Drug Detail:Synjardy xr (Empagliflozin and metformin [ em-pa-gli-floe-zin-and-met-for-min ])
Drug Class: Antidiabetic combinations
Highlights of Prescribing Information
SYNJARDY® XR (empagliflozin and metformin hydrochloride extended-release tablets), for oral use
Initial U.S. Approval: 2015
WARNING: LACTIC ACIDOSIS
See full prescribing information for complete boxed warning.
- Postmarketing cases of metformin-associated lactic acidosis have resulted in death, hypothermia, hypotension, and resistant bradyarrhythmias. Symptoms included malaise, myalgias, respiratory distress, somnolence, and abdominal pain. Laboratory abnormalities included elevated blood lactate levels, anion gap acidosis, increased lactate/pyruvate ratio; and metformin plasma levels generally >5 mcg/mL. (5.1)
- Risk factors include renal impairment, concomitant use of certain drugs, age ≥65 years old, radiological studies with contrast, surgery and other procedures, hypoxic states, excessive alcohol intake, and hepatic impairment. Steps to reduce the risk of and manage metformin-associated lactic acidosis in these high risk groups are provided in the Full Prescribing Information. (5.1)
- If lactic acidosis is suspected, discontinue SYNJARDY XR and institute general supportive measures in a hospital setting. Prompt hemodialysis is recommended. (5.1)
Recent Major Changes
| Indications and Usage (1) | 2/2023 |
| Dosage and Administration (2.2) | 2/2023 |
| Warnings and Precautions (5.4, 5.6) | 10/2022 |
Indications and Usage for Synjardy XR
SYNJARDY XR
SYNJARDY XR is a combination of empagliflozin, a sodium-glucose co-transporter 2 (SGLT2) inhibitor and metformin hydrochloride (HCl), a biguanide, indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
Empagliflozin
Empagliflozin when used as a component of SYNJARDY XR, is indicated in adults with type 2 diabetes mellitus to reduce the risk of:
- Cardiovascular death in adults with established cardiovascular disease. (1)
- Cardiovascular death and hospitalization for heart failure in adults with heart failure. (1)
Limitations of Use:
- Not recommended for use in patients with type 1 diabetes mellitus. It may increase the risk of diabetic ketoacidosis in these patients. (1)
- Because of the metformin component, SYNJARDY XR is not recommended for use in patients with heart failure without type 2 diabetes mellitus. (1)
Synjardy XR Dosage and Administration
- Assess renal function before initiating and as clinically indicated. (2.1)
- Individualize the starting dosage based on the patient's current regimen and renal function. (2.2, 2.3)
- Initiation is not recommended in patients with an eGFR less than 45 mL/min/1.73 m2, due to the metformin component. (2.3)
- The maximum recommended total daily dosage is 25 mg empagliflozin and 2,000 mg metformin HCl. (2.2)
- Take once daily with a meal in the morning, with gradual dosage escalation to reduce the gastrointestinal side effects due to metformin. (2.2)
- Swallow whole; do not split, crush, dissolve, or chew. (2.2)
- SYNJARDY XR may need to be discontinued at time of, or prior to, iodinated contrast imaging procedures. (2.4)
Dosage Forms and Strengths
Tablets:
- 5 mg empagliflozin/1,000 mg metformin HCl extended-release (3)
- 10 mg empagliflozin/1,000 mg metformin HCl extended-release (3)
- 12.5 mg empagliflozin/1,000 mg metformin HCl extended-release (3)
- 25 mg empagliflozin/1,000 mg metformin HCl extended-release (3)
Contraindications
- Severe renal impairment (eGFR below 30 mL/min/1.73 m2), end stage renal disease, or on dialysis (4, 5.1)
- Metabolic acidosis, including diabetic ketoacidosis (1, 4, 5.1)
- Hypersensitivity to empagliflozin, metformin or any of the excipients in SYNJARDY XR (4)
Warnings and Precautions
- Lactic Acidosis: See boxed warning (5.1)
- Ketoacidosis: Assess patients who present with signs and symptoms of metabolic acidosis for ketoacidosis, regardless of blood glucose level. If suspected, discontinue SYNJARDY XR, evaluate and treat promptly. Before initiating SYNJARDY XR, consider risk factors for ketoacidosis. Patients on SYNJARDY XR may require monitoring and temporary discontinuation of therapy in clinical situations known to predispose to ketoacidosis. (5.2)
- Volume Depletion: Before initiating SYNJARDY XR, assess volume status and renal function in patients with impaired renal function, elderly patients, or patients on loop diuretics. Monitor for signs and symptoms during therapy. (5.3)
- Urosepsis and Pyelonephritis: Evaluate patients for signs and symptoms of urinary tract infections and treat promptly, if indicated (5.4)
- Hypoglycemia: Consider lowering the dosage of insulin secretagogue or insulin to reduce the risk of hypoglycemia when initiating SYNJARDY XR (5.5)
- Necrotizing Fasciitis of the Perineum (Fournier's Gangrene): Serious, life-threatening cases have occurred in both females and males. Assess patients presenting with pain or tenderness, erythema, or swelling in the genital or perineal area, along with fever or malaise. If suspected, institute prompt treatment. (5.6)
- Genital Mycotic Infections: Monitor and treat as appropriate (5.7)
- Hypersensitivity Reactions: Serious hypersensitivity reactions (e.g., angioedema) have occurred with empagliflozin. If hypersensitivity reactions occur, discontinue SYNJARDY XR, treat promptly, and monitor until signs and symptoms resolve. (5.8)
- Vitamin B12 Deficiency: Metformin may lower vitamin B12 levels. Measure hematologic parameters annually and vitamin B12 at 2 to 3 year intervals and manage any abnormalities. (5.9)
Adverse Reactions/Side Effects
- Most common adverse reactions associated with empagliflozin (5% or greater incidence) were urinary tract infection and female genital mycotic infections. (6.1)
- Most common adverse reactions associated with metformin (>5%) are diarrhea, nausea/vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Boehringer Ingelheim Pharmaceuticals, Inc. at 1-800-542-6257 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- Carbonic Anhydrase Inhibitors: May increase risk of lactic acidosis. Consider more frequent monitoring. (7)
- Drugs that Reduce Metformin Clearance: May increase risk of lactic acidosis. Consider benefits and risks of concomitant use. (7)
- See full prescribing information for additional drug interactions and information on interference of SYNJARDY XR with laboratory tests. (7)
Use In Specific Populations
- Pregnancy: Advise females of the potential risk to a fetus especially during the second and third trimesters. (8.1)
- Lactation: Not recommended when breastfeeding. (8.2)
- Females and Males of Reproductive Potential: Advise premenopausal females of the potential for an unintended pregnancy. (8.3)
- Geriatric Patients: Higher incidence of adverse reactions related to volume depletion and reduced renal function. (5.1, 5.3, 8.5, 8.6)
- Renal Impairment: Higher incidence of adverse reactions related to reduced renal function. (5.1, 5.3, 8.6)
- Hepatic Impairment: Avoid use in patients with hepatic impairment. (8.7)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 2/2023
Full Prescribing Information
WARNING: LACTIC ACIDOSIS
Postmarketing cases of metformin-associated lactic acidosis have resulted in death, hypothermia, hypotension, and resistant bradyarrhythmias. The onset of metformin-associated lactic acidosis is often subtle, accompanied only by nonspecific symptoms such as malaise, myalgias, respiratory distress, somnolence, and abdominal pain. Metformin-associated lactic acidosis was characterized by elevated blood lactate levels (>5 mmol/Liter), anion gap acidosis (without evidence of ketonuria or ketonemia), an increased lactate/pyruvate ratio; and metformin plasma levels generally >5 mcg/mL [see Warnings and Precautions (5.1)].
