. The population apparent systemic clearance of mepolizumab in adult and adolescent subjects with asthma is estimated to be 0.28 L/day for a 70-kg individual.
Metabolism: Mepolizumab is a humanized IgG1 monoclonal antibody that is degraded by the proteolytic enzymes widely distributed in the body and not restricted to hepatic tissue.
Specific Populations
Racial Groups and Male and Female Patients: Population pharmacokinetics analyses indicated there was no significant effect of race and gender on mepolizumab clearance.
Age: Population pharmacokinetics analyses indicated there was no significant effect of age on mepolizumab clearance.
Pediatric Patients: Mepolizumab pharmacokinetics following subcutaneous administration in subjects aged 6 to 11 years with severe asthma was investigated in the initial 12-week treatment phase of an open-label clinical trial. Exposures (AUC) following subcutaneous administration of either 40 mg (for children weighing <40 kg) or 100 mg (for children weighing ≥40 kg) were 1.32 and 1.97 times higher, respectively, compared with that observed in adults and adolescents receiving 100 mg. Based on these results, simulation of a 40-mg subcutaneous dose every 4 weeks in children aged 6 to 11 years, irrespective of body weight, resulted in predicted exposures similar to that observed in adults and adolescents.
Patients with Renal Impairment: No clinical trials have been conducted to investigate the effect of renal impairment on the pharmacokinetics of mepolizumab. Based on population pharmacokinetic analyses, mepolizumab clearance was comparable between subjects with creatinine clearance values between 50 and 80 mL/min and patients with normal renal function. There are limited data available in subjects with creatinine clearance values <50 mL/min; however, mepolizumab is not cleared renally.
Patients with Hepatic Impairment: No clinical trials have been conducted to investigate the effect of hepatic impairment on the pharmacokinetics of mepolizumab. Since mepolizumab is degraded by widely distributed proteolytic enzymes, not restricted to hepatic tissue, changes in hepatic function are unlikely to have any effect on the elimination of mepolizumab.
Drug Interaction Studies
No formal drug interaction studies have been conducted with mepolizumab. In population pharmacokinetics analyses of Phase 3 studies, there was no evidence of an effect of commonly coadministered small molecule drugs on mepolizumab exposure.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term animal studies have not been performed to evaluate the carcinogenic potential of mepolizumab. Published literature using animal models suggests that IL-5 and eosinophils are part of an early inflammatory reaction at the site of tumorigenesis and can promote tumor rejection. However, other reports indicate that eosinophil infiltration into tumors can promote tumor growth. Therefore, the malignancy risk in humans from an antibody to IL-5 such as mepolizumab is unknown.
Male and female fertility were unaffected based upon no adverse histopathological findings in the reproductive organs from cynomolgus monkeys receiving mepolizumab for 6 months at IV dosages up to 100 mg/kg once every 4 weeks (approximately 20 times the MRHD of 300 mg on an AUC basis). Mating and reproductive performance were unaffected in male and female CD-1 mice receiving an analogous antibody, which inhibits the activity of murine IL-5, at an IV dosage of 50 mg/kg once per week.
14. Clinical Studies
14.1 Severe Asthma
The asthma development program for NUCALA in patients aged 12 years and older included 3 double-blind, randomized, placebo-controlled trials: 1 dose-ranging and exacerbation trial (Trial 1, NCT01000506) and 2 confirmatory trials (Trial 2, NCT01691521 and Trial 3, NCT01691508). Mepolizumab was administered every 4 weeks in all 3 trials as add-on to background treatment. All patients continued their background asthma therapy throughout the duration of the trials.
Dose-Ranging and Exacerbation Trial
Trial 1 was a 52-week dose-ranging and exacerbation-reduction trial in patients with severe asthma with a history of 2 or more exacerbations in the previous year despite regular use of high-dose ICS plus additional controller(s) with or without OCS. Patients enrolled in this trial were required to have at least 1 of the following 4 pre-specified criteria in the previous 12 months: blood eosinophil count ≥300 cells/mcL, sputum eosinophil count ≥3%, exhaled nitric oxide concentration ≥50 ppb, or deterioration of asthma control after ≤25% reduction in regular maintenance ICS/OCS. Three IV dosages of mepolizumab (75, 250, and 750 mg) administered once every 4 weeks were evaluated compared with placebo. Results from this trial and the pharmacodynamic study supported the evaluation of mepolizumab 75 mg IV and 100 mg subcutaneous in the subsequent trials [see Clinical Pharmacology (12.2)]. NUCALA is not indicated for IV use and should only be administered by the subcutaneous route.
Confirmatory Trials
A total of 711 patients with severe asthma were studied in the 2 confirmatory trials (Trials 2 and 3). In these 2 trials patients were required to have blood eosinophils of ≥150 cells/mcL at screening (within 6 weeks of dosing) or blood eosinophils of ≥300 cells/mcL within 12 months of enrollment. The screening blood eosinophils of ≥150 cells/mcL criterion was derived from exploratory analyses of data from Trial 1. Trial 2 was a 32-week placebo- and active-controlled trial in patients with severe asthma with a history of 2 or more exacerbations in the previous year despite regular use of high-dose ICS plus additional controller(s) with or without OCS. Patients received mepolizumab 75 mg IV (n = 191), NUCALA 100 mg (n = 194), or placebo (n = 191) once every 4 weeks for 32 weeks.
Trial 3 was a 24-week OCS-reduction trial in patients with severe asthma who required daily OCS in addition to regular use of high-dose ICS plus additional controller(s) to maintain asthma control. Patients in Trial 3 were not required to have a history of exacerbations in the previous year. Patients received NUCALA 100 mg (n = 69) or placebo (n = 66) once every 4 weeks for 24 weeks. The baseline mean OCS use was similar in the 2 treatment groups: 13.2 mg in the placebo group and 12.4 mg in the group receiving NUCALA 100 mg.
The demographics and baseline characteristics of these 3 trials are provided in Table 3.
| FEV1 = forced expiratory volume in 1 second, SABA = short-acting beta2-agonist, FVC = forced vital capacity. | |||
|
Trial 1 (N = 616) |
Trial 2 (N = 576) |
Trial 3 (N = 135) |
|
|
Mean age, years |
49 |
50 |
50 |
|
Female, n (%) |
387 (63) |
328 (57) |
74 (55) |
|
White, n (%) |
554 (90) |
450 (78) |
128 (95) |
|
Duration of asthma, years, mean |
19 |
20 |
19 |
|
Never smoked, n (%) |
483 (78) |
417 (72) |
82 (61) |
|
Baseline FEV1, L |
1.88 |
1.82 |
1.95 |
|
Baseline % predicted FEV1 |
60 |
61 |
59 |
|
Baseline % reversibility |
25 |
27 |
26 |
|
Baseline post-SABA FEV1/FVC |
0.67 |
0.66 |
0.66 |
|
Geometric mean eosinophil count at baseline, cells/mcL |
250 |
290 |
240 |
|
Mean number of exacerbations in previous year |
3.6 |
3.6 |
3.1 |
Exacerbations
Efficacy was assessed in Trials 1 and 2 using an endpoint of the frequency of exacerbations defined as worsening of asthma requiring use of oral/systemic corticosteroids and/or hospitalization and/or emergency department visits. For patients on maintenance OCS, an exacerbation requiring OCS was defined as the use of oral/systemic corticosteroids at least double the existing dose for at least 3 days. Compared with placebo, patients receiving NUCALA 100 mg or mepolizumab 75 mg IV experienced significantly fewer exacerbations. Additionally, compared with placebo, there were fewer exacerbations requiring hospitalization and/or emergency department visits and exacerbations requiring only in-patient hospitalization with NUCALA 100 mg (Table 4).
