Drug Detail:Praluent (Alirocumab [ al-i-rok-ue-mab ])
Drug Class: PCSK9 inhibitors
Highlights of Prescribing Information
PRALUENT® (alirocumab) injection, for subcutaneous use
Initial U.S. Approval: 2015
Recent Major Changes
| Indications and Usage (1) | 4/2021 |
| Dosage and Administration (2.1) | 4/2021 |
| Dosage and Administration (2.3) | 4/2021 |
| Contraindications (4) | 4/2021 |
Indications and Usage for Praluent
PRALUENT is a PCSK9 (proprotein convertase subtilisin kexin type 9) inhibitor indicated:
- To reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with established cardiovascular disease. (1)
- As adjunct to diet, alone or in combination with other low-density lipoprotein cholesterol (LDL-C)-lowering therapies, in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (HeFH), to reduce LDL-C. (1)
- As an adjunct to other LDL-C-lowering therapies in adult patients with homozygous familial hypercholesterolemia (HoFH) to reduce LDL-C. (1)
Praluent Dosage and Administration
- In adults with established cardiovascular disease or with primary hyperlipidemia, including HeFH (2.1):
- The recommended starting dose of PRALUENT is either 75 mg once every 2 weeks or 300 mg once every 4 weeks administered subcutaneously.
- For patients receiving PRALUENT 300 mg every 4 weeks, measure LDL-C just prior to the next scheduled dose, because LDL-C can vary between doses in some patients.
- If the LDL-C response is inadequate, the dosage may be adjusted 150 mg subcutaneously every 2 weeks.
- In adults with HeFH undergoing LDL apheresis or in adults with HoFH (2.1):
- The recommended dose of PRALUENT is 150 mg once every 2 weeks administered subcutaneously.
- PRALUENT can be administered without regard to the timing of LDL apheresis.
- Assess LDL-C when clinically appropriate. The LDL-lowering effect of PRALUENT may be measured as early as 4 weeks after initiation. (2.1)
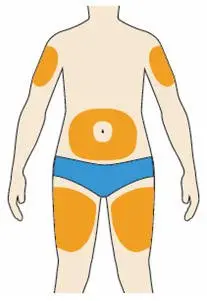
- Administer PRALUENT subcutaneously into areas of the thigh, abdomen, or upper arm that are not tender, bruised, red, or indurated. Rotate injection sites for each administration. (2.3)
- To administer the 300 mg dose, give two 150 mg PRALUENT injections consecutively at two different injection sites. (2.3)
Dosage Forms and Strengths
Injection: 75 mg/mL or 150 mg/mL in a single-dose pre-filled pen. (3)
Contraindications
History of a serious hypersensitivity reaction to alirocumab or any of the excipients in PRALUENT. (4)
Warnings and Precautions
Hypersensitivity reactions: hypersensitivity vasculitis, angioedema, and other hypersensitivity reactions requiring hospitalization, have been reported with PRALUENT treatment. If signs or symptoms of serious hypersensitivity reactions occur, discontinue treatment with PRALUENT, treat according to the standard of care, and monitor until signs and symptoms resolve. (5.1)
Adverse Reactions/Side Effects
Common (>5% of patients treated with PRALUENT and more frequently than placebo) adverse reactions in adults with:
Primary hyperlipidemia: nasopharyngitis, injection site reactions, and influenza. (6) Established cardiovascular disease: non-cardiac chest pain, nasopharyngitis, and myalgia. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Regeneron at 1-844-734-6643 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 4/2021
Full Prescribing Information
1. Indications and Usage for Praluent
PRALUENT® is indicated:
- To reduce the risk of myocardial infarction, stroke, and unstable angina requiring hospitalization in adults with established cardiovascular disease.
- As an adjunct to diet, alone or in combination with other low density lipoprotein cholesterol (LDL-C)-lowering therapies, in adults with primary hyperlipidemia, including heterozygous familial hypercholesterolemia (HeFH), to reduce LDL-C.
- As an adjunct to other LDL-C-lowering therapies in adult patients with homozygous familial hypercholesterolemia (HoFH) to reduce LDL-C.
2. Praluent Dosage and Administration
2.1 Recommended Dosage
- In adults with established cardiovascular disease or with primary hyperlipidemia, including HeFH:
- The recommended starting dose of PRALUENT is either 75 mg once every 2 weeks or 300 mg once every 4 weeks administered subcutaneously [see Dosage and Administration (2.3)].
- For patients receiving PRALUENT 300 mg every 4 weeks, measure LDL-C just prior to the next scheduled dose, because LDL-C can vary between doses in some patients [see Clinical Studies (14)].
- If the LDL-C response is inadequate, the dosage may be adjusted 150 mg subcutaneously every 2 weeks.
- In adults with HeFH undergoing LDL apheresis or in adults with HoFH:
- The recommended dose of PRALUENT is 150 mg once every 2 weeks administered subcutaneously [see Dosage and Administration (2.3)].
- PRALUENT can be administered without regard to the timing of LDL apheresis.
- Assess LDL-C when clinically appropriate. The LDL-lowering effect of PRALUENT may be measured as early as 4 weeks after initiation.
2.2 Missed Doses
If a dose is missed:
- Within 7 days from the missed dose, instruct the patient to administer PRALUENT and resume the patient's original schedule.
- More than 7 days after the missed dose:
- For every 2 week dose, instruct the patient to wait until the next dose on the original schedule.
- For every 4 week dose, instruct the patient to administer the dose and start a new schedule based on this date.
2.3 Important Administration Instructions
- Train patients and/or caregivers on how to prepare and administer PRALUENT, according to the Instructions for Use and instruct them to read and follow the Instructions for Use each time they use PRALUENT.
- Prior to use, allow PRALUENT to warm to room temperature for 30 to 40 minutes if PRALUENT has been refrigerated [see How Supplied/Storage and Handling (16)].
- Visually inspect PRALUENT prior to administration. PRALUENT is a clear, colorless to pale yellow solution. Do not use if the solution is cloudy, discolored, or contains particles.
- Administer PRALUENT subcutaneously into areas of the thigh, abdomen, or upper arm that are not tender, bruised, red, or indurated. Rotate injection sites for each administration.
- To administer the 300 mg dose, give two 150 mg PRALUENT injections consecutively at two different injection sites.
3. Dosage Forms and Strengths
PRALUENT injection is a clear, colorless to pale yellow solution available as follows:
- 75 mg/mL single-dose pre-filled pen
- 150 mg/mL single-dose pre-filled pen
4. Contraindications
PRALUENT is contraindicated in patients with a history of a serious hypersensitivity reaction to alirocumab or any of the excipients in PRALUENT. Hypersensitivity vasculitis, angioedema, and hypersensitivity reactions requiring hospitalization have occurred [see Warnings and Precautions (5.1)].