Risk factors for metformin-associated lactic acidosis include renal impairment, concomitant use of certain drugs (e.g., carbonic anhydrase inhibitors such as topiramate), age 65 years old or greater, having a radiological study with contrast, surgery and other procedures, hypoxic states (e.g., acute congestive heart failure), excessive alcohol intake, and hepatic impairment.
Steps to reduce the risk of and manage metformin-associated lactic acidosis in these high risk groups are provided in the full prescribing information [see Dosage and Administration (2.1), Contraindications (4), Warnings and Precautions (5.1), Drug Interactions (7), and Use in Specific Populations (8.6, 8.7)].
If metformin-associated lactic acidosis is suspected, immediately discontinue SYNJARDY XR and institute general supportive measures in a hospital setting. Prompt hemodialysis is recommended [see Warnings and Precautions (5.1)].
2. Synjardy XR Dosage and Administration
2.1 Recommendations Prior to Initiation of SYNJARDY XR
- Assess renal function before initiating SYNJARDY XR and as clinically indicated [see Warnings and Precautions (5.1, 5.3)].
- In patients with volume depletion, correct this condition before initiating SYNJARDY XR [see Warnings and Precautions (5.3) and Use in Specific Populations (8.5, 8.6)].
2.2 Recommended Dosage and Administration
- When switching to SYNJARDY XR from:
- Metformin HCl: initiate SYNJARDY XR at a similar total daily dosage of metformin HCl and a total daily empagliflozin dosage of 10 mg.
- Empagliflozin: initiate SYNJARDY XR at the same total daily dosage of empagliflozin and a total daily metformin HCl dosage of extended-release 1,000 mg.
- Empagliflozin and metformin HCl: initiate SYNJARDY XR at the same total daily dosages of each component.
- Recommended dosage of SYNJARDY XR:
- The recommended dosage of empagliflozin is 10 mg once daily.
- For additional glycemic control, empagliflozin may be increased to a maximum once daily dosage of 25 mg in patients tolerating 10 mg once daily and metformin may be increased to a maximum once daily dosage of 2,000 mg, with gradual escalation to reduce gastrointestinal adverse reactions with metformin [see Adverse Reactions (6.1)].
- Take SYNJARDY XR orally once daily with a meal in the morning.
- Swallow SYNJARDY XR tablets whole. Do not split, crush, dissolve, or chew.
2.3 Dosage Recommendations in Patients with Renal Impairment
- Initiation of SYNJARDY XR is not recommended in patients with an eGFR less than 45 mL/min/1.73 m2, due to the metformin component.
- SYNJARDY XR is contraindicated in patients with an eGFR less than 30 mL/min/1.73 m2 or in patients on dialysis [see Contraindications (4), Warnings and Precautions (5.1) and Use in Specific Populations (8.6)].
2.4 Discontinuation for Iodinated Contrast Imaging Procedures
Discontinue SYNJARDY XR at the time of, or prior to, an iodinated contrast imaging procedure in patients with an eGFR less than 60 mL/min/1.73 m2; in patients with a history of liver disease, alcoholism or heart failure; or in patients who will be administered intra-arterial iodinated contrast. Re-evaluate eGFR 48 hours after the imaging procedure; restart SYNJARDY XR if renal function is stable [see Warnings and Precautions (5.1)].
3. Dosage Forms and Strengths
SYNJARDY XR Tablets:
| Empagliflozin Strength | Metformin HCl Strength | Color/Shape | Tablet Markings |
|---|---|---|---|
| 5 mg | 1,000 mg | olive green, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S5" on the top line and "1000 M" on the bottom line. |
| 10 mg | 1,000 mg | orange, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S10" on the top line and "1000 M" on the bottom line. |
| 12.5 mg | 1,000 mg | blue, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S12" on the top line and "1000 M" on the bottom line. |
| 25 mg | 1,000 mg | light green, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S25" on the top line and "1000 M" on the bottom line. |
4. Contraindications
SYNJARDY XR is contraindicated in patients with:
- Severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage renal disease, or dialysis [see Warnings and Precautions (5.1) and Use in Specific Populations (8.6)].
- Acute or chronic metabolic acidosis, including diabetic ketoacidosis [see Warnings and Precautions (5.1)].
- Hypersensitivity to empagliflozin, metformin or any of the excipients in SYNJARDY XR, reactions such as angioedema have occurred [see Warnings and Precautions (5.8)].
5. Warnings and Precautions
5.1 Lactic Acidosis
There have been postmarketing cases of metformin-associated lactic acidosis, including fatal cases. These cases had a subtle onset and were accompanied by nonspecific symptoms such as malaise, myalgias, abdominal pain, respiratory distress, or increased somnolence; however, hypothermia, hypotension, and resistant bradyarrhythmias have occurred with severe acidosis. Metformin-associated lactic acidosis was characterized by elevated blood lactate concentrations (>5 mmol/Liter), anion gap acidosis (without evidence of ketonuria or ketonemia), and an increased lactate:pyruvate ratio; metformin plasma levels generally >5 mcg/mL. Metformin decreases liver uptake of lactate increasing lactate blood levels which may increase the risk of lactic acidosis, especially in patients at risk.
If metformin-associated lactic acidosis is suspected, general supportive measures should be instituted promptly in a hospital setting, along with immediate discontinuation of SYNJARDY XR. In SYNJARDY XR-treated patients with a diagnosis or strong suspicion of lactic acidosis, prompt hemodialysis is recommended to correct the acidosis and remove accumulated metformin (metformin is dialyzable, with a clearance of up to 170 mL/minute under good hemodynamic conditions). Hemodialysis has often resulted in reversal of symptoms and recovery.
Educate patients and their families about the symptoms of lactic acidosis and if these symptoms occur instruct them to discontinue SYNJARDY XR and report these symptoms to their healthcare provider.