| IV = intravenous, SC = subcutaneous. | ||||||||
|
Trial |
Treatment |
Exacerbations per Year |
||||||
|
Rate |
Difference |
Rate Ratio (95% CI) |
||||||
|
All exacerbations |
||||||||
|
Trial 1 |
Placebo (n = 155) |
2.40 | ||||||
|
Mepolizumab 75 mg IV (n = 153) |
1.24 |
1.16 |
0.52 (0.39, 0.69) |
|||||
|
Trial 2 |
Placebo (n = 191) |
1.74 | ||||||
|
Mepolizumab 75 mg IV (n = 191) |
0.93 |
0.81 |
0.53 (0.40, 0.72) |
|||||
|
NUCALA 100 mg SC (n = 194) |
0.83 |
0.91 |
0.47 (0.35, 0.64) |
|||||
|
Exacerbations requiring hospitalization/emergency room visit |
||||||||
|
Trial 1 |
Placebo (n = 155) |
0.43 | ||||||
|
Mepolizumab 75 mg IV (n = 153) |
0.17 |
0.26 |
0.40 (0.19, 0.81) |
|||||
|
Trial 2 |
Placebo (n = 191) |
0.20 | ||||||
|
Mepolizumab 75 mg IV (n = 191) |
0.14 |
0.06 |
0.68 (0.33, 1.41) |
|||||
|
NUCALA 100 mg SC (n = 194) |
0.08 |
0.12 |
0.39 (0.18, 0.83) |
|||||
|
Exacerbations requiring hospitalization |
||||||||
|
Trial 1 |
Placebo (n = 155) |
0.18 | ||||||
|
Mepolizumab 75 mg IV (n = 153) |
0.11 |
0.07 |
0.61 (0.28, 1.33) |
|||||
|
Trial 2 |
Placebo (n = 191) |
0.10 | ||||||
|
Mepolizumab 75 mg IV (n = 191) |
0.06 |
0.04 |
0.61 (0.23, 1.66) |
|||||
|
NUCALA 100 mg SC (n = 194) |
0.03 |
0.07 |
0.31 (0.11, 0.91) |
|||||
The time to first exacerbation was longer for the groups receiving NUCALA 100 mg and mepolizumab 75 mg IV compared with placebo in Trial 2 (Figure 1).
Figure 1. Kaplan-Meier Cumulative Incidence Curve for Time to First Exacerbation (Severe Asthma Trial 2)
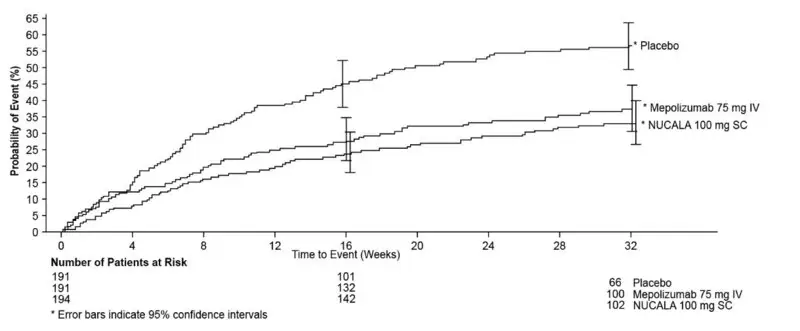
IV = intravenous, SC = subcutaneous.
Trial 1 data were explored to determine criteria that could identify patients likely to benefit from treatment with NUCALA. The exploratory analysis suggested that baseline blood eosinophil count of ≥150 cells/mcL was a potential predictor of treatment benefit. Exploratory analysis of Trial 2 data also suggested that baseline blood eosinophil count (obtained within 6 weeks of initiation of dosing) of ≥150 cells/mcL was a potential predictor of efficacy and showed a trend of greater exacerbation benefit with increasing blood eosinophil count. In Trial 2, patients enrolled solely on the basis of the historical blood eosinophil count of ≥300 cells/mcL in the previous 12 months, but who had a baseline blood eosinophil count <150 cells/mcL, had virtually no exacerbation benefit following treatment with NUCALA 100 mg compared with placebo.
The Asthma Control Questionnaire-5 (ACQ-5) was assessed in Trials 1 and 2, and the St. George’s Respiratory Questionnaire (SGRQ) was assessed in Trial 2. In Trial 1, the ACQ-5 responder rate (defined as a decrease in score of 0.5 or more as threshold) for the 75-mg IV mepolizumab arm was 47% compared with 50% for placebo with an odds ratio (OR) of 1.1 (95% CI: 0.7, 1.7). In Trial 2, the ACQ-5 responder rate for the treatment arm for NUCALA 100 mg was 57% compared with 45% for placebo with an OR of 1.8 (95% CI: 1.2, 2.8). In Trial 2, the SGRQ responder rate (defined as a decrease in score of 4 or more as threshold) for the treatment arm for NUCALA 100 mg was 71% compared with 55% for placebo with an OR of 2.1 (95% CI: 1.3, 3.2).
Oral Corticosteroid Reduction
Trial 3 evaluated the effect of NUCALA 100 mg on reducing the use of maintenance OCS. Efficacy was assessed using an endpoint of the percent reduction of OCS dose during Weeks 20 to 24 compared with baseline dose, while maintaining asthma control. Patients were classified according to their change in OCS use during the trial with the following categories: 90% to 100% decrease, 75% to <90% decrease, 50% to <75% decrease, >0% to <50% decrease, and no improvement (i.e., no change or any increase or lack of asthma control or withdrawal of treatment). Compared with placebo, patients receiving NUCALA 100 mg achieved greater reductions in daily maintenance OCS dose, while maintaining asthma control. Sixteen (23%) patients in the group receiving NUCALA 100 mg versus 7 (11%) in the placebo group had a 90% to 100% reduction in their OCS dose. Twenty-five (36%) patients in the group receiving NUCALA 100 mg versus 37 (56%) in the placebo group were classified as having no improvement for OCS dose. Additionally, 54% of patients receiving NUCALA 100 mg achieved at least a 50% reduction in the daily prednisone dose compared with 33% of patients receiving placebo (95% CI for difference: 4%, 37%). An exploratory analysis was also performed on the subgroup of 29 patients in Trial 3 who had an average baseline and screening blood eosinophil count <150 cells/mcL. Five (29%) patients in the group receiving NUCALA 100 mg versus 0 (0%) in the placebo group had a 90% to 100% reduction in their dose. Four (24%) patients in the group receiving NUCALA 100 mg versus 8 (67%) in the placebo group were classified as having no improvement for OCS dose. The ACQ and SGRQ were also assessed in Trial 3 and showed results similar to those in Trial 2.
Lung Function
Change from baseline in mean forced expiratory volume in 1 second (FEV1) was measured in all 3 trials and is presented in Table 5. Compared with placebo, NUCALA 100 mg did not provide consistent improvements in mean change from baseline in FEV1.
| FEV1 = forced expiratory volume in 1 second. a Dose = 75 mg intravenous. b Forced expiratory volume in 1 second (FEV1) at Week 52. c Dose = 100 mg subcutaneous. d FEV1 at Week 32. |
||||||||||||
|
Trial |
Difference from Placebo in Mean Change from
|
|||||||||||
|
Week 12 |
Week 24 |
Weeks 32/52 |
||||||||||
|
1a |
10 (-87, 108) |
5 (-98, 108) |
61 (-39, 161)b |
|||||||||
|
2c |
52 (-30, 134) |
76 (-6, 159) |
98 (11, 184)d |
|||||||||
|
3c |
56 (-91, 203) |
114 (-42, 271) |
NA |
|||||||||
The effect of mepolizumab on lung function was also studied in a 12-week placebo-controlled trial enrolling patients with asthma on a moderate dose of ICS with evidence of symptoms and lung function impairment. Enrollment was not dependent on a history of exacerbations or a pre-specified eosinophil count. Change from baseline in FEV1 at Week 12 was numerically lower in the mepolizumab treatment groups than the placebo group.
14.2 Chronic Rhinosinusitis with Nasal Polyps
A total of 407 adult patients with CRSwNP were evaluated in a randomized, double‑blind, placebo-controlled, multicenter, 52-week trial (NCT03085797). Patients received NUCALA 100 mg or placebo administered subcutaneously once every 4 weeks while continuing nasal corticosteroid therapy. Patients must have received background nasal corticosteroid for ≥8 weeks pre‑screening. Patients had recurrent and symptomatic CRSwNP, and had at least 1 surgery for the removal of nasal polyps within the previous 10 years. Patients were required to have nasal obstruction symptoms with a visual analog scale (VAS) score of >5 out of a maximum score of 10. Patients were also required to have an endoscopic bilateral nasal polyp score (NPS) of ≥5 out of 8 with NPS ≥2 in each nasal cavity. Patients reported nasal obstruction VAS scores daily by placing a single mark on a continuous line labeled from 0 (none) to 100 (as bad as you can imagine). The distance along the line was converted to a 0 to 10 point scale for scoring. For NPS, polyps on each side of the nose were graded on a categorical scale (0 = no polyps, 1 = small polyps in the middle meatus not reaching below the inferior border of the middle concha, 2 = polyps reaching below the lower border of the middle turbinate, 3 = large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle concha, 4 = large polyps causing almost complete congestion/obstruction of the inferior meatus) for a total score of 0 to 8. Sinus CT scans were not performed at baseline nor during treatment to evaluate for sinus opacification.