5. Warnings and Precautions
5.1 Hypersensitivity Reactions
Hypersensitivity reactions, including hypersensitivity vasculitis, angioedema, and other hypersensitivity reactions requiring hospitalization, have been reported with PRALUENT treatment. If signs or symptoms of serious hypersensitivity reactions occur, discontinue treatment with PRALUENT, treat according to the standard of care, and monitor until signs and symptoms resolve. PRALUENT is contraindicated in patients with a history of a serious hypersensitivity reaction to alirocumab or any excipient in PRALUENT [see Contraindications (4)].
6. Adverse Reactions/Side Effects
The following adverse reactions are also discussed in the other sections of the labeling:
- Hypersensitivity Reactions [see Warnings and Precautions (5.1)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data in Table 1 are derived from 9 primary hyperlipidemia placebo-controlled trials that included 2476 patients treated with PRALUENT 75 mg and/or 150 mg every 2 weeks, including 2135 exposed for 6 months and 1999 exposed for more than 1 year (median treatment duration of 65 weeks). The mean age of the population was 59 years, 40% of the population were women, 90% were White, 4% were Black or African American, and 3% were Asian.
Adverse reactions reported in at least 2% of PRALUENT-treated patients, and more frequently than in placebo-treated patients, are shown in Table 1.
| Adverse Reactions | Placebo (N=1276) % | PRALUENT*
(N=2476) % |
|---|---|---|
|
||
| Nasopharyngitis | 11.1 | 11.3 |
| Injection site reactions† | 5.1 | 7.2 |
| Influenza | 4.6 | 5.7 |
| Urinary tract infection | 4.6 | 4.8 |
| Diarrhea | 4.4 | 4.7 |
| Bronchitis | 3.8 | 4.3 |
| Myalgia | 3.4 | 4.2 |
| Muscle spasms | 2.4 | 3.1 |
| Sinusitis | 2.7 | 3.0 |
| Cough | 2.3 | 2.5 |
| Contusion | 1.3 | 2.1 |
| Musculoskeletal pain | 1.6 | 2.1 |
Adverse reactions led to discontinuation of treatment in 5.3% of patients treated with PRALUENT and 5.1% of patients treated with placebo. The most common adverse reactions leading to treatment discontinuation in patients treated with PRALUENT were allergic reactions (0.6% versus 0.2% for PRALUENT and placebo, respectively) and elevated liver enzymes (0.3% versus <0.1%).
In an analysis of ezetimibe-controlled trials in which 864 patients were exposed to PRALUENT for a median of 27 weeks and 618 patients were exposed to ezetimibe for a median of 24 weeks, the types and frequencies of common adverse reactions were similar to those listed above.
In a cardiovascular outcomes trial in which 9451 patients were exposed to PRALUENT for a median of 31 months and 9443 patients were exposed to placebo for a median of 32 months, common adverse reactions (greater than 5% of patients treated with PRALUENT and occurring more frequently than placebo) included non-cardiac chest pain (7.0% PRALUENT, 6.8% placebo), nasopharyngitis (6.0% PRALUENT, 5.6% placebo), and myalgia (5.6% PRALUENT, 5.3% placebo).
In the HoFH placebo-controlled trial in which 45 patients were exposed to PRALUENT for a median of 12 weeks and 24 patients were exposed to placebo for a median of 12 weeks, no additional adverse reactions were identified.
6.2 Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity with PRALUENT. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to PRALUENT in the studies described below with the incidence of antibodies in other studies or to other products may be misleading.
In a cardiovascular outcomes trial, 5.5% (504/9091) of patients treated with PRALUENT 75 mg and/or 150 mg every 2 weeks had anti-drug antibodies (ADA) detected after initiating treatment compared with 1.6% (149/9097) of patients treated with placebo. Persistent ADA responses, defined as at least 2 consecutive post-baseline samples with positive ADA separated by at least a 16-week period, were observed in 0.7% of patients treated with PRALUENT and 0.4% of patients treated with placebo. Neutralizing antibody (NAb) responses were observed in 0.5% of patients treated with PRALUENT and in <0.1% of patients treated with placebo. Efficacy based on reductions in LDL-C was mostly similar in patients with or without ADA. However, some patients treated with PRALUENT with persistent or neutralizing antibodies experienced attenuation in LDL-C efficacy.
A higher incidence of injection site reactions were observed in patients with treatment-emergent ADA compared to patients who were ADA negative (7.5% vs 3.6%). In a pool of ten placebo-controlled and active-controlled trials of patients treated with PRALUENT 75 mg and/or 150 mg every 2 weeks as well as in a separate clinical study of patients treated with PRALUENT 75 mg every 2 weeks or 300 mg every 4 weeks (including some patients with dose adjustment to 150 mg every 2 weeks), the incidence of detecting ADA and NAb was similar to the results from the trial described above.
The long-term consequences of continuing PRALUENT treatment in the presence of ADA are unknown.
6.3 Postmarketing Experience
The following adverse reactions have been reported during post-approval use of PRALUENT. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
- Hypersensitivity reactions: Angioedema
- Influenza-like illness
8. Use In Specific Populations
8.4 Pediatric Use
The safety and effectiveness of PRALUENT have not been established in pediatric patients.
8.5 Geriatric Use
In controlled trials, 3663 patients treated with PRALUENT were ≥65 years of age and 734 patients treated with PRALUENT were ≥75 years of age. No overall differences in safety or effectiveness were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
11. Praluent Description
Alirocumab is a human monoclonal antibody (IgG1 isotype) that targets proprotein convertase subtilisin kexin type 9 (PCSK9). Alirocumab is a PCSK9 inhibitor produced by recombinant DNA technology in Chinese Hamster Ovary cell suspension culture. Alirocumab consists of two disulfide-linked human heavy chains, each covalently linked through a disulfide bond to a human kappa light chain. A single N-linked glycosylation site is located in each heavy chain within the CH2 domain of the Fc constant region of the molecule. The variable domains of the heavy and light chains combine to form the PCSK9 binding site within the antibody. Alirocumab has an approximate molecular weight of 146 kDa.
PRALUENT is a sterile, preservative-free, clear, colorless to pale yellow solution for subcutaneous use. PRALUENT 75 mg/mL or 150 mg/mL solution for subcutaneous injection in a single-dose pre-filled pen is supplied in a siliconized 1 mL Type-1 clear glass syringe.