For each of the known and possible risk factors for metformin-associated lactic acidosis, recommendations to reduce the risk of and manage metformin-associated lactic acidosis are provided below:
5.2 Ketoacidosis
Reports of ketoacidosis, a serious life-threatening condition requiring urgent hospitalization have been identified in clinical trials and postmarketing surveillance in patients with type 1 and type 2 diabetes mellitus receiving sodium glucose co-transporter-2 (SGLT2) inhibitors, including empagliflozin. Fatal cases of ketoacidosis have been reported in patients taking empagliflozin. In placebo-controlled trials of patients with type 1 diabetes, the risk of ketoacidosis was increased in patients who received SGLT2 inhibitors compared to patients who received placebo. SYNJARDY XR is not indicated for the treatment of patients with type 1 diabetes mellitus [see Indications and Usage (1)].
Patients treated with SYNJARDY XR who present with signs and symptoms consistent with severe metabolic acidosis should be assessed for ketoacidosis regardless of presenting blood glucose levels, as ketoacidosis associated with SYNJARDY XR may be present even if blood glucose levels are less than 250 mg/dL. If ketoacidosis is suspected, SYNJARDY XR should be discontinued, patient should be evaluated, and prompt treatment should be instituted. Treatment of ketoacidosis may require insulin, fluid and carbohydrate replacement.
In many of the postmarketing reports, and particularly in patients with type 1 diabetes, the presence of ketoacidosis was not immediately recognized and institution of treatment was delayed because presenting blood glucose levels were below those typically expected for diabetic ketoacidosis (often less than 250 mg/dL). Signs and symptoms at presentation were consistent with dehydration and severe metabolic acidosis and included nausea, vomiting, abdominal pain, generalized malaise, and shortness of breath. In some but not all cases, factors predisposing to ketoacidosis such as insulin dosage reduction, acute febrile illness, reduced caloric intake, surgery, pancreatic disorders suggesting insulin deficiency (e.g., type 1 diabetes, history of pancreatitis or pancreatic surgery), and alcohol abuse were identified.
Before initiating SYNJARDY XR, consider factors in the patient history that may predispose to ketoacidosis including pancreatic insulin deficiency from any cause, caloric restriction, and alcohol abuse.
For patients who undergo scheduled surgery, consider temporarily discontinuing SYNJARDY XR for at least 3 days prior to surgery [see Clinical Pharmacology (12.2, 12.3)].
Consider monitoring for ketoacidosis and temporarily discontinuing SYNJARDY XR in other clinical situations known to predispose to ketoacidosis (e.g., prolonged fasting due to acute illness or post-surgery). Ensure risk factors for ketoacidosis are resolved prior to restarting SYNJARDY XR.
Educate patients on the signs and symptoms of ketoacidosis and instruct patients to discontinue SYNJARDY XR and seek medical attention immediately if signs and symptoms occur.
5.3 Volume Depletion
Empagliflozin can cause intravascular volume depletion which may sometimes manifest as symptomatic hypotension or acute transient changes in creatinine [see Adverse Reactions (6.1)]. There have been post-marketing reports of acute kidney injury, some requiring hospitalization and dialysis, in patients with type 2 diabetes mellitus receiving SGLT2 inhibitors, including empagliflozin. Patients with impaired renal function (eGFR less than 60 mL/min/1.73 m2), elderly patients, or patients on loop diuretics may be at increased risk for volume depletion or hypotension. Before initiating SYNJARDY XR in patients with one or more of these characteristics, assess volume status and renal function. In patients with volume depletion, correct this condition before initiating SYNJARDY XR. Monitor for signs and symptoms of volume depletion, and renal function after initiating therapy.
5.4 Urosepsis and Pyelonephritis
There have been reports of serious urinary tract infections including urosepsis and pyelonephritis requiring hospitalization in patients receiving empagliflozin. Treatment with empagliflozin increases the risk for urinary tract infections. Evaluate patients for signs and symptoms of urinary tract infections and treat promptly, if indicated [see Adverse Reactions (6)].
5.5 Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues
Insulin and insulin secretagogues are known to cause hypoglycemia. The risk of hypoglycemia is increased when SYNJARDY XR is used in combination with insulin secretagogues (e.g., sulfonylurea) or insulin [see Adverse Reactions (6.1)]. Therefore, a lower dosage of the insulin secretagogue or insulin may be required to reduce the risk of hypoglycemia when used in combination with SYNJARDY XR.
5.6 Necrotizing Fasciitis of the Perineum (Fournier's Gangrene)
Reports of necrotizing fasciitis of the perineum (Fournier's gangrene), a rare but serious and life-threatening necrotizing infection requiring urgent surgical intervention, have been identified in patients with diabetes mellitus receiving SGLT2 inhibitors, including empagliflozin. Cases have been reported in both females and males. Serious outcomes have included hospitalization, multiple surgeries, and death.
Patients treated with SYNJARDY XR presenting with pain or tenderness, erythema, or swelling in the genital or perineal area, along with fever or malaise, should be assessed for necrotizing fasciitis. If suspected, start treatment immediately with broad-spectrum antibiotics and, if necessary, surgical debridement. Discontinue SYNJARDY XR, closely monitor blood glucose levels, and provide appropriate alternative therapy for glycemic control.
5.7 Genital Mycotic Infections
Empagliflozin increases the risk for genital mycotic infections [see Adverse Reactions (6.1)]. Patients with a history of chronic or recurrent genital mycotic infections were more likely to develop genital mycotic infections. Monitor and treat as appropriate.
5.8 Hypersensitivity Reactions
There have been postmarketing reports of serious hypersensitivity reactions, (e.g., angioedema) in patients treated with empagliflozin. If a hypersensitivity reaction occurs, discontinue SYNJARDY XR; treat promptly per standard of care, and monitor until signs and symptoms resolve. SYNJARDY XR is contraindicated in patients with hypersensitivity to empagliflozin or any of the excipients in SYNJARDY XR [see Contraindications (4)].
5.9 Vitamin B12 Deficiency
In metformin clinical trials of 29-week duration, a decrease to subnormal levels of previously normal serum vitamin B12 levels was observed in approximately 7% of metformin-treated patients. Such decrease, possibly due to interference with B12 absorption from the B12-intrinsic factor complex, may be associated with anemia but appears to be rapidly reversible with discontinuation of metformin or vitamin B12 supplementation. Certain individuals (those with inadequate vitamin B12 or calcium intake or absorption) appear to be predisposed to developing subnormal vitamin B12 levels. Measure hematologic parameters on an annual basis and vitamin B12 at 2 to 3 year intervals in patients on SYNJARDY XR and manage any abnormalities [see Adverse Reactions (6.1)].