The co-primary endpoints were change from baseline to Week 52 in total endoscopic NPS (0 to 8 scale) as graded by independent blinded assessors and change from baseline in nasal obstruction VAS score (0 to 10 scale) during Weeks 49 to 52. The key secondary endpoint was the time to first nasal surgery (nasal polypectomy) up to Week 52 in this trial. Other secondary endpoints were change from baseline in loss of smell VAS score during Weeks 49 to 52, and proportion of patients requiring systemic steroids for nasal polyps up to Week 52. All VAS scores were collected daily by the patients and reported on a 0 to 10 scale (0 = none, 10 = as bad as you can imagine).
The demographics and baseline characteristics of patients in this trial are provided in Table 6.
| CRSwNP = Chronic Rhinosinusitis with Nasal Polyps, SD = standard deviation, OCS = oral corticosteroid, NPS = nasal polyp score, VAS = visual analog scale, AERD = aspirin-exacerbated respiratory disease. a As graded by independent blinded assessors. |
|
|
N = 407 |
|
|
Mean age, years |
49 |
|
Female, n (%) |
143 (35) |
|
White, n (%) |
379 (93) |
|
Mean CRSwNP duration in years (SD) |
11.4 (8.4) |
|
Patients with ≥1 surgery in past 10 years (%) |
407 (100) |
|
Patients with ≥3 surgeries in past 10 years (%) |
124 (30) |
|
OCS use (≥1 course) in past 12 months, n (%) |
197 (48) |
|
Mean bilateral endoscopic NPSa, (SD), range 0-8 |
5.5 (1.29) |
|
Mean nasal obstruction VAS score, (SD), range 0-10 |
9.0 (0.83) |
|
Geometric mean blood eosinophil cells/mcL (95% CI) |
390 (360, 420) |
|
Asthma, n (%) |
289 (71) |
|
AERD, n (%) |
108 (27) |
Endoscopic Nasal Polyp Score and Nasal Obstruction Visual Analog Scale Scores
Patients who received NUCALA 100 mg had a statistically significant improvement (decrease) in bilateral NPS at Week 52 and nasal obstruction VAS score from Weeks 49 to 52 at the end of the 52 week treatment period (Table 7).
| CRSwNP = Chronic Rhinosinusitis with Nasal Polyps, SD = standard deviation, SE = standard error, NPS = nasal polyp score at Week 52. a Patients with nasal surgery were assigned worst possible score for the period after nasal surgery. Missing data were imputed based on available off-treatment data across treatment arms. Imputations were made stepwise by visit and conditioned on data from previous visits with the same covariates used in the analysis model. b Least square means from analysis using mixed model repeated measures with covariates of treatment group, geographic region, baseline score, and log(e) baseline blood eosinophil count, visit, interaction terms for visit by baseline and visit by treatment. |
|||||||
|
Scoresa (range) |
Placebo n = 201 |
NUCALA 100 mg n = 206 |
Mean Difference vs. Placebo
|
||||
|
Baseline Mean (SD) |
Mean Changeb (SE) |
Baseline Mean (SD) |
Mean Changeb (SE) |
||||
|
NPS (0-8) |
5.6 (1.41) |
0.06 (0.14) |
5.4 (1.17) |
-0.87 (0.14) |
-0.93 (-1.31, -0.55) |
||
|
Nasal obstruction (0-10) |
9.02 (0.83) |
-2.54 (0.25) |
8.92 (0.83) |
-4.40 (0.25) |
-1.86 (-2.53, -1.19) |
||
Nasal Polypectomy
The key secondary endpoint was the time to first nasal surgery (nasal polypectomy) up to Week 52. The proportion of patients who had surgery was significantly reduced by 57% (hazard ratio: 0.43, 95% CI: 0.25, 0.76) in the group treated with NUCALA 100 mg compared with the placebo group (Figure 2). By Week 52, 18 (9%) patients who received NUCALA 100 mg had surgery compared with 46 (23%) patients in the placebo group.
Figure 2. Kaplan-Meier Plot of Time to First Nasal Surgery in CRSwNP
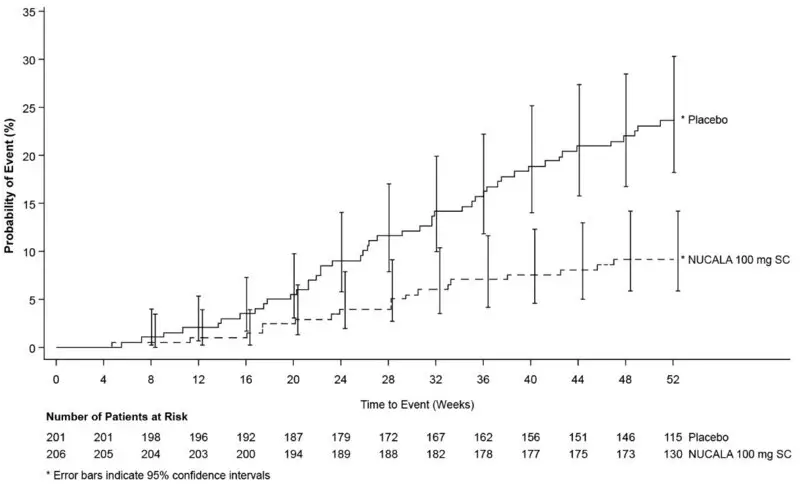
CRSwNP = Chronic Rhinosinusitis with Nasal Polyps, SC = subcutaneous.
Additional CRSwNP Symptoms Scores
For patients who received NUCALA 100 mg, statistically significant improvement was observed in loss of smell compared to placebo and improvements were also observed in the individual VAS symptom scores compared with patients in the placebo group in the 4-weeks prior to the end of the 52-week treatment period (Table 8).
| VAS = visual analog scale; SD = standard deviation; SE = standard error. a Patients with nasal surgery were assigned the worst possible score for the period after nasal surgery. Missing data was imputed based on available off-treatment data across treatment arms. Imputations were made stepwise by visit and conditioned on data from previous visits with the same covariates used in the analysis model. b Least square means from an analysis using mixed model repeated measures with covariates of treatment group, geographic region, baseline score, and log(e) baseline blood eosinophil count visit, interaction terms for visit by baseline and visit by treatment. c This endpoint was not prespecified in the analysis plan to adjust for multiplicity. |
|||||||||||||
|
VAS Scoresa (range) |
Placebo n = 201 |
NUCALA 100 mg n = 206 |
Mean Difference vs. Placebo (95% CI) |
||||||||||
|
Baseline Mean (SD) |
Mean Changeb (SE) |
Baseline Mean (SD) |
Mean Changeb (SE) |
||||||||||
|
Loss of smell (0-10) |
9.68 (0.60) |
-1.46 (0.24) |
9.63 (0.83) |
-2.92 (0.24) |
-1.46 (-2.11, -0.81) |
||||||||
|
Nasal dischargec (0-10) |
8.78 (1.25) |
-2.49 (0.26) |
8.78 (1.07) |
-4.38 (0.25) |
-1.89 (-2.58, -1.20) |
||||||||
|
Mucus in the throatc (0-10) |
8.58 (1.63) |
-2.37 (0.26) |
8.51 (1.61) |
-4.07 (0.26) |
-1.70 (-2.41, -0.99) |
||||||||
|
Facial painc (0-10) |
7.77 (2.72) |
-2.04 (0.28) |
7.76 (2.51) |
-3.73 (0.27) |
-1.69 (-2.43, -0.95) |
||||||||
Corticosteroid Reduction
Treatment with NUCALA 100 mg significantly reduced the need for systemic steroids for nasal polyps vs. placebo up to Week 52 (odds ratio: 0.58, 95% CI: 0.36, 0.92). In patients who received NUCALA 100 mg, 52 (25%) required ≥1 course of systemic steroids compared with 74 (37%) in the placebo group throughout the 52-week treatment period.