Each 75 mg/mL pre-filled pen contains 75 mg alirocumab, histidine (8 mM), polysorbate 20 (0.1 mg), sucrose (100 mg), and Water for Injection USP, to pH 6.0.
Each 150 mg/mL pre-filled pen contains 150 mg alirocumab, histidine (6 mM), polysorbate 20 (0.1 mg), sucrose (100 mg), and Water for Injection USP, to pH 6.0.
12. Praluent - Clinical Pharmacology
12.1 Mechanism of Action
Alirocumab is a human monoclonal antibody that binds to proprotein convertase subtilisin kexin type 9 (PCSK9). PCSK9 binds to the low-density lipoprotein (LDL) receptors (LDLR) on the surface of hepatocytes to promote LDLR degradation within the liver. By inhibiting the binding of PCSK9 to LDLR, alirocumab increases the number of LDLRs available to clear LDL, thereby lowering LDL-C levels.
12.2 Pharmacodynamics
Alirocumab reduced free PCSK9 in a concentration-dependent manner. Following a single subcutaneous administration of alirocumab 75 or 150 mg, maximal suppression of free PCSK9 occurred within 4 to 8 hours. Free PCSK9 concentrations returned to baseline when alirocumab concentrations decreased below the limit of quantitation.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with alirocumab. The mutagenic potential of alirocumab has not been evaluated; however, monoclonal antibodies are not expected to alter DNA or chromosomes.
There were no adverse effects on surrogate markers of fertility (e.g., estrous cyclicity, testicular volume, ejaculate volume, sperm motility, or total sperm count per ejaculate) in a 6-month chronic toxicology study in sexually-mature monkeys subcutaneously administered at 5, 15, and 75 mg/kg/week at systemic exposures up to 103-fold the 150 mg every two weeks subcutaneous clinical dose based on serum AUC. In addition, there were no adverse alirocumab-related anatomic pathology or histopathology findings in reproductive tissues in rat or monkey toxicology studies at systemic exposures up to 11-fold and 103-fold respectively, in the 6-month studies, compared to clinical systemic exposure following a 150 mg every two weeks dose, based on serum AUC.
13.2 Animal Toxicology and/or Pharmacology
During a 13-week toxicology study of 75 mg/kg once weekly alirocumab in combination with 40 mg/kg once daily atorvastatin in adult monkeys, there were no effects of PRALUENT on the humoral immune response to keyhole limpet hemocyanin (KLH) after one to two months at exposures 100-fold greater than the exposure at the maximum recommended human dose of 150 mg every two weeks, based on AUC.
14. Clinical Studies
Adult Patients with Established Cardiovascular Disease
Study 1 (ODYSSEY OUTCOMES, NTC01663402) was a multicenter, double-blind, placebo-controlled trial in 18,924 adult patients (9462 PRALUENT; 9462 placebo) followed for up to 5 years. Patients had an acute coronary syndrome (ACS) event 4 to 52 weeks prior to randomization and were treated with a lipid-modifying therapy (LMT) regimen that was statin-intensive (defined as atorvastatin 40 or 80 mg, or rosuvastatin 20 or 40 mg) or at maximally tolerated dose of a statin, with or without other LMT. Patients were randomized to receive either PRALUENT 75 mg or placebo once every two weeks.
At month 2, if additional LDL-C lowering was required based on pre-specified LDL-C criteria (LDL-C ≥50 mg/dL), PRALUENT was adjusted to 150 mg every 2 weeks. For patients who had their dose adjusted to 150 mg every 2 weeks and who had two consecutive LDL-C values below 25 mg/dL, down-titration from 150 mg every 2 weeks to 75 mg every 2 weeks was performed. Patients on 75 mg every 2 weeks who had two consecutive LDL-C values below 15 mg/dL were switched to placebo in a blinded fashion. Approximately 2615 (27.7%) of 9451 patients treated with PRALUENT required dose adjustment to 150 mg every 2 weeks. Of these 2615 patients, 805 (30.8%) were down-titrated to 75 mg every 2 weeks. Overall, 730 (7.7%) of 9451 patients switched to placebo.
A total of 99.5% of patients were followed for survival until the end of the trial. The median follow-up duration was 33 months.
The mean age at baseline was 59 years (range 39-92), with 25% women, and 27% at least 65 years old. The trial population was 79% White, 3% Black, and 13% Asian; 17% identified as Hispanic/Latino ethnicity. The index ACS event was a myocardial infarction in 83% of patients and unstable angina in 17% of patients. Prior to the index ACS event, 19% had prior myocardial infarction and 23% had coronary revascularization procedures (CABG/PCI). Selected additional baseline risk factors included hypertension (65%), diabetes mellitus (25%), New York Association class I or II congestive heart failure (15%), and eGFR <60 mL/min/1.73 m2 (13%). Most patients (89%) were receiving statin-intensive therapy with or without other LMT at randomization. The mean LDL-C value at baseline was 92.4 mg/dL.
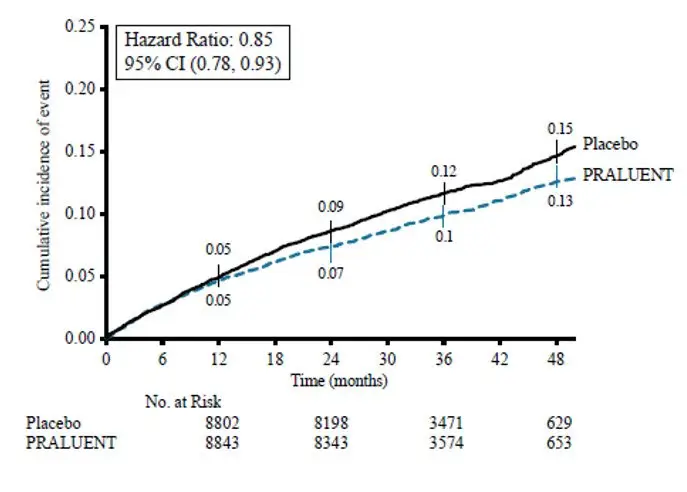
PRALUENT significantly reduced the risk for the primary composite endpoint (time to first occurrence of coronary heart disease death, non-fatal myocardial infarction, fatal and non-fatal ischemic stroke, or unstable angina requiring hospitalization: p=0.0003). The results are presented in Table 2.