6. Adverse Reactions/Side Effects
The following important adverse reactions are described below and elsewhere in the labeling:
- Lactic Acidosis [see Boxed Warning and Warnings and Precautions (5.1)]
- Ketoacidosis [see Warnings and Precautions (5.2)]
- Volume Depletion [see Warnings and Precautions (5.3)]
- Urosepsis and Pyelonephritis [see Warnings and Precautions (5.4)]
- Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues [see Warnings and Precautions (5.5)]
- Necrotizing Fasciitis of the Perineum (Fournier's Gangrene) [see Warnings and Precautions (5.6)]
- Genital Mycotic Infections [see Warnings and Precautions (5.7)]
- Hypersensitivity Reactions [see Warnings and Precautions (5.8)]
- Vitamin B12 Deficiency [see Warnings and Precautions (5.9)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of concomitantly administered empagliflozin (daily dosage 10 mg or 25 mg) and metformin hydrochloride (mean daily dosage of approximately 1,800 mg) has been evaluated in 3,456 adult patients with type 2 diabetes mellitus treated for 16 to 24 weeks, of which 926 patients received placebo, 1,271 patients received a daily dosage of empagliflozin 10 mg, and 1,259 patients received a daily dosage of empagliflozin 25 mg. Discontinuation of therapy due to adverse events across treatment groups was 3.0%, 2.8%, and 2.9% for placebo, empagliflozin 10 mg, and empagliflozin 25 mg, respectively.
Adverse Reactions in a Clinical Trial with Empagliflozin (Add-On Combination Therapy with Metformin and Sulfonylurea) for Glycemic Control in Adults with Type 2 Diabetes Mellitus
In a 24-week placebo-controlled trial of empagliflozin 10 mg or 25 mg administered once daily added to metformin and sulfonylurea, adverse reactions reported in ≥5% of empagliflozin-treated patients and more commonly than in placebo-treated patients are presented in Table 1 (see also Table 4).
| Adverse Reactions | Placebo + metformin and sulfonylurea (%) n=225 | Empagliflozin 10 mg + metformin and sulfonylurea (%) n=224 | Empagliflozin 25 mg + metformin and sulfonylurea (%) n=217 |
|---|---|---|---|
| Hypoglycemia | 9.8 | 15.6 | 12.9 |
| Urinary tract infection | 6.7 | 9.4 | 6.9 |
| Nasopharyngitis | 4.9 | 8.0 | 6.0 |
Empagliflozin
Clinical Trials in Patients with Type 2 Diabetes Mellitus
The data in Table 2 are derived from a pool of four 24-week placebo-controlled trials and 18-week data from a placebo-controlled trial with basal insulin in adult patients with type 2 diabetes mellitus. Empagliflozin was used as monotherapy in one trial and as add-on therapy in four trials [see Clinical Studies (14)].
These data reflect exposure of 1,976 patients to empagliflozin with a mean exposure duration of approximately 23 weeks. Patients received placebo (N=995), empagliflozin 10 mg (N=999), or empagliflozin 25 mg (N=977) once daily. The mean age of the population was 56 years and 3% were older than 75 years of age. More than half (55%) of the population was male; 46% were White, 50% were Asian, and 3% were Black or African American. At baseline, 57% of the population had diabetes more than 5 years and had a mean hemoglobin A1c (HbA1c) of 8%. Established microvascular complications of diabetes at baseline included diabetic nephropathy (7%), retinopathy (8%), or neuropathy (16%). Baseline renal function was normal or mildly impaired in 91% of patients and moderately impaired in 9% of patients (mean eGFR 86.8 mL/min/1.73 m2).
Table 2 shows adverse reactions (excluding hypoglycemia) that were not present at baseline, occurred more commonly in empagliflozin-treated patients than placebo-treated patients, and occurred in greater than or equal to 2% of empagliflozin-treated patients.
| Adverse Reactions | Placebo (%) N=995 | Empagliflozin 10 mg (%) N=999 | Empagliflozin 25 mg (%) N=977 |
|---|---|---|---|
| aPredefined adverse event grouping, including, but not limited to, urinary tract infection, asymptomatic bacteriuria, cystitis bFemale genital mycotic infections include the following adverse reactions: vulvovaginal mycotic infection, vaginal infection, vulvitis, vulvovaginal candidiasis, genital infection, genital candidiasis, genital infection fungal, genitourinary tract infection, vulvovaginitis, cervicitis, urogenital infection fungal, vaginitis bacterial. Percentages calculated with the number of female subjects in each group as denominator: placebo (N=481), empagliflozin 10 mg (N=443), empagliflozin 25 mg (N=420). cPredefined adverse event grouping, including, but not limited to, polyuria, pollakiuria, and nocturia dMale genital mycotic infections include the following adverse reactions: balanoposthitis, balanitis, genital infections fungal, genitourinary tract infection, balanitis candida, scrotal abscess, penile infection. Percentages calculated with the number of male subjects in each group as denominator: placebo (N=514), empagliflozin 10 mg (N=556), empagliflozin 25 mg (N=557). |
|||
| Urinary tract infectiona | 7.6 | 9.3 | 7.6 |
| Female genital mycotic infectionsb | 1.5 | 5.4 | 6.4 |
| Upper respiratory tract infection | 3.8 | 3.1 | 4.0 |
| Increased urinationc | 1.0 | 3.4 | 3.2 |
| Dyslipidemia | 3.4 | 3.9 | 2.9 |
| Arthralgia | 2.2 | 2.4 | 2.3 |
| Male genital mycotic infectionsd | 0.4 | 3.1 | 1.6 |
| Nausea | 1.4 | 2.3 | 1.1 |
Thirst (including polydipsia) was reported in 0%, 1.7%, and 1.5% for placebo, empagliflozin 10 mg, and empagliflozin 25 mg, respectively.