Results in Patients with Co-morbid Asthma
In 289 (71%) patients with co-morbid asthma, pre-specified analyses showed improvements in the co-primary endpoints consistent with those seen in the overall population in the patients who received NUCALA 100 mg compared with placebo. Additionally, based on a post-hoc analysis in these patients, there was a greater response from baseline at Week 52 in asthma control as measured by the ACQ‑5 for NUCALA 100 mg compared with placebo (57% of the NUCALA patients met the responder threshold reduction of ≥0.5, compared to 35% in the placebo group, with an odds ratio of 2.42 [95% CI 1.43, 4.11]).
14.3 Eosinophilic Granulomatosis with Polyangiitis
A total of 136 adult patients with EGPA were evaluated in a randomized, placebo-controlled, multicenter, 52-week trial (NCT02020889). Patients received 300 mg of NUCALA or placebo administered subcutaneously once every 4 weeks while continuing their stable OCS therapy. Starting at Week 4, OCS was tapered during the treatment period at the discretion of the investigator. Efficacy was assessed in this trial using co-endpoints of the total accrued duration of remission over the 52-week treatment period, defined as Birmingham Vasculitis Activity Score (BVAS) = 0 (no active vasculitis) plus prednisolone or prednisone dose less than or equal to 4 mg/day, and the proportion of patients in remission at both Week 36 and Week 48 of treatment. The BVAS is a clinician-completed tool to assess clinically active vasculitis that would likely require treatment, after exclusion of other causes.
The demographics and baseline characteristics of patients in this trial are provided in Table 9.
| EGPA = Eosinophilic Granulomatosis with Polyangiitis, SD = standard deviation. a Prednisone or prednisolone equivalent. b e.g., azathioprine, methotrexate, mycophenolic acid. |
|
|
N = 136 |
|
|
Mean age, years |
48.5 |
|
Female, n (%) |
80 (59) |
|
White, n (%) |
125 (92) |
|
Duration of EGPA, years, mean (SD) |
5.5 (4.63) |
|
History of >1 confirmed relapse in past 2 years, n (%) |
100 (74) |
|
Refractory disease, n (%) |
74 (54) |
|
Recurrence of EGPA symptoms, n (%) |
68 (50) |
|
Failed induction treatment, n (%) |
6 (4) |
|
Baseline oral corticosteroida daily dose, mg, median (range) |
12 (7.5-50) |
|
Receiving immunosuppressive therapyb, n (%) |
72 (53) |
Remission
Patients receiving 300 mg of NUCALA achieved a significantly greater accrued time in remission compared with placebo. A significantly higher proportion of patients receiving 300 mg of NUCALA achieved remission at both Week 36 and Week 48 compared with placebo (Table 10). Results of the components of remission are also shown in Table 10. In addition, significantly more patients receiving 300 mg of NUCALA achieved remission within the first 24 weeks and remained in remission for the remainder of the 52-week trial treatment period compared with placebo (19% for 300 mg of NUCALA versus 1% for placebo; OR 19.7; 95% CI: 2.3, 167.9).
| EGPA = Eosinophilic Granulomatosis with Polyangiitis, OCS = oral corticosteroid, BVAS = Birmingham Vasculitis Activity Score. a An odds ratio >1 favors NUCALA. |
||||||||
|
Remission (OCS ≤4 mg/day + BVAS = 0) |
OCS ≤4 mg/day |
BVAS = 0 |
||||||
|
Placebo n = 68 |
NUCALA 300 mg n = 68 |
Placebo n = 68 |
NUCALA 300 mg n = 68 |
Placebo n = 68 |
NUCALA 300 mg n = 68 |
|||
|
Accrued duration over 52 weeks, n (%) |
||||||||
|
0 |
55 (81) |
32 (47) |
46 (68) |
27 (40) |
6 (9) |
3 (4) |
||
|
>0 to <12 weeks |
8 (12) |
8 (12) |
12 (18) |
5 (7) |
15 (22) |
13 (19) |
||
|
12 to <24 weeks |
3 (4) |
9 (13) |
6 (9) |
12 (18) |
11 (16) |
5 (7) |
||
|
24 to <36 weeks |
0 |
10 (15) |
2 (3) |
10 (15) |
17 (25) |
2 (3) |
||
|
≥36 weeks |
2 (3) |
9 (13) |
2 (3) |
14 (21) |
19 (28) |
45 (66) |
||
|
Odds ratio (NUCALA/placebo)a |
5.9 |
5.1 |
3.7 |
|||||
|
(95% CI) |
(2.7, 13.0) |
(2.5, 10.4) |
(1.8, 7.6) |
|||||
|
Proportion of patients at both Weeks 36 and 48 |
||||||||
|
Patients, n (%) |
2 (3) |
22 (32) |
7 (10) |
28 (41) |
23 (34) |
34 (50) |
||
|
Odds ratio (NUCALA/placebo)a |
16.7 |
6.6 |
1.9 |
|||||
|
(95% CI) |
(3.6, 77.6) |
(2.6, 17.1) |
(0.9, 4.2) |
|||||
Additionally, a statistically significant benefit for these endpoints was demonstrated using remission defined as BVAS = 0 plus prednisolone/prednisone ≤7.5 mg/day.
Relapse
The time to first relapse (defined as worsening related to vasculitis, asthma, or sino-nasal symptoms requiring an increase in dose of corticosteroids or immunosuppressive therapy or hospitalization) was significantly longer for patients receiving 300 mg of NUCALA compared with placebo with a hazard ratio of 0.32 (95% CI: 0.21, 0.5) (Figure 3). Additionally, patients receiving 300 mg of NUCALA had a reduction in rate of relapse compared with patients receiving placebo (rate ratio 0.50; 95% CI: 0.36, 0.70 for 300 mg of NUCALA compared with placebo). The incidence and number of relapse types (vasculitis, asthma, sino‑nasal) were numerically lower with NUCALA compared with placebo.
Figure 3. Kaplan-Meier Plot of Time to First Relapse in EGPA
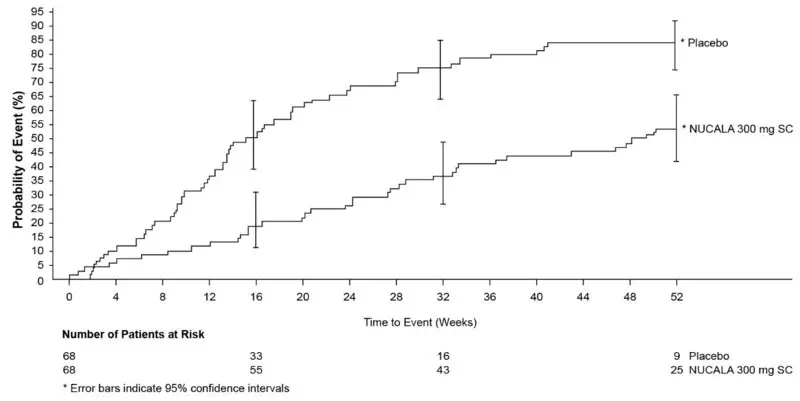
EGPA = Eosinophilic Granulomatosis with Polyangiitis, SC = subcutaneous.
Corticosteroid Reduction
Patients receiving 300 mg of NUCALA had a significantly greater reduction in average daily OCS dose compared with patients receiving placebo during Weeks 48 to 52 (Table 11).
| EGPA = Eosinophilic Granulomatosis with Polyangiitis. a Analyzed using a proportional odds model with covariates of treatment group, baseline oral corticosteroid daily dose, baseline Birmingham Vasculitis Activity Score, and region. b An odds ratio <1 favors NUCALA. |
|||||||||||
|
Number (%) of Patients |
|||||||||||
|
Placebo n = 68 |
NUCALA 300 mg n = 68 |
||||||||||
|
0 |
2 (3) |
12 (18) |
|||||||||
|
>0 to ≤4.0 mg |
3 (4) |
18 (26) |
|||||||||
|
>4.0 to ≤7.5 mg |
18 (26) |
10 (15) |
|||||||||
|
>7.5 mg |
45 (66) |
28 (41) |
|||||||||
|
Comparison: NUCALA/placeboa | |||||||||||
|
Odds ratiob |
0.20 |
||||||||||
|
95% CI |
0.09, 0.41 |
||||||||||
Asthma Control Questionnaire-6 (ACQ-6)
The ACQ-6, a 6-item questionnaire completed by the patient, was developed to measure the adequacy of asthma control and change in asthma control. The on-treatment ACQ-6 responder rate during Weeks 48 to 52 (defined as a decrease in score of 0.5 or more compared with baseline) was 22% for 300 mg of NUCALA and 16% for placebo (OR 1.56; 95% CI: 0.63, 3.88 for 300 mg of NUCALA compared with placebo).