| Endpoint | PRALUENT N=9462 | Placebo N=9462 | Hazard Ratio (95% CI)* |
||
|---|---|---|---|---|---|
| n (%) | Incidence Rate per 100 Patient Years (95% CI) | n (%) | Incidence Rate per 100 Patient Years (95% CI) |
||
|
|||||
| Primary composite endpoint† | 903 (9.5%) | 3.5 (3.3 to 3.8) | 1052 (11.1%) | 4.2 (3.9 to 4.4) | 0.85 (0.78, 0.93) |
| Components of the Primary Composite Endpoint‡ | |||||
| CHD death | 205 (2.2%) | 0.8 (0.7 to 0.9) | 222 (2.3%) | 0.8 (0.7 to 0.9) | 0.92 (0.76, 1.11) |
| Non-fatal MI§ | 626 (6.6%) | 2.4 (2.2 to 2.6) | 722 (7.6%) | 2.8 (2.6 to 3.0) | 0.86 (0.77, 0.96) |
| Fatal or non-fatal ischemic stroke§ | 111 (1.2%) | 0.4 (0.3 to 0.5) | 152 (1.6%) | 0.6 (0.5 to 0.7) | 0.73 (0.57, 0.93) |
| Unstable angina requiring hospitalization§ | 37 (0.4%) | 0.1 (0.1 to 0.2) | 60 (0.6%) | 0.2 (0.2 to 0.3) | 0.61 (0.41, 0.92) |
| Mortality Endpoint (not statistically significant per pre-specified method to control for type I error) | |||||
| All-cause mortality | 334 (3.5%) | 1.2 (1.1 to 1.4) | 392 (4.1%) | 1.5 (1.3 to 1.6) | 0.85 (0.73, 0.98) |
The Kaplan-Meier estimates of the cumulative incidence of the primary endpoint over time is presented in Figure 1.
Figure 1: Primary Composite Endpoint Cumulative Incidence over 4 Years in ODYSSEY OUTCOMES
Primary Hyperlipidemia
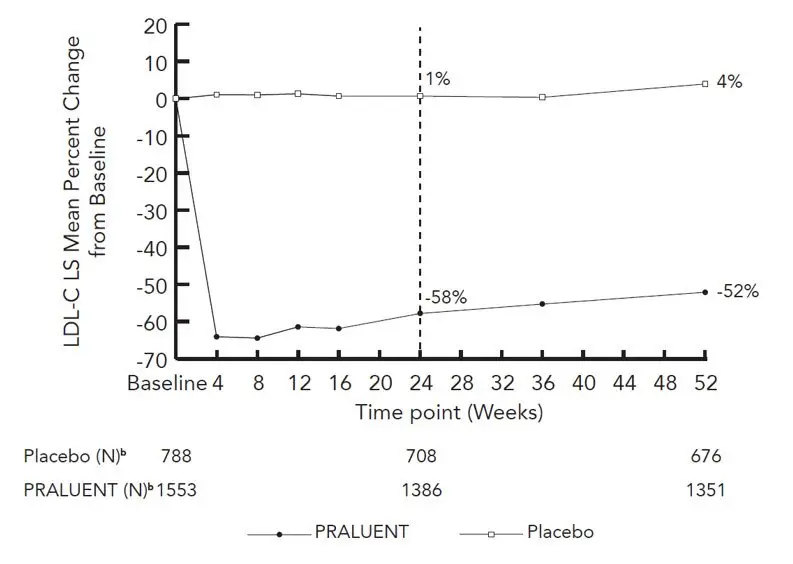
Study 2 (ODYSSEY LONG TERM, NCT01507831) was a multicenter, double-blind, placebo-controlled trial that randomly assigned 1553 patients to PRALUENT 150 mg every 2 weeks and 788 patients to placebo. All patients were taking maximally tolerated doses of statins with or without other lipid-modifying therapy, and required additional LDL-C reduction. The mean age was 61 years (range 18-89), 38% were women, 93% were White, 3% were Black, and 5% were Hispanic/Latino. The average LDL-C at baseline was 122 mg/dL.
The proportion of patients who prematurely discontinued study drug prior to the 24-week primary endpoint was 8% among those treated with PRALUENT and 8% among those treated with placebo.
At week 24, the treatment difference between PRALUENT and placebo in mean LDL-C percent change was -58% (95% CI: -61%, -56%; p-value: ˂0.0001).
For additional results see Table 3 and Figure 2.
| Treatment Group | LDL-C | Total-C | Non-HDL-C | Apo B |
|---|---|---|---|---|
|
||||
| Week 24 (Mean Percent Change from Baseline) | ||||
| Placebo (n=788) | 1 | 0 | 1 | 1 |
| PRALUENT 150 mg (n=1553) | -58 | -36 | -49 | -50 |
| Difference from placebo (LS Mean) (95% CI) | -58 (-61, -56) | -36 (-37, -34) | -50 (-52, -47) | -51 (-53, -48) |
| a The means were estimated based on all randomized patients, with multiple imputation of missing data taking into account treatment adherence |
| b Number of patients with observed data |
| Figure 2: Mean Percent Change from Baseline in LDL-C Over 52 Weeks in Patients on Maximally Tolerated Statin Treated with PRALUENT 150 mg Every 2 Weeks and Placebo Every 2 Weeks (ODYSSEY LONG TERM)a |
|
|
Study 3 (ODYSSEY COMBO I, NCT01644175) was a multicenter, double-blind, placebo-controlled trial that randomly assigned 209 patients to PRALUENT and 107 patients to placebo. Patients were taking maximally tolerated doses of statins with or without other lipid-modifying therapy, and required additional LDL-C reduction.
The mean age was 63 years (range 39-87), 34% were women, 82% were White, 16% were Black, and 11% were Hispanic/Latino. Mean baseline LDL-C was 102 mg/dL.
The proportion of patients who prematurely discontinued study drug prior to the 24-week primary endpoint was 11% among those treated with PRALUENT and 12% among those treated with placebo.
At week 12, the mean percent change from baseline in LDL-C was -45% with PRALUENT compared to 1% with placebo, and the treatment difference between PRALUENT 75 mg every 2 weeks and placebo in mean LDL-C percent change was -46% (95% CI: -53%, -39%).
At week 12, if additional LDL-C lowering was required based on pre-specified LDL-C criteria, PRALUENT was up-titrated to 150 mg every 2 weeks for the remainder of the trial. The dose was up-titrated to 150 mg every 2 weeks in 32 (17%) of 191 patients treated with PRALUENT for at least 12 weeks. At week 24, the mean percent change from baseline in LDL-C was -44% with PRALUENT and -2% with placebo, and the treatment difference between PRALUENT and placebo in mean LDL-C percent change was -43% (95% CI: -50%, -35%; p-value: ˂0.0001).