Hypoglycemia in Clinical Trials with Empagliflozin for Glycemic Control in Adults with Type 2 Diabetes Mellitus
The incidence of hypoglycemia by study is shown in Table 3. The incidence of hypoglycemia increased when empagliflozin was administered with insulin or sulfonylurea.
| aOverall hypoglycemic events: plasma or capillary glucose of less than or equal to 70 mg/dL bSevere hypoglycemic events: requiring assistance regardless of blood glucose cTreated set (patients who had received at least one dosage of study drug) dInsulin dosage could not be adjusted during the initial 18-week treatment period |
|||
| Monotherapy (24 weeks) | Placebo (n=229) | Empagliflozin 10 mg (n=224) | Empagliflozin 25 mg (n=223) |
| Overall (%) | 0.4 | 0.4 | 0.4 |
| Severe (%) | 0 | 0 | 0 |
| In Combination with Metformin (24 weeks) | Placebo + Metformin (n=206) | Empagliflozin 10 mg + Metformin (n=217) | Empagliflozin 25 mg + Metformin (n=214) |
| Overall (%) | 0.5 | 1.8 | 1.4 |
| Severe (%) | 0 | 0 | 0 |
| In Combination with Metformin + Sulfonylurea (24 weeks) | Placebo (n=225) | Empagliflozin 10 mg + Metformin + Sulfonylurea (n=224) | Empagliflozin 25 mg + Metformin + Sulfonylurea (n=217) |
| Overall (%) | 8.4 | 16.1 | 11.5 |
| Severe (%) | 0 | 0 | 0 |
| In Combination with Pioglitazone +/- Metformin (24 weeks) | Placebo (n=165) | Empagliflozin 10 mg + Pioglitazone +/- Metformin (n=165) | Empagliflozin 25 mg + Pioglitazone +/- Metformin (n=168) |
| Overall (%) | 1.8 | 1.2 | 2.4 |
| Severe (%) | 0 | 0 | 0 |
| In Combination with Basal Insulin +/-Metformin (18 weeksd) | Placebo (n=170) | Empagliflozin 10 mg (n=169) | Empagliflozin 25 mg (n=155) |
| Overall (%) | 20.6 | 19.5 | 28.4 |
| Severe (%) | 0 | 0 | 1.3 |
| In Combination with MDI Insulin +/-Metformin (18 weeksd) | Placebo (n=188) | Empagliflozin 10 mg (n=186) | Empagliflozin 25 mg (n=189) |
| Overall (%) | 37.2 | 39.8 | 41.3 |
| Severe (%) | 0.5 | 0.5 | 0.5 |
6.2 Postmarketing Experience
Additional adverse reactions have been identified during postapproval use. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7. Drug Interactions
See Table 4 for clinically relevant interactions with SYNJARDY XR.
| Carbonic Anhydrase Inhibitors | |
| Clinical Impact | Topiramate or other carbonic anhydrase inhibitors (e.g., zonisamide, acetazolamide or dichlorphenamide) frequently causes a decrease in serum bicarbonate and induce non-anion gap, hyperchloremic metabolic acidosis. Concomitant use of these drugs with SYNJARDY XR may increase the risk of lactic acidosis. |
| Intervention | Consider more frequent monitoring of these patients. |
| Drugs that Reduce Metformin Clearance | |
| Clinical Impact | Concomitant use of drugs that interfere with common renal tubular transport systems involved in the renal elimination of metformin (e.g., organic cationic transporter-2 [OCT2] / multidrug and toxin extrusion [MATE] inhibitors such as ranolazine, vandetanib, dolutegravir, and cimetidine) could increase systemic exposure to metformin and may increase the risk for lactic acidosis [see Clinical Pharmacology (12.3)]. |
| Intervention | Consider the benefits and risks of concomitant use. |
| Alcohol | |
| Clinical Impact | Alcohol is known to potentiate the effect of metformin on lactate metabolism. |
| Intervention | Warn patients against excessive alcohol intake while receiving SYNJARDY XR. |
| Diuretics | |
| Clinical Impact | Coadministration of empagliflozin with diuretics resulted in increased urine volume and frequency of voids, which might enhance the potential for volume depletion. |
| Intervention | Before initiating SYNJARDY XR, assess volume status and renal function. In patients with volume depletion, correct this condition before initiating SYNJARDY XR. Monitor for signs and symptoms of volume depletion, and renal function after initiating therapy. |
| Insulin or Insulin Secretagogues | |
| Clinical Impact | The risk of hypoglycemia is increased when SYNJARDY XR is used in combination with insulin secretagogues (e.g., sulfonylurea) or insulin. |
| Intervention | Coadministration of SYNJARDY XR with an insulin secretagogue (e.g., sulfonylurea) or insulin may require lower dosages of the insulin secretagogue or insulin to reduce the risk of hypoglycemia. |
| Drugs Affecting Glycemic Control | |
| Clinical Impact | Certain drugs tend to produce hyperglycemia and may lead to loss of glycemic control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid. |
| Intervention | When such drugs are administered to a patient receiving SYNJARDY XR, the patient should be closely observed to maintain adequate glycemic control. When such drugs are withdrawn from a patient receiving SYNJARDY XR, the patient should be observed closely for hypoglycemia. |
| Lithium | |
| Clinical Impact | Concomitant use of an SGLT2 inhibitor with lithium may decrease serum lithium concentrations. |
| Intervention | Monitor serum lithium concentration more frequently during SYNJARDY XR initiation and dosage changes. |
| Positive Urine Glucose Test | |
| Clinical Impact | SGLT2 inhibitors increase urinary glucose excretion and will lead to positive urine glucose tests. |
| Intervention | Monitoring glycemic control with urine glucose tests is not recommended in patients taking SGLT2 inhibitors. Use alternative methods to monitor glycemic control. |
| Interference with 1,5-anhydroglucitol (1,5-AG) Assay | |
| Clinical Impact | Measurements of 1,5-AG are unreliable in assessing glycemic control in patients taking SGLT2 inhibitors. |
| Intervention | Monitoring glycemic control with 1,5-AG assay is not recommended. Use alternative methods to monitor glycemic control. |
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
Based on animal data showing adverse renal effects from empagliflozin, SYNJARDY XR is not recommended during the second and third trimesters of pregnancy.
The limited available data with SYNJARDY XR or empagliflozin in pregnant women are not sufficient to determine a drug-associated risk for major birth defects and miscarriage. Published studies with metformin use during pregnancy have not reported a clear association with metformin and major birth defect or miscarriage risk (see Data). There are risks to the mother and fetus associated with poorly controlled diabetes in pregnancy (see Clinical Considerations).
In animal studies, empagliflozin, a component of SYNJARDY XR, resulted in adverse renal changes in rats when administered during a period of renal development corresponding to the late second and third trimesters of human pregnancy. Doses approximately 13-times the maximum clinical dose caused renal pelvic and tubule dilatations that were reversible. No adverse developmental effects were observed when metformin was administered to pregnant rats or rabbits (see Data).
The estimated background risk of major birth defects is 6% to 10% in women with pre-gestational diabetes with a HbA1c >7 and has been reported to be as high as 20% to 25% in women with HbA1c >10. The estimated background risk of miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
8.2 Lactation
Data
Published clinical lactation studies report that metformin is present in human milk which resulted in infant doses approximately 0.11% to 1% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 0.13 and 1. However, the studies were not designed to definitely establish the risk of use of metformin during lactation because of small sample size and limited adverse event data collected in infants.
Empagliflozin was present at a low level in rat fetal tissues after a single oral dose to the dams at gestation day 18. In rat milk, the mean milk to plasma ratio ranged from 0.634 to 5, and was greater than one from 2 to 24 hours post-dose. The mean maximal milk to plasma ratio of 5 occurred at 8 hours post-dose, suggesting accumulation of empagliflozin in the milk. Juvenile rats directly exposed to empagliflozin showed a risk to the developing kidney (renal pelvic and tubular dilatations) during maturation.