14.4 Hypereosinophilic Syndrome
A total of 108 adult and adolescent patients aged 12 years and older with HES for at least 6 months were evaluated in a randomized, double-blind, placebo-controlled, multicenter, 32-week trial (NCT02836496). Patients with non‑hematologic secondary HES (e.g., drug hypersensitivity, parasitic helminth infection, HIV infection, non-hematologic malignancy) or FIP1L1-PDGFRα kinase-positive HES were excluded from the trial. Patients received 300 mg of NUCALA or placebo subcutaneously once every 4 weeks while continuing their stable HES therapy. Patients entering the trial had experienced at least 2 HES flares within the past 12 months and a blood eosinophil count of 1,000 cells/mcL or higher during screening. Historical HES flares for the trial entry criteria were defined as HES-related worsening of clinical symptoms or blood eosinophil counts requiring an escalation in therapy. Patients must have been on stable HES therapy for the 4 weeks prior to randomization. HES therapy could include chronic or episodic OCS, immunosuppressive, or cytotoxic therapy.
The efficacy of NUCALA in HES was established based upon the proportion of patients who experienced a HES flare during the 32-week treatment period. A HES flare was defined as worsening of clinical signs and symptoms of HES or increasing eosinophils (on at least 2 occasions), resulting in the need to increase OCS or increase/add cytotoxic or immunosuppressive HES therapy.
The demographics and baseline characteristics of patients in this trial are provided in Table 12.
| HES = Hypereosinophilic Syndrome, SD = standard deviation. | |
|
N = 108 |
|
|
Mean age, years (SD) |
46.0 (15.78) |
|
Female, n (%) |
57 (53) |
|
White, n (%) |
100 (93) |
|
Mean duration of HES, years |
5.55 |
Flares
The trial compared the proportion of patients who experienced a HES flare or withdrew from the trial in the NUCALA and placebo treatment groups (Table 13). Over the 32-week treatment period, the incidence of HES flare over the treatment period was 56% for the placebo group and 28% for the group treated with NUCALA (50% reduction).
| HES = Hypereosinophilic Syndrome, CMH = Cochran-Mantel-Haenszel. a Analysis compared the number of patients who experienced ≥1 HES flare and/or withdrew from the trial prematurely. b An odds ratio <1 favors NUCALA. |
||||
|
Number (%) of Patients |
||||
|
Placebo n = 54 |
NUCALA 300 mg n = 54 |
|||
|
Patients with ≥1 HES flare or who withdrew from trial |
30 (56) |
15 (28) |
||
|
Patients with ≥1 HES flare |
28 (52) |
14 (26) |
||
|
Patients with no HES flare who withdrew from trial |
2 (4) |
1 (2) |
||
|
Comparison: NUCALA/placeboa | ||||
|
CMH P value |
0.002 |
|||
|
Odds ratiob |
0.28 |
|||
|
95% CI |
(0.12, 0.64) |
|||
Time to First Flare
Difference was observed between NUCALA and placebo arms in the time to first HES flare (Figure 4). The risk of first HES flare over the treatment period was 66 % lower for patients treated with NUCALA compared with placebo (hazard ratio: 0.34; 95 % CI 0.18, 0.67, P = 0.002).
Figure 4. Kaplan-Meier Curve for Time to First HES Flare
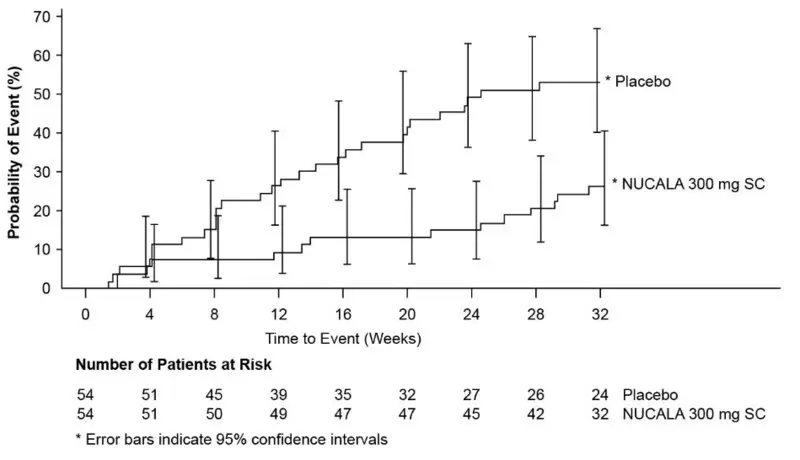
HES = Hypereosinophilic Syndrome, SC = subcutaneous.
Proportion of Patients Who Experienced Flares during Week 20 through Week 32
From Week 20 through Week 32, significantly fewer patients experienced a HES flare or withdrew from the trial when treated with 300 mg of NUCALA compared with placebo (17% vs. 35%, respectively, P = 0.020; OR: 0.33; 95 % CI: 0.13, 0.85).
Rate of Flares
Patients who received NUCALA experienced significantly fewer HES flares during the 32-week treatment period compared with the placebo group (Table 14). Treatment with NUCALA resulted in a statistically significant 66% reduction in the annualized rate of HES flares compared with placebo.
| a Adjusted P values based on pre-specified hierarchy of endpoints. b A rate ratio <1 favors NUCALA. |
|||||||
|
Number (%) of Patients |
|||||||
|
Placebo n = 54 |
NUCALA 300 mg n = 54 |
||||||
|
0 |
26 (48) |
40 (74) |
|||||
|
1 |
15 (28) |
11 (20) |
|||||
|
2 |
7 (13) |
3 (6) |
|||||
|
3 |
5 (9) |
0 |
|||||
|
4 |
1 (2) |
0 |
|||||
|
≥5 |
0 |
0 |
|||||
|
Comparison: NUCALA/placebo | |||||||
|
Wilcoxon P value (unadjusted/adjusted)a |
0.002/0.02 |
||||||
|
Rate/year |
1.46 |
0.50 |
|||||
|
Rate ratiob |
0.34 |
||||||
|
95% CI |
(0.19, 0.63) |
||||||
Brief Fatigue Inventory
Brief Fatigue Inventory (BFI) Item 3 asks patients to record their worst level of weariness/tiredness severity during the past 24 hours (scale: 0 = no fatigue to 10 = as bad as you can imagine). At baseline, median BFI Item 3 scores were similar between treatment groups (4.46 for NUCALA 300 mg and 4.69 for placebo). At Week 32, BFI Item 3 scores improved with NUCALA compared with placebo (P = 0.036). The median change from baseline score for BFI Item 3 at Week 32 was -0.66 in the group treated with NUCALA and 0.32 in the placebo group.
16. How is Nucala supplied
NUCALA for Injection
NUCALA (mepolizumab) for injection is a sterile, preservative-free, white to off-white, lyophilized powder for reconstitution and subcutaneous injection in a single-dose glass vial with a flip-off seal. The vial stopper is not made with natural rubber latex.
NUCALA for injection is supplied as:
100-mg single-dose vials in cartons of 1 (NDC 0173-0881-01).
Store vials below 77°F (25°C). Do not freeze. Store in the original carton to protect from light.
NUCALA Injection
NUCALA (mepolizumab) injection is a sterile, preservative-free, clear to opalescent, colorless to pale yellow to pale brown solution for subcutaneous use. Each single-dose prefilled autoinjector delivers 100 mg of mepolizumab in 1 mL of solution. Each single-dose prefilled syringe delivers 100 mg of mepolizumab in 1 mL of solution or 40 mg of mepolizumab in 0.4 mL of solution. The autoinjectors and syringes are not made with natural rubber latex.