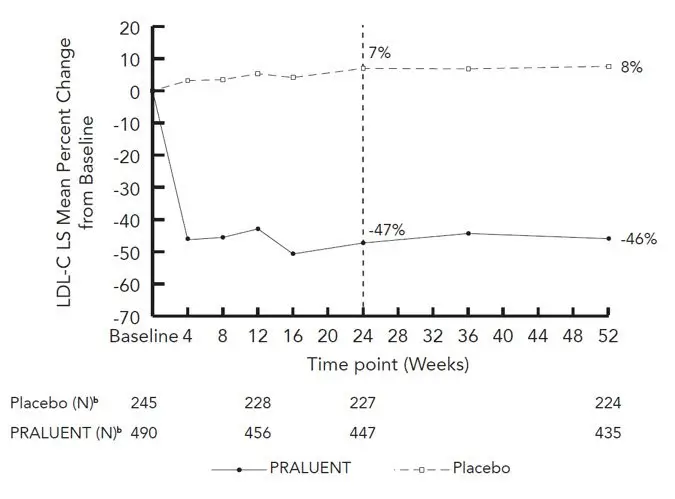
Studies 4 (ODYSSEY FH I, NCT01623115) and 5 (ODYSSEY FH II, NCT01709500) were multicenter, double-blind, placebo-controlled trials that, combined, randomly assigned 490 patients to PRALUENT and 245 patients to placebo. The trials were similar with regard to both design and eligibility criteria. All patients had HeFH, were taking a maximally tolerated dose of statin with or without other lipid-modifying therapy, and required additional LDL-C reduction. The diagnosis of HeFH was made either by genotyping or clinical criteria ("definite FH" using either the Simon Broome or WHO/Dutch Lipid Network criteria). The mean age was 52 years (range 20-87), 45% were women, 94% were White, 1% were Black, and 3% were Hispanic/Latino. The average LDL-C at baseline was 141 mg/dL.
Considering both trials together, the proportion of patients who prematurely discontinued study drug prior to the 24-week primary endpoint was 6% among those treated with PRALUENT and 4% among those treated with placebo.
At week 12, the treatment difference between PRALUENT 75 mg every 2 weeks and placebo in mean LDL-C percent change was -48% (95% CI: -52%, -44%).
At week 12, if additional LDL-C lowering was required based on pre-specified LDL-C criteria, PRALUENT was up-titrated to 150 mg every 2 weeks for the remainder of the trials. The dose was up-titrated to 150 mg every 2 weeks in 196 (42%) of 469 patients treated with PRALUENT for at least 12 weeks. At week 24, the mean treatment difference between PRALUENT and placebo in mean LDL-C percent change from baseline was -54% (95% CI: -59%, -50%; p-value: ˂0.0001). The LDL-C-lowering effect was sustained to week 52.
For additional results see Table 4 and Figure 3.
| Treatment Group | LDL-C | Total-C | Non-HDL-C | Apo B |
|---|---|---|---|---|
|
||||
| Week 12 (Mean Percent Change from Baseline) | ||||
| Placebo (n=245) | 5 | 4 | 5 | 2 |
| PRALUENT 75 mg (n=490) | -43 | -27 | -38 | -34 |
| Difference from placebo (LS Mean) (95% CI) | -48 (-52, -44) | -31 (-34, -28) | -42 (-46, -39) | -36 (-39, -33) |
| Week 24 (Mean Percent Change from Baseline) | ||||
| Placebo (n=245) | 7 | 5 | 7 | 2 |
| PRALUENT 75 mg/150 mg‡ (n=490) | -47 | -30 | -42 | -40 |
| Difference from placebo (LS Mean) (95% CI) | -54 (-59, -50) | -36 (-39, -33) | -49 (-53, -45) | -42 (-45, -39) |
| a The means were estimated based on all randomized patients, with multiple imputation of missing data taking into account treatment adherence |
| b Number of patients with observed data |
| Figure 3: Mean Percent Change from Baseline in LDL-C Over 52 Weeks in Patients with HeFH on Maximally Tolerated Statin Treated with PRALUENT 75/150 mg Every 2 Weeks and Placebo every 2 weeks (ODYSSEY FH I and FH II Pooled)a |
|
|
Study 6 (ODYSSEY HIGH FH, NCT01617655) was a multicenter, double-blind, placebo-controlled trial that randomly assigned 72 patients to PRALUENT 150 mg every 2 weeks and 35 patients to placebo. Patients had HeFH with a baseline LDL-C ≥160 mg/dL while taking a maximally tolerated dose of statin with or without other lipid-modifying therapy. The mean age was 51 years (range 18-80), 47% were women, 88% were White, 2% were Black, and 6% were Hispanic/Latino. The average LDL-C at baseline was 198 mg/dL.
The proportion of patients who discontinued study drug prior to the 24-week primary endpoint was 10% among those treated with PRALUENT and 0% among those treated with placebo.
At week 24, the mean percent change from baseline in LDL-C was -43% with PRALUENT and -7% with placebo, and the treatment difference between PRALUENT and placebo in mean LDL-C percent change was -36% (95% CI: -49%, -24%; p-value: ˂0.0001).
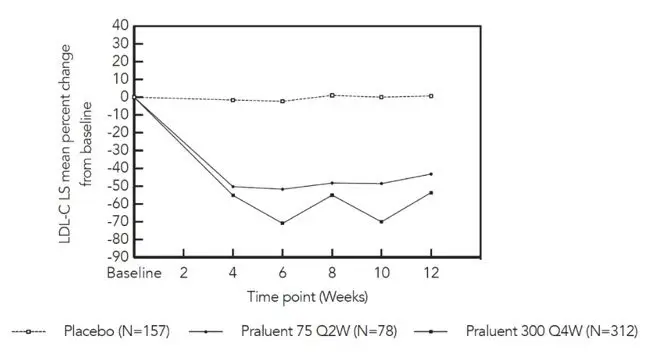
Study 7 (ODYSSEY CHOICE I, NCT01926782) was a multicenter, double-blind, placebo-controlled trial that randomly assigned 458 patients with primary hyperlipidemia to PRALUENT 300 mg every 4 weeks, 115 patients to PRALUENT 75 mg every 2 weeks, and 230 patients to placebo. Patients were stratified based on whether or not they were treated concomitantly with statin.
The mean age was 61 years (range 21-88), 42% were women, 87% were White, 11% were Black, and 3% were Hispanic/Latino.