8.3 Females and Males of Reproductive Potential
Discuss the potential for unintended pregnancy with premenopausal women as therapy with metformin may result in ovulation in some anovulatory women.
8.4 Pediatric Use
Safety and effectiveness of SYNJARDY XR have not been established in pediatric patients.
8.5 Geriatric Use
Assess renal function more frequently in SYNJARDY XR-treated geriatric patients because there is a greater risk of empagliflozin-associated intravascular volume contraction and symptomatic hypotension in geriatric patients and there is a greater risk of metformin-associated lactic acidosis in geriatric patients [see Warnings and Precautions (5.1, 5.3)].
The recommended dosage for the metformin component of SYNJARDY XR in geriatric patients should usually start at the lower end of the dosage range.
10. Overdosage
In the event of an overdose with SYNJARDY XR, consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdosage management recommendations.
Overdose of metformin HCl has occurred, including ingestion of amounts greater than 50 grams. Lactic acidosis has been reported in approximately 32% of metformin overdose cases [see Warnings and Precautions (5.1)]. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis may be useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
Removal of empagliflozin by hemodialysis has not been studied.
11. Synjardy XR Description
SYNJARDY XR tablets for oral use contain: empagliflozin and metformin hydrochloride.
12. Synjardy XR - Clinical Pharmacology
12.1 Mechanism of Action
12.3 Pharmacokinetics
Empagliflozin
Metformin
Specific Populations
Drug Interactions
Pharmacokinetic drug interaction studies with SYNJARDY XR have not been performed; however, such studies have been conducted with the individual components empagliflozin and metformin HCl.
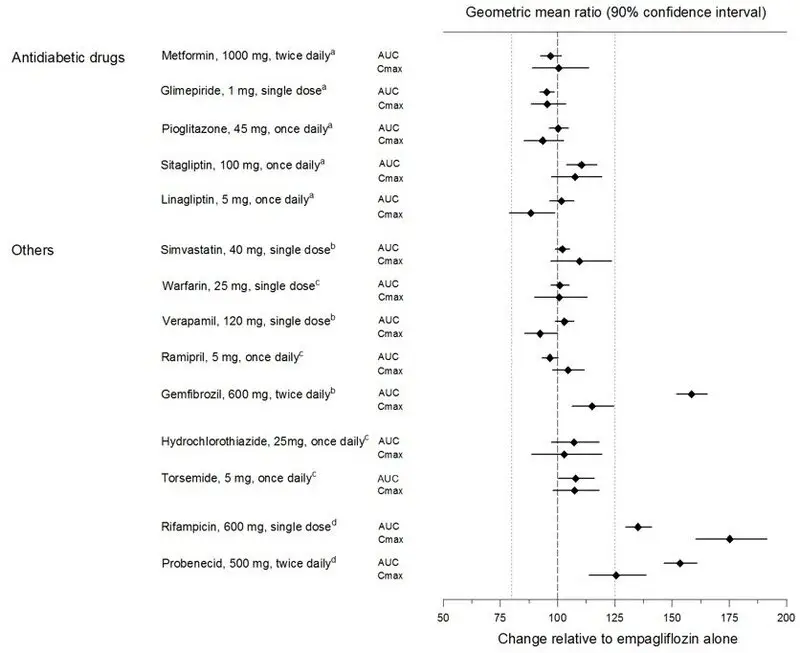
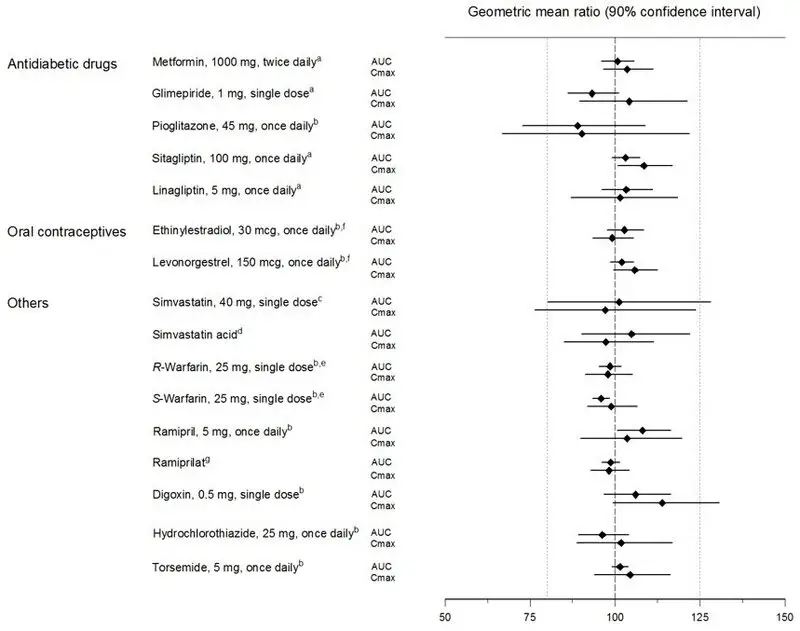
Empagliflozin
Metformin hydrochloride
| Coadministered Drug | Dose of Coadministered Drug* | Dose of Metformin hydrochloride* | Geometric Mean Ratio (ratio with/without coadministered drug) No effect=1.0 |
||
|---|---|---|---|---|---|
| AUC† | Cmax | ||||
| * All metformin and coadministered drugs were given as single doses | |||||
| † AUC = AUC(INF) | |||||
| ≠ Metformin hydrochloride extended-release tablets 500 mg | |||||
| ‡ Ratio of arithmetic means | |||||
| **At steady-state with topiramate 100 mg every 12 hours and metformin 500 mg every 12 hours; AUC = AUC(0-12 hours) | |||||
| Glyburide | 5 mg | 500 mg≠ | metformin | 0.98‡ | 0.99‡ |
| Furosemide | 40 mg | 850 mg | metformin | 1.09‡ | 1.22‡ |
| Nifedipine | 10 mg | 850 mg | metformin | 1.16 | 1.21 |
| Propranolol | 40 mg | 850 mg | metformin | 0.90 | 0.94 |
| Ibuprofen | 400 mg | 850 mg | metformin | 1.05‡ | 1.07‡ |
| Cationic drugs eliminated by renal tubular secretion may reduce metformin elimination [see Drug Interactions (7)]. | |||||
| Cimetidine | 400 mg | 850 mg | metformin | 1.40 | 1.61 |
| Carbonic anhydrase inhibitors may cause metabolic acidosis [see Drug Interactions (7)]. | |||||
| Topiramate** | 100 mg | 500 mg | metformin | 1.25 | 1.17 |
| Coadministered Drug | Dose of Coadministered Drug* | Dose of Metformin hydrochloride* | Geometric Mean Ratio (ratio with/without metformin) No effect=1.0 |
||
|---|---|---|---|---|---|
| AUC† | Cmax | ||||
| * All metformin and coadministered drugs were given as single doses | |||||
| † AUC = AUC(INF) unless otherwise noted | |||||
| § AUC(0-24 hours) reported | |||||
| ‡ Ratio of arithmetic means, p-value of difference <0.05 | |||||
| ¶ Ratio of arithmetic means | |||||
| Glyburide | 5 mg | 500 mg§ | glyburide | 0.78‡ | 0.63‡ |
| Furosemide | 40 mg | 850 mg | furosemide | 0.87‡ | 0.69‡ |
| Nifedipine | 10 mg | 850 mg | nifedipine | 1.10§ | 1.08 |
| Propranolol | 40 mg | 850 mg | propranolol | 1.01§ | 0.94 |
| Ibuprofen | 400 mg | 850 mg | ibuprofen | 0.97¶ | 1.01¶ |
| Cimetidine | 400 mg | 850 mg | cimetidine | 0.95§ | 1.01 |
14. Clinical Studies
14.1 Glycemic Control Studies in Adult Patients with Type 2 Diabetes Mellitus
In adult patients with type 2 diabetes mellitus, treatment with empagliflozin and metformin produced clinically and statistically significant improvements in HbA1c compared to placebo and metformin. Reductions in HbA1c were observed across subgroups including age, sex, race, and baseline BMI.