NUCALA injection is supplied as:
- •
- 100 mg/mL, single-dose, prefilled autoinjector with attached 29-gauge, half-inch needle in cartons of 1 (NDC 0173-0892-01).
- •
- 100 mg/mL, single-dose, prefilled glass syringe with attached 29-gauge, half-inch needle with a needle guard in cartons of 1 (NDC 0173-0892-42).
- •
- 40 mg/0.4 mL, single-dose, prefilled glass syringe with attached 29-gauge, half-inch needle with a needle guard in cartons of 1 (NDC 0173-0904-42).
Prior to Dispensing: Refrigerate prefilled autoinjectors and prefilled syringes at 36°F to 46°F (2°C to 8°C). Keep the product in the original carton to protect from light. Do not freeze. Do not shake. Avoid exposure to heat.
Following Dispensing: Refrigerate prefilled autoinjectors and prefilled syringes at 36°F to 46°F (2°C to 8°C). Keep the product in the original carton to protect from light until the time of use. Do not freeze. Do not shake. Avoid exposure to heat.
If necessary, an unopened carton can be stored outside the refrigerator at up to 86°F (30°C) for up to 7 days. Discard if left out of the refrigerator for more than 7 days.
NUCALA injection must be administered within 8 hours after removal from the carton. Discard if not administered within 8 hours.
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Hypersensitivity Reactions
Inform patients that hypersensitivity reactions (e.g., anaphylaxis, angioedema, bronchospasm, hypotension, urticaria, rash) have occurred after administration of NUCALA. Instruct patients to contact their physicians if such reactions occur.
Not for Acute Symptoms or Deteriorating Disease
Inform patients that NUCALA does not treat acute asthma symptoms or acute exacerbations. Inform patients to seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with NUCALA.
Opportunistic Infections: Herpes Zoster
Inform patients that herpes zoster infections have occurred in patients receiving NUCALA and where medically appropriate, inform patients that vaccination should be considered.
Reduction of Corticosteroid Dosage
Inform patients to not discontinue systemic or inhaled corticosteroids except under the direct supervision of a physician. Inform patients that reduction in corticosteroid dose may be associated with systemic withdrawal symptoms and/or unmask conditions previously suppressed by systemic corticosteroid therapy.
Trademarks are owned by or licensed to the GSK group of companies.
Manufactured by
GlaxoSmithKline LLC
Philadelphia, PA 19104
U.S. License No. 1727
Distributed by
GlaxoSmithKline
Durham, NC 27701
©2023 GSK group of companies or its licensor.
NCL:10PI
|
Patient Information |
|
|
NUCALA (new KAH la) (mepolizumab) for injection, for subcutaneous use |
NUCALA (new KAH la) (mepolizumab) injection, for subcutaneous use |
|
What is NUCALA?
It is not known if NUCALA is safe and effective in children with severe asthma under 6 years of age. It is not known if NUCALA is safe and effective in children and adolescents with CRSwNP or EGPA under 18 years of age. It is not known if NUCALA is safe and effective in children with HES under 12 years of age. |
|
|
Do not use NUCALA if you are allergic to mepolizumab or any of the ingredients in NUCALA. See the end of this leaflet for a complete list of ingredients in NUCALA. |
|
|
Before receiving NUCALA, tell your healthcare provider about all of your medical conditions, including if you:
|
|
|
How will I receive NUCALA? Your healthcare provider will prescribe the dose that is right for you depending on what you are being treated for. When injection is given by a healthcare provider:
When injection is given by a patient or patient caregiver with a prefilled syringe or prefilled autoinjector:
|
|
|
What are the possible side effects of NUCALA? NUCALA can cause serious side effects, including:
ο swelling of your face, mouth, and tongue ο breathing problems ο fainting, dizziness, feeling lightheaded (low blood pressure) ο rash ο hives
The most common side effects of NUCALA include: headache, injection site reactions (pain, redness, swelling, itching, or a burning feeling at the injection site), back pain, and tiredness (fatigue). Mouth/throat pain and joint pain have been reported with CRSwNP. These are not all of the possible side effects of NUCALA. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
How should I store NUCALA?
Keep NUCALA and all medicines out of the reach of children. |
|
|
General information about the safe and effective use of NUCALA. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information Leaflet. Do not give NUCALA to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about NUCALA that is written for health professionals. |