The proportion of patients who discontinued study drug prior to the 24-week primary endpoint was 12% among those treated with PRALUENT 300 mg every 4 weeks, 14% among those treated with PRALUENT 75 mg every 2 weeks, and 15% among those treated with placebo.
In the cohort of patients on background statin, the mean LDL-C at baseline was 113 mg/dL. At week 12, the treatment difference between PRALUENT 300 mg every 4 weeks and placebo in mean percent change in LDL-C from baseline was -54% (97.5% CI: -61%, -48%), and the treatment difference between PRALUENT 75 mg every 2 weeks and placebo in mean percent change in LDL-C was -44% (97.5% CI: -53%, -35%) (Figure 4).
| a The means were estimated based on all randomized patients, with multiple imputation of missing data taking into account treatment adherence |
| Figure 4: Mean Percent Change from Baseline in LDL-C up to Week 12 in Patients on Concomitant Statin Treated with PRALUENT 75 mg Every 2 Weeks, PRALUENT 300 mg Every 4 Weeks or Placeboa |
|
|
At week 12, if additional LDL-C lowering was required based on pre-specified LDL-C criteria, PRALUENT was adjusted to 150 mg every 2 weeks for the remainder of the trial. The dose was adjusted to 150 mg every 2 weeks in approximately 20% of patients treated with PRALUENT 75 mg every 2 weeks or 300 mg every 4 weeks for at least 12 weeks.
At week 24, the treatment difference between initial assignment to PRALUENT 300 mg every 4 weeks and placebo in mean percent change in LDL-C from baseline was -56% (97.5% CI: -62%, -49%; p-value: <0.0001), and the treatment difference between initial assignment to PRALUENT 75 mg every 2 weeks and placebo in mean percent change in LDL-C from baseline was -48% (97.5% CI: -57%, -39%).
In the cohort of patients not treated with a concomitant statin, the mean LDL-C at baseline was 142 mg/dL. The treatment difference between PRALUENT and placebo were similar to the cohort of patients treated with a concomitant statin.
Study 8 (ODYSSEY ESCAPE, NCT02326220) was a multicenter, double-blind, placebo-controlled trial that randomly assigned patients with HeFH who were undergoing LDL apheresis to PRALUENT 150 mg every 2 weeks (N=41) or placebo (N=21). Patients were treated in combination with their usual LDL apheresis schedule for 6 weeks. The mean age was 59 years (range 27-79), 42% were women, 97% were White, 3% were Black, and 0% were Hispanic/Latino. The mean LDL-C at baseline, measured before the apheresis procedure, was 181 mg/dL. The proportion of patients who discontinued study drug prior to the 6-week endpoint was 2% among those treated with PRALUENT 150 mg every 2 weeks and 5% among those treated with placebo. At week 6, the mean percent change from baseline in pre-apheresis LDL-C was -53% in patients in the PRALUENT group compared to 1% in patients who received placebo.
Study 9 (ODYSSEY COMBO II, NCT01644188) was a multicenter, double-blind, ezetimibe-controlled trial that randomly assigned 479 patients to PRALUENT 75 mg every 2 weeks/150 mg every 2 weeks and 241 patients to ezetimibe 10 mg/day. Patients were taking a maximally tolerated dose of a statin and required additional LDL-C reduction.
The mean age was 62 years (range 29-88), 26% were women, 85% were White, 4% were Black, and 3% were Hispanic/Latino. Mean baseline LDL-C was 107 mg/dL.
The proportion of patients who prematurely discontinued study drug prior to the 24-week primary endpoint was 9% among those treated with PRALUENT and 10% among those treated with ezetimibe.
At week 12, the mean percent change from baseline in LDL-C was -50% with PRALUENT compared to -22% with ezetimibe, and the treatment difference between PRALUENT and ezetimibe in mean LDL-C percent change was -28% (95% CI: -32%, -23%).
At week 12, if additional LDL-C lowering was required based on pre-specified LDL-C criteria, PRALUENT was up-titrated to 150 mg every 2 weeks for the remainder of the trial. The dose was up-titrated to 150 mg every 2 weeks in 82 (18%) of 446 patients treated with PRALUENT for at least 12 weeks. At week 24, the mean percent change from baseline in LDL-C was -48% with PRALUENT and -20% with ezetimibe, and the treatment difference between PRALUENT and ezetimibe in mean LDL-C percent change was -28% (95% CI: -33%, -23%; p-value: ˂0.0001).
Study 10 (ODYSSEY MONO, NCT01644474) was a multicenter, double-blind, ezetimibe-controlled trial in patients with a moderate CV risk, not taking statins or other lipid-modifying therapies, and a baseline LDL-C between 100 mg/dL to 190 mg/dL that randomly assigned 52 patients to PRALUENT 75 mg every 2 weeks and 51 patients to ezetimibe 10 mg/day.
The mean age was 60 years (range 45-72), 47% were women, 90% were White and 10% were Black. Mean baseline LDL-C was 140 mg/dL.
The proportion of patients who prematurely discontinued study drug prior to the 24-week endpoint was 15% among those treated with PRALUENT and 14% among those treated with ezetimibe.
At week 12, the mean percent change from baseline in LDL-C was -48% with PRALUENT compared to -19% with ezetimibe, and the treatment difference between PRALUENT 75 mg every 2 weeks and ezetimibe in mean LDL-C percent change was -29% (95% CI: -37%, -22%). At week 12, if additional LDL-C lowering was required based on pre-specified LDL-C criteria, PRALUENT was up-titrated to 150 mg every 2 weeks for the remainder of the trial. The dose was up-titrated to 150 mg every 2 weeks in 14 (30%) of 46 patients treated with PRALUENT for at least 12 weeks. At week 24, the mean percent change from baseline in LDL-C was -45% with PRALUENT and -14% with ezetimibe, and the treatment difference between PRALUENT and ezetimibe in mean LDL-C percent change was -31% (95% CI: -40%, -22%; p-value: ˂0.0001).