Empagliflozin Add-On Combination Therapy with Metformin in Adult Patients with Type 2 Diabetes Mellitus
A total of 637 patients with type 2 diabetes mellitus participated in a double-blind, placebo-controlled study to evaluate the efficacy of empagliflozin in combination with metformin.
Patients with type 2 diabetes mellitus inadequately controlled on at least 1,500 mg of metformin HCl per day entered an open-label 2-week placebo run-in. At the end of the run-in period, patients who remained inadequately controlled and had an HbA1c between 7% and 10% were randomized to placebo, empagliflozin 10 mg, or empagliflozin 25 mg.
At Week 24, treatment with empagliflozin 10 mg or 25 mg daily provided statistically significant reductions in HbA1c (p-value <0.0001), FPG, and body weight compared with placebo (see Table 7).
| Empagliflozin 10 mg + Metformin N=217 | Empagliflozin 25 mg + Metformin N=213 | Placebo + Metformin N=207 |
|
|---|---|---|---|
| aModified intent-to-treat population. Last observation on study (LOCF) was used to impute missing data at Week 24. At Week 24, 9.7%, 14.1%, and 24.6% was imputed for patients randomized to empagliflozin 10 mg, empagliflozin 25 mg, and placebo, respectively. | |||
| bANCOVA p-value <0.0001 (HbA1c: ANCOVA model includes baseline HbA1c, treatment, renal function, and region. Body weight and FPG: same model used as for HbA1c but additionally including baseline body weight/baseline FPG, respectively.) | |||
| cFPG (mg/dL); for empagliflozin 10 mg, n=216, for empagliflozin 25 mg, n=213, and for placebo, n=207 | |||
| HbA1c (%)a | |||
| Baseline (mean) | 7.9 | 7.9 | 7.9 |
| Change from baseline (adjusted mean) | -0.7 | -0.8 | -0.1 |
| Difference from placebo + metformin (adjusted mean) (95% CI) | -0.6b (-0.7, -0.4) | -0.6b (-0.8, -0.5) | -- |
| Patients [n (%)] achieving HbA1c <7% | 75 (38%) | 74 (39%) | 23 (13%) |
| FPG (mg/dL)c | |||
| Baseline (mean) | 155 | 149 | 156 |
| Change from baseline (adjusted mean) | -20 | -22 | 6 |
| Difference from placebo + metformin (adjusted mean) | -26 | -29 | -- |
| Body Weight | |||
| Baseline mean in kg | 82 | 82 | 80 |
| % change from baseline (adjusted mean) | -2.5 | -2.9 | -0.5 |
| Difference from placebo (adjusted mean) (95% CI) | -2.0b (-2.6, -1.4) | -2.5b (-3.1, -1.9) | -- |
At Week 24, the systolic blood pressure was statistically significantly reduced compared to placebo by -4.1 mmHg (placebo-corrected, p-value <0.0001) for empagliflozin 10 mg and -4.8 mmHg (placebo-corrected, p-value <0.0001) for empagliflozin 25 mg.
Empagliflozin Initial Combination Therapy with Metformin
A total of 1,364 patients with type 2 diabetes mellitus participated in a double-blind, randomized, active-controlled study to evaluate the efficacy of empagliflozin in combination with metformin as initial therapy compared to the corresponding individual components.
Treatment-naïve patients with inadequately controlled type 2 diabetes mellitus entered an open-label placebo run-in for 2 weeks. At the end of the run-in period, patients who remained inadequately controlled and had an HbA1c between 7% and 10.5% were randomized to one of 8 active-treatment arms: empagliflozin 10 mg or 25 mg; metformin hydrochloride 1,000 mg, or 2,000 mg; empagliflozin 10 mg in combination with 1,000 mg or 2,000 mg metformin; or empagliflozin 25 mg in combination with 1,000 mg or 2,000 mg metformin hydrochloride.
At Week 24, initial therapy of empagliflozin in combination with metformin provided statistically significant reductions in HbA1c (p-value <0.01) compared to the individual components (see Table 8).