|
|
What are the ingredients in NUCALA? Active Ingredient: mepolizumab. Inactive Ingredients (vials): polysorbate 80, sodium phosphate dibasic heptahydrate, and sucrose. Inactive Ingredients (prefilled autoinjectors and prefilled syringes): citric acid monohydrate, EDTA disodium dihydrate, polysorbate 80, sodium phosphate dibasic heptahydrate, and sucrose. For more information about NUCALA, call 1-888-825-5249 or visit our website at www.NUCALA.com. Trademarks are owned by or licensed to the GSK group of companies. Manufactured by: GlaxoSmithKline LLC, Philadelphia, PA 19104, U.S. License No. 1727 Distributed by: GlaxoSmithKline, Durham, NC 27701 ©2023 GSK group of companies or its licensor. NCL:9PIL |
|
- This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: March 2023
|
Instructions for Use |
|
NUCALA (mepolizumab) injection, for subcutaneous use 100 mg/mL Prefilled Autoinjector |
|
Important information |
|
NUCALA is a prescription medicine that is injected under the skin (subcutaneous) from a single-dose prefilled autoinjector. You and your caregiver should be trained on how to prepare and perform your injection before trying to do it yourself. The following instructions provide the information you need to correctly use the prefilled autoinjector with yellow needle guard. Before starting your injection, it is important that you read and understand these instructions and then carefully follow them so that you complete each step successfully. |
|
Storage information |
Keep NUCALA and all medicines out of the reach of children. |
|
Warnings |
|
|
Know your prefilled autoinjector |
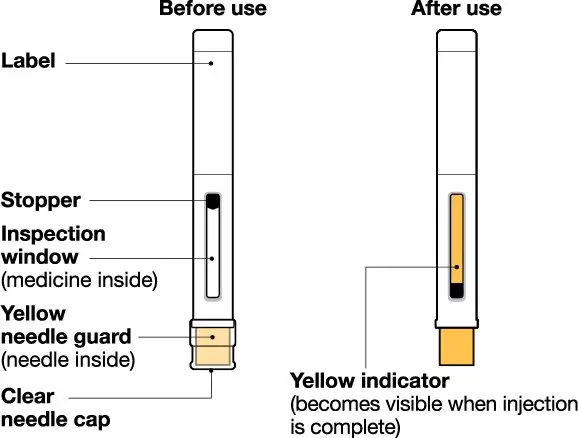 |
|
Supplies in carton |
|
1 Prefilled autoinjector |
|
Supplies not in carton |
|
|
Prepare |
|
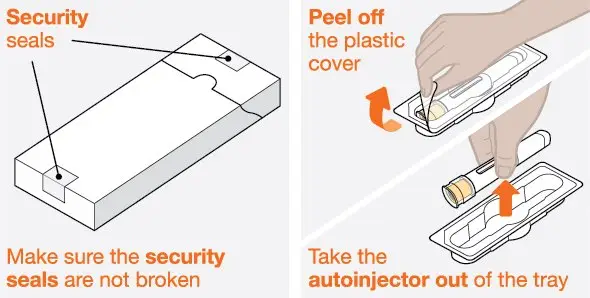 |
|
|
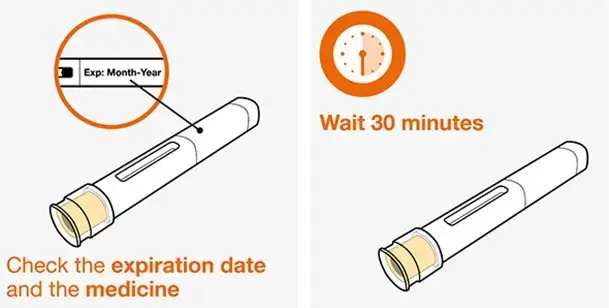 |
|
|
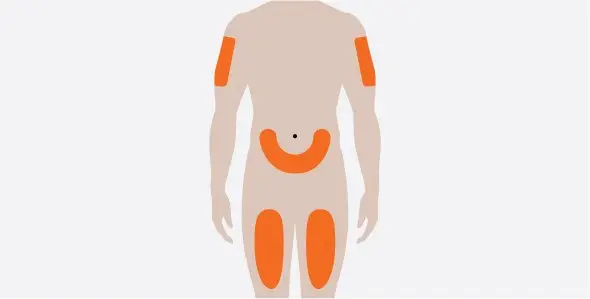 |
|
|
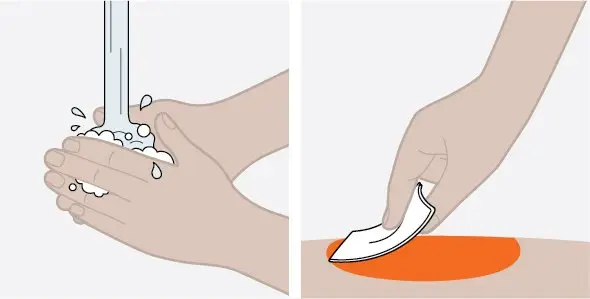 |
|
|
Inject |
|
 |
|
|
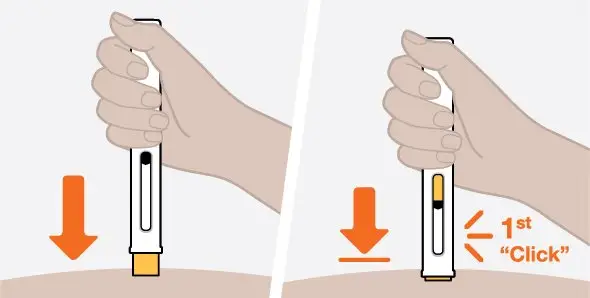 |
|
|
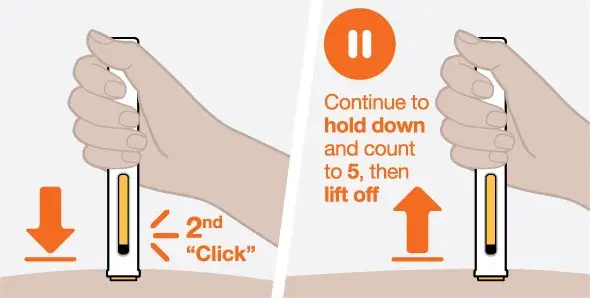 |
|
|
Dispose |
|
 |
|
Put your used autoinjector and clear needle cap in an FDA-cleared sharps disposal container right away after use. If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of it. There may be state or local laws about how you should throw away used autoinjectors. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA’s website at: www.fda.gov/safesharpsdisposal.
Keep your sharps disposal container out of the reach of children. |
|
Frequently asked questions |
For more information about NUCALA, call 1-888-825-5249 or visit our website at www.NUCALA.com. Trademarks are owned by or licensed to the GSK group of companies. Manufactured by: GlaxoSmithKline LLC, Philadelphia, PA 19104, U.S. License No. 1727 Distributed by: GlaxoSmithKline, Durham, NC 27701 ©2023 GSK group of companies or its licensor. NCL:4IFU-A This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: March 2023 |
|
Instructions for Use |
|
NUCALA (mepolizumab) injection, for subcutaneous use 100 mg/mL Prefilled Syringe |
|
Important information |
|
NUCALA is a prescription medicine that is injected under the skin (subcutaneous) from a single-dose prefilled syringe. You and your caregiver should be trained on how to prepare and perform your injection before trying to do it yourself. The following instructions provide the information you need to correctly use the prefilled syringe with automatic needle guard. Before starting your injection, it is important that you read and understand these instructions and then carefully follow them so that you complete each step successfully. |
|
Storage information |
Keep NUCALA and all medicines out of the reach of children. |
|
Warnings |
|
|
Know your prefilled syringe |
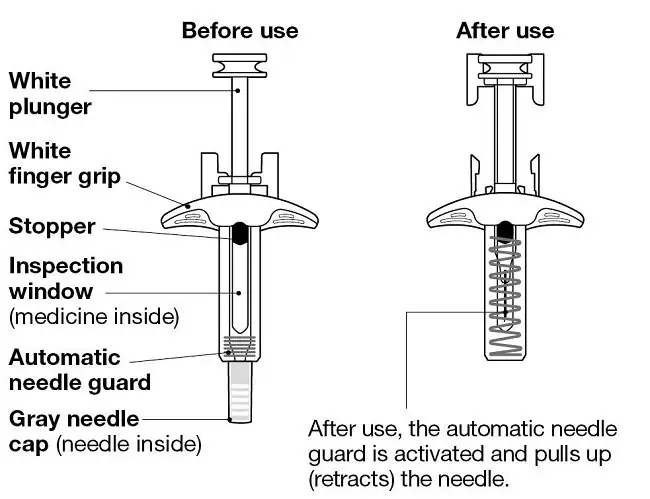 |
|
Supplies in carton |
|
1 Prefilled syringe |
|
Supplies not in carton |
|
|
Prepare |
|
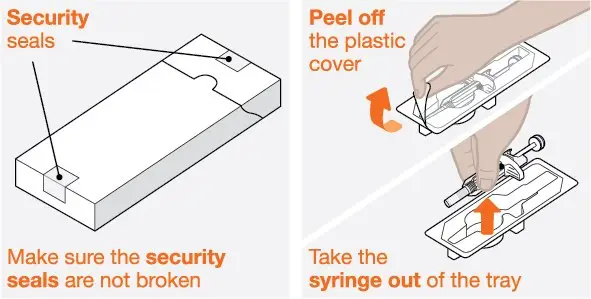 |
|
|
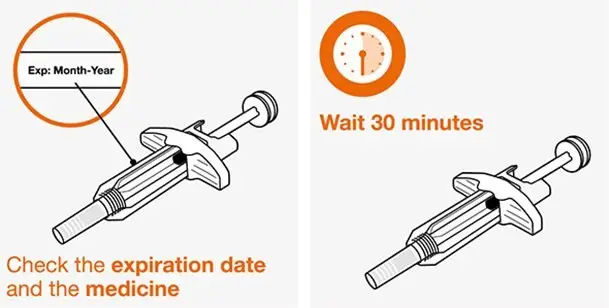 |
|
|
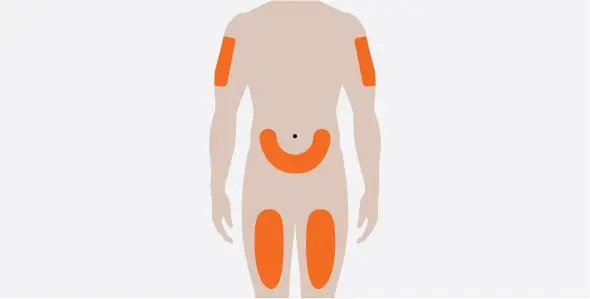 |
|
|
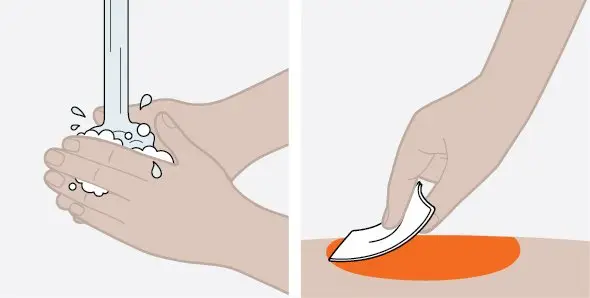 |
|
|
Inject |
|
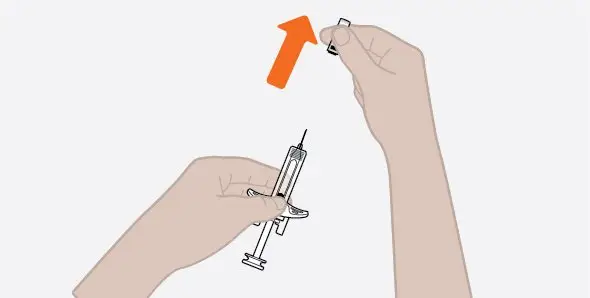 |
|
|
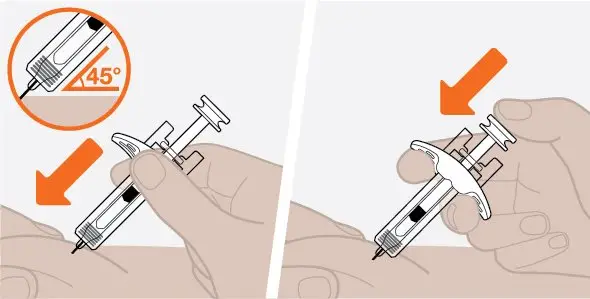 |
|
|
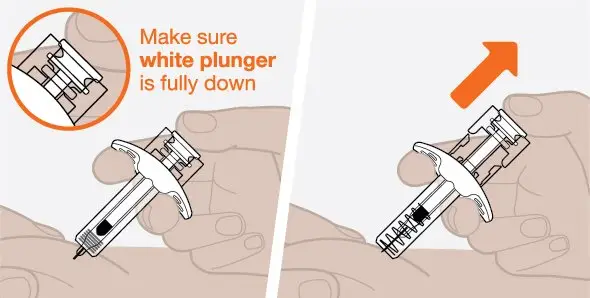 |
|
|
Dispose |
|
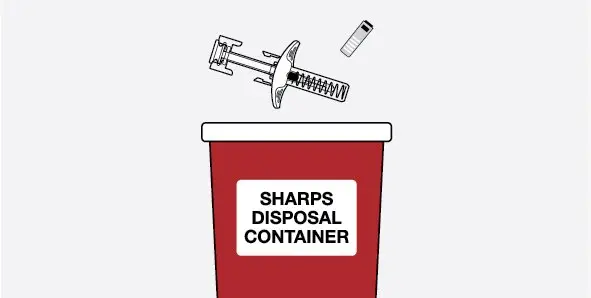 |
|
Put your used syringe and gray needle cap in an FDA-cleared sharps disposal container right away after use. If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of it. There may be state or local laws about how you should throw away used syringes. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA’s website at: www.fda.gov/safesharpsdisposal.