HoFH
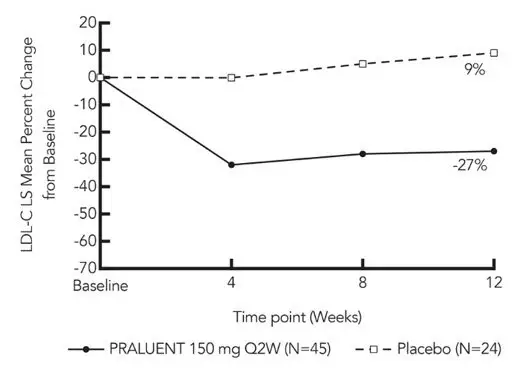
Study 11 (ODYSSEY HoFH, NCT03156621) was a multicenter, double-blind, placebo-controlled trial that randomly assigned 45 adult patients to PRALUENT 150 mg every 2 weeks and 24 adult patients to placebo. Patients were taking maximally tolerated doses of statins with or without other lipid-lowering therapy and required additional LDL-C reduction. Randomization was stratified by LDL apheresis treatment status. The diagnosis of HoFH was made by either clinical diagnosis, which included a history of an untreated total cholesterol concentration >500 mg/dL together with either xanthoma before 10 years of age or with a history of total cholesterol >250 mg in both parents, or by genetic testing. The mean age was 43 years (range 19-81), 51% were women, 78% were White, 3% were Black, 17% were Asian, and 3% were identified as Hispanic/Latino ethnicity. Mean baseline LDL-C was 283 mg/dL with 97% on statins, 72% on ezetimibe, and 14% on lomitapide. No patient discontinued from the study prior to the 12-week primary endpoint.
At week 12, the treatment difference between PRALUENT and placebo in mean LDL-C percent change from baseline was -36% (95% CI: -51% to -20%; p <0.0001) (see Figure 5). For the effect of PRALUENT on lipid parameters as compared to placebo, see Table 5.
Patients with two LDL-receptor negative alleles (little to no residual function) had a minimal to absent response to PRALUENT.
| Treatment Group | LDL-C | Apo B | Non-HDL-C | Total Cholesterol |
|---|---|---|---|---|
| Placebo (n=24) | 9 | 7 | 8 | 7 |
| PRALUENT 150 mg every 2 weeks (n=45) | -27 | -23 | -25 | -20 |
| Difference from placebo (LS Mean) (95% CI) | -36 (-51, -20) | -30 (-42, -17) | -33 (-48, -18) | -27 (-39, -14) |
16. How is Praluent supplied
PRALUENT injection is a clear, colorless to pale yellow solution, supplied as follows:
| Pack Size | 75 mg/mL Pre-filled Pen | 150 mg/mL Pre-filled Pen |
|---|---|---|
| Pack of 1 pen | NDC 0024-5901-01 | NDC 0024-5902-01 |
| Pack of 2 pens | NDC 0024-5901-02 NDC 72733-5901-2 | NDC 0024-5902-02 NDC 72733-5902-2 |
The needle shield is not made with natural rubber latex.
17. Patient Counseling Information
Advise the patient to read the FDA-Approved Patient Labeling (Patient Information and Instructions for Use).
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: April 2021 | |||
| Patient Information PRALUENT® (PRAHL-u-ent) (alirocumab) injection, for subcutaneous use |
||||
| What is PRALUENT?
PRALUENT is an injectable prescription medicine used:
|
||||
| Who should not use PRALUENT?
Do not use PRALUENT if you are allergic to alirocumab or to any of the ingredients in PRALUENT. See the end of this leaflet for a complete list of ingredients in PRALUENT. |
||||
| What should I tell my healthcare provider before using PRALUENT?
Before you start using PRALUENT, tell your healthcare provider about all of your medical conditions, including allergies, and if you:
Tell your healthcare provider or pharmacist about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. |
||||
How should I use PRALUENT?
|
||||
| What are the possible side effects of PRALUENT?
PRALUENT can cause serious side effects, including:
|
||||
|
|
|
||
| The most common side effects of PRALUENT include: | ||||
|
|
|||
| Tell your healthcare provider if you have any side effect that bothers you or that does not go away. These are not all of the possible side effects of PRALUENT. Ask your healthcare provider or pharmacist for more information. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
||||
| General information about the safe and effective use of PRALUENT.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use PRALUENT for a condition for which it was not prescribed. Do not give PRALUENT to other people, even if they have the same symptoms that you have. It may harm them. This Patient Information summarizes the most important information about PRALUENT. If you would like more information, talk with your healthcare provider. You can ask your pharmacist or healthcare provider for information about PRALUENT that is written for health professionals. For more information about PRALUENT, go to www.PRALUENT.com or call 1-844-PRALUENT (1-844-772-5836). |
||||
| What are the ingredients in PRALUENT? | ||||
|
|
|||
| Manufactured by: sanofi-aventis U.S. LLC, Bridgewater, NJ 08807; A SANOFI COMPANY, U.S. License # 1752; Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807) and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591) / PRALUENT is a registered trademark of Sanofi / ©2021 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC | ||||
Instructions For Use
PRALUENT® (PRAHL-u-ent)
(alirocumab)
Injection, for Subcutaneous Injection
Single-Dose Pre-Filled Pen (75 mg/mL)
| Important Information | |
|---|---|
|
|
Storage of PRALUENT
|
|
Keep this leaflet. If you have questions, ask your healthcare provider or call 1-844-PRALUENT (1-844-772-5836).
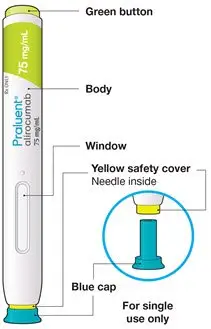
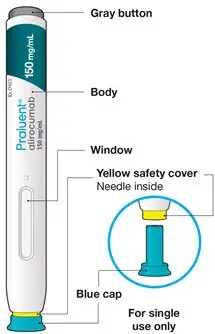
The parts of the PRALUENT pen are shown in this picture.
Step A: Getting ready for your injection
Before you start you will need:
- the PRALUENT pen
- 1 alcohol wipe
- 1 cotton ball or gauze
- a puncture-resistant container (see Step B8)
A1: Look at the label on the pen.
- Check that you have the correct product and the correct dose.
- Check the expiration date: do not use if this date has passed.

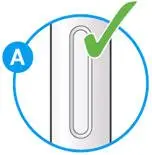
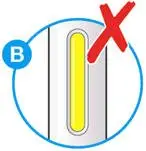
A2: Look at the window.
- Check the liquid is clear, colorless to pale yellow and free from particles (see Figure A).
- You may see an air bubble. This is normal.
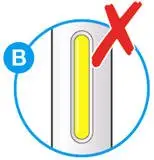
- Do not use if the window appears solid yellow (see Figure B).
- Do not use this medicine if the solution is discolored or cloudy, or if it contains visible flakes or particles.
A3: Let the pen warm up at room temperature for 30 to 40 minutes.
- This is important for administering the entire dose and helps minimize discomfort.
- Take PRALUENT out of the refrigerator to warm up before using.
- Do not heat the pen, let it warm up on its own.
- Do not put the pen back in the refrigerator.

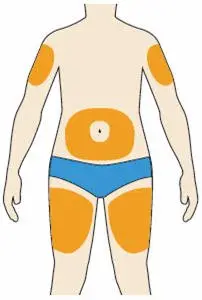
A4: Prepare the injection site.
- Wash your hands with soap and water and dry with a towel.
- Clean skin in the injection area with an alcohol wipe.
- You can inject into your (see below picture):
- thighs
- stomach (except for the 2 inch area around your navel)
- upper arms
- You can stand or sit to give yourself an injection.
Important:
- Change (rotate) your injection site each time you give yourself an injection. If you need to use the same injection site, make sure it is not the same spot on the site you used last time.
- Do not inject into areas where the skin is injured, tender, hard, red, or hot. Do not inject PRALUENT into areas with visible veins, scars or stretch marks.
Step B: How to give your injection
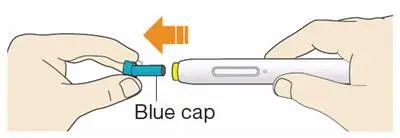
B1: After completing all steps in "Step A: Getting ready for your injection", pull off the blue cap.
- Do not pull off the cap until you are ready to inject.
- Do not put the blue cap back on.
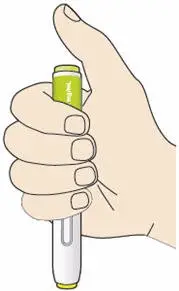
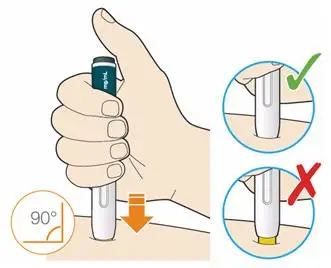
B2: Hold the PRALUENT pen like this.
- Do not touch the yellow safety cover.
- Make sure you can see the window.
B3: Press the yellow safety cover on your skin at roughly a 90° angle.
- Press and firmly hold the pen against your body until the yellow safety cover is no longer visible. The pen will not work if the yellow safety cover is not depressed fully.
- If needed, pinch the skin to make sure the injection site is firm.
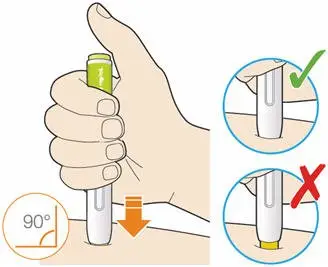
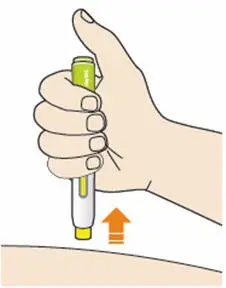
B4: Push and immediately release the green button with your thumb.
- You will hear a click. Your injection has now started.
- The window will start to turn yellow.

B5: Keep holding the pen against your skin after releasing the button.
- The injection may take up to 20 seconds.
- The time required for injection to give the entire dose may be longer than for other injectable medicines.

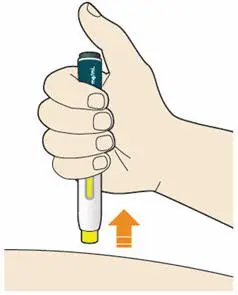
B6: Check the window has turned yellow, before removing the pen.
- Do not remove the pen until the entire window has turned yellow.
- Your injection is complete when the window has turned completely yellow, you may hear a second click.
- If the window does not turn completely yellow, call 1-844-772-5836 for help. Do not give yourself a second dose without speaking to your healthcare provider.

B7: Pull pen away from your skin.
- Do not rub the skin after the injection.
- If you see any blood, press a cotton ball or gauze on the site until the bleeding stops.
- Do not put the blue cap back on.
- Throw away pen and cap in a puncture-resistant container immediately after they have been used.

Disposing of used pens:
- Put your used pens in a FDA-cleared sharps disposal container right away after use. Do not throw away (dispose of) pens and caps in your household trash.
- If you do not have a FDA-cleared sharps disposal container, you may use a household container that is:
- made of a heavy-duty plastic,
- can be closed with a tight-fitting, puncture-resistant lid, without sharps being able to come out,
- upright and stable during use,
- leak-resistant, and
- properly labeled to warn of hazardous waste inside the container.
- When your sharps disposal container is almost full, you will need to follow your community guidelines for the right way to dispose of your sharps disposal container. There may be state or local laws about how you should throw away used needles and syringes. For more information about safe sharps disposal, and for specific information about sharps disposal in the state that you live in, go to the FDA's website at: http://www.fda.gov/safesharpsdisposal.
- Do not dispose of your used sharps disposal container in your household trash unless your community guidelines permit this. Do not recycle your used sharps disposal container.
Keep PRALUENT and all medicines out of the reach of children.
This Instructions for Use has been approved by the U.S. Food and Drug Administration.
Manufactured by:
sanofi-aventis U.S. LLC
Bridgewater, NJ 08807
A SANOFI COMPANY
U.S. License # 1752
Marketed by: sanofi-aventis U.S. LLC (Bridgewater, NJ 08807)
and Regeneron Pharmaceuticals, Inc. (Tarrytown, NY 10591)
PRALUENT is a registered trademark of Sanofi
©2018 Regeneron Pharmaceuticals, Inc. / sanofi-aventis U.S. LLC
Revised: December 2018











| PRALUENT
alirocumab injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| PRALUENT
alirocumab injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Sanofi US Corporation (116902801) |
| Registrant - Regeneron Pharmaceuticals, Inc. (194873139) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Regeneron Pharmaceuticals, Inc. | 945589711 | ANALYSIS(72733-5901, 72733-5902) , API MANUFACTURE(72733-5901, 72733-5902) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Sanofi Chimie | 291592785 | ANALYSIS(72733-5901, 72733-5902) , API MANUFACTURE(72733-5901, 72733-5902) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Regn Ireland DAC | 986063166 | ANALYSIS(72733-5901, 72733-5902) , API MANUFACTURE(72733-5901, 72733-5902) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Sanofi-Aventis Deutschland GmbH | 313218430 | ANALYSIS(72733-5901, 72733-5902) , LABEL(72733-5901, 72733-5902) , MANUFACTURE(72733-5901, 72733-5902) , PACK(72733-5901, 72733-5902) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Ireland Limited | 985127419 | ANALYSIS(72733-5901, 72733-5902) , LABEL(72733-5901, 72733-5902) , MANUFACTURE(72733-5901, 72733-5902) , PACK(72733-5901, 72733-5902) | |