Keep your sharps disposal container out of the reach of children. |
|
Frequently asked questions |
For more information about NUCALA, call 1-888-825-5249 or visit our website at www.NUCALA.com. Trademarks are owned by or licensed to the GSK group of companies. Manufactured by: GlaxoSmithKline LLC, Philadelphia, PA 19104, U.S. License No. 1727 Distributed by: GlaxoSmithKline, Durham, NC 27701 ©2023 GSK group of companies or its licensor. NCL:4IFU-S This Instructions for Use has been approved by the U.S. Food and Drug Administration. Revised: March 2023 |
|
Instructions for Use |
|
NUCALA (mepolizumab) injection, for subcutaneous use 40 mg/0.4 mL Prefilled Syringe |
|
Important information |
|
NUCALA is a prescription medicine that is injected under the skin (subcutaneous) from a single-dose prefilled syringe. You should be trained on how to prepare and perform the injection before trying to do it yourself. The following instructions provide the information you need to correctly use the prefilled syringe with automatic needle guard. Before starting the injection, it is important that you read and understand these instructions and then carefully follow them so that you complete each step successfully. |
|
Storage information |
Keep NUCALA and all medicines out of the reach of children. |
|
Warnings |
|
|
Know the prefilled syringe |
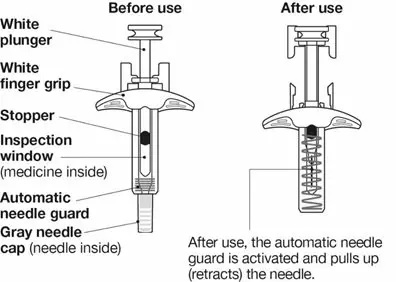 |
|
Supplies in carton |
|
1 Prefilled syringe |
|
Supplies not in carton |
|
|
Prepare |
|
1. Take out the prefilled syringe |
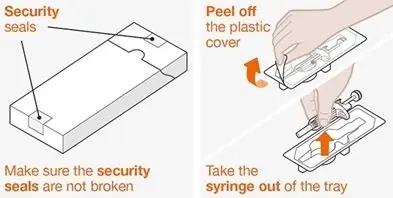 |
|
|
2. Inspect and wait 30 minutes before use |
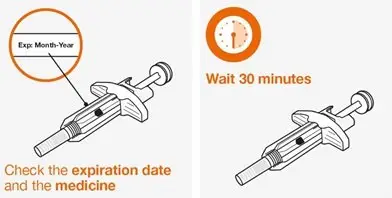 |
|
|
3. Choose the injection site |
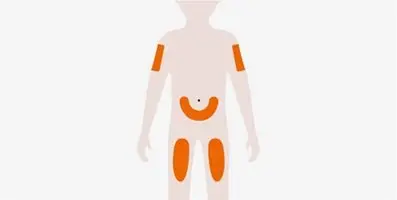 |
|
|
4. Clean the injection site |
 |
|
|
Inject |
|
5. Remove the gray needle cap |
 |
|
|
6. Start the injection |
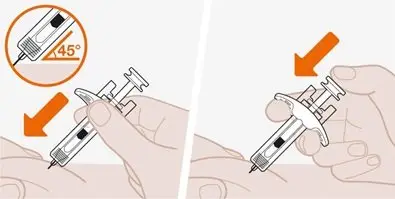 |
|
|
7. Complete the injection |
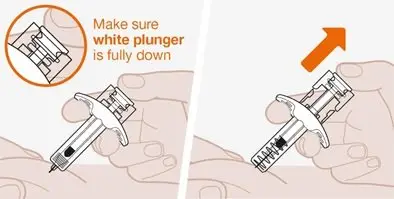 |
|
|
Dispose |
|
8. Throw away the used syringe |
 |
|
Put the used syringe and gray needle cap in an FDA-cleared sharps disposal container right away after use. If you do not have an FDA-cleared sharps disposal container, you may use a household container that is:
When the sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of it. There may be state or local laws about how you should throw away used syringes. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA’s website at: www.fda.gov/safesharpsdisposal.
Keep the sharps disposal container out of the reach of children. |
|
Frequently asked questions |
For more information about NUCALA, call 1-888-825-5249 or visit our website at www.NUCALA.com. Trademarks are owned by or licensed to the GSK group of companies. Manufactured by: GlaxoSmithKline LLC, Philadelphia, PA 19104, U.S. License No. 1727 Distributed by: GlaxoSmithKline, Durham, NC 27701 ©2023 GSK group of companies or its licensor. NCL:2IFU-S40 Revised: March 2023 |
Package/Label Display Panel
PRINCIPAL DISPLAY PANEL
NDC 0173-0881-01
Nucala
(mepolizumab)
for Injection
100 mg/vial
Rx Only
For subcutaneous injection after reconstitution.
Reconstituted solution contains 100mg/mL.
Single-dose vial. Discard unused portion.
Contents: Each vial delivers 100 mg of mepolizumab, polysorbate 80 (0.67 mg), sodium phosphate dibasic heptahydrate (7.14 mg), and sucrose (160 mg).
No preservative.
No U.S. standard of potency.
1 vial
Do not accept if plastic overseal is missing or not securely fitted.
©2019 GSK group of companies or its licensor.
- Rev. 9/19
- 62000000043659
PRINCIPAL DISPLAY PANEL
NDC 0173-0892-01
Nucala
(mepolizumab)
100 mg/mL
Rx Only
Prefilled Autoinjector
For subcutaneous use only.
Contents:
-1 Single-Dose 1-mL. Prefilled Autoinjector
-Instructions for Use
-Prescribing Information
-Patient Information
©2019 GSK group of companies or its licensor.
Do not accept if security seal is missing or broken.
- 62000000038009 Rev. 4/19
PRINCIPAL DISPLAY PANEL
NDC 0173-0904-42
Nucala
(mepolizumab)
Injection
40mg/0.4 mL
Rx Only
Prefilled Syringe
For subcutaneous use only.
Contents:
- 1 Single-Dose 0.4-mL Prefilled Syringe
- Instructions for Use
- Prescribing Information
- Patient Information
©2022 GSK group of companies or its licensor.
Rev. 3/22
62000000077331
| NUCALA
mepolizumab injection, powder, for solution |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| NUCALA
mepolizumab injection, solution |
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||
| NUCALA
mepolizumab injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - GlaxoSmithKline LLC (167380711) |