| Empagliflozin 10 mg + Metformin 1,000 mga
N=161 | Empagliflozin 10 mg + Metformin 2,000 mga
N=167 | Empagliflozin 25 mg + Metformin 1,000 mga
N=165 | Empagliflozin 25 mg + Metformin 2,000 mga
N=169 | Empagliflozin 10 mg N=169 | Empagliflozin 25 mg N=163 | Metformin 1,000 mga
N=167 | Metformin 2,000 mga
N=162 |
|
|---|---|---|---|---|---|---|---|---|
| aMetformin hydrochloride total daily dose, administered in two equally divided doses per day. | ||||||||
| bp-value ≤0.0062 (modified intent-to-treat population [observed case] MMRM model included treatment, renal function, region, visit, visit by treatment interaction, and baseline HbA1c). | ||||||||
| cp-value ≤0.0056 (modified intent-to-treat population [observed case] MMRM model included treatment, renal function, region, visit, visit by treatment interaction, and baseline HbA1c). | ||||||||
| HbA1c (%) | ||||||||
| Baseline (mean) | 8.7 | 8.7 | 8.8 | 8.7 | 8.6 | 8.9 | 8.7 | 8.6 |
| Change from baseline (adjusted mean) | -2.0 | -2.1 | -1.9 | -2.1 | -1.4 | -1.4 | -1.2 | -1.8 |
| Comparison vs empagliflozin (adjusted mean) (95% CI) | -0.6b
(-0.9, -0.4) | -0.7b
(-1.0, -0.5) | -0.6c
(-0.8, -0.3) | -0.7c
(-1.0, -0.5) | -- | -- | -- | -- |
| Comparison vs metformin (adjusted mean) (95% CI) | -0.8b
(-1.0, -0.6) | -0.3b
(-0.6, -0.1) | -0.8c
(-1.0, -0.5) | -0.3c
(-0.6, -0.1) | -- | -- | -- | -- |
| Patients [n (%)] achieving HbA1c <7% | 96 (63%) | 112 (70%) | 91 (57%) | 111 (68%) | 69 (43%) | 51 (32%) | 63 (38%) | 92 (58%) |
Empagliflozin Add-On Combination Therapy with Metformin and Sulfonylurea
A total of 666 patients with type 2 diabetes mellitus participated in a double-blind, placebo-controlled study to evaluate the efficacy of empagliflozin in combination with metformin plus a sulfonylurea.
Patients with inadequately controlled type 2 diabetes mellitus on at least 1,500 mg per day of metformin HCl and on a sulfonylurea, entered a 2-week open-label placebo run-in. At the end of the run-in, patients who remained inadequately controlled and had an HbA1c between 7% and 10% were randomized to placebo, empagliflozin 10 mg, or empagliflozin 25 mg.
Treatment with empagliflozin 10 mg or 25 mg daily provided statistically significant reductions in HbA1c (p-value <0.0001), FPG, and body weight compared with placebo (see Table 9).
| Empagliflozin 10 mg + Metformin + SU N=225 | Empagliflozin 25 mg + Metformin + SU N=216 | Placebo + Metformin + SU N=225 |
|
|---|---|---|---|
| aModified intent-to-treat population. Last observation on study (LOCF) was used to impute missing data at Week 24. At Week 24, 17.8%, 16.7%, and 25.3% was imputed for patients randomized to empagliflozin 10 mg, empagliflozin 25 mg, and placebo, respectively. | |||
| bANCOVA p-value <0.0001 (HbA1c: ANCOVA model includes baseline HbA1c, treatment, renal function, and region. Body weight and FPG: same model used as for HbA1c but additionally including baseline body weight/baseline FPG, respectively.) | |||
| cFPG (mg/dL); for empagliflozin 10 mg, n=225, for empagliflozin 25 mg, n=215, for placebo, n=224 | |||
| HbA1c (%)a | |||
| Baseline (mean) | 8.1 | 8.1 | 8.2 |
| Change from baseline (adjusted mean) | -0.8 | -0.8 | -0.2 |
| Difference from placebo (adjusted mean) (95% CI) | -0.6b (-0.8, -0.5) | -0.6b (-0.7, -0.4) | -- |
| Patients [n (%)] achieving HbA1c <7% | 55 (26%) | 65 (32%) | 20 (9%) |
| FPG (mg/dL)c | |||
| Baseline (mean) | 151 | 156 | 152 |
| Change from baseline (adjusted mean) | -23 | -23 | 6 |
| Difference from placebo (adjusted mean) | -29 | -29 | -- |
| Body Weight | |||
| Baseline mean in kg | 77 | 78 | 76 |
| % change from baseline (adjusted mean) | -2.9 | -3.2 | -0.5 |
| Difference from placebo (adjusted mean) (95% CI) | -2.4b (-3.0, -1.8) | -2.7b (-3.3, -2.1) | -- |
Active-Controlled Study vs Glimepiride in Combination with Metformin
The efficacy of empagliflozin was evaluated in a double-blind, glimepiride-controlled, study in 1,545 patients with type 2 diabetes mellitus with insufficient glycemic control despite metformin therapy.
Patients with inadequate glycemic control and an HbA1c between 7% and 10% after a 2-week run-in period were randomized to glimepiride or empagliflozin 25 mg.
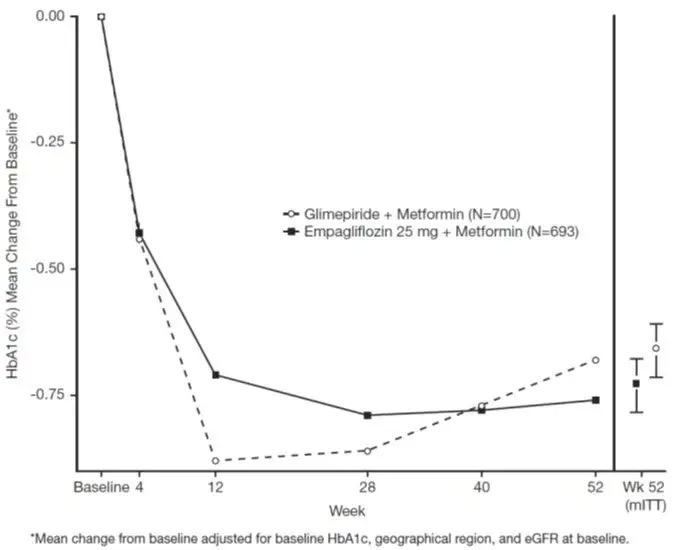
At Week 52, empagliflozin 25 mg and glimepiride lowered HbA1c and FPG (see Table 10, Figure 3). The difference in observed effect size between empagliflozin 25 mg and glimepiride excluded the pre-specified non-inferiority margin of 0.3%. The mean daily dosage of glimepiride was 2.7 mg and the maximal approved dosage in the United States is 8 mg per day.
| Empagliflozin 25 mg + Metformin N=765 | Glimepiride + Metformin N=780 |
|
|---|---|---|
| aModified intent-to-treat population. Last observation on study (LOCF) was used to impute data missing at Week 52. At Week 52, data was imputed for 15.3% and 21.9% of patients randomized to empagliflozin 25 mg and glimepiride, respectively. | ||
| bNon-inferior, ANCOVA model p-value <0.0001 (HbA1c: ANCOVA model includes baseline HbA1c, treatment, renal function, and region) | ||
| cANCOVA p-value <0.0001 (Body weight and FPG: same model used as for HbA1c but additionally including baseline body weight/baseline FPG, respectively.) | ||
| dFPG (mg/dL); for empagliflozin 25 mg, n=764, for glimepiride, n=779 | ||
| HbA1c (%)a | ||
| Baseline (mean) | 7.9 | 7.9 |
| Change from baseline (adjusted mean) | -0.7 | -0.7 |
| Difference from glimepiride (adjusted mean) (97.5% CI) | -0.07b (-0.15, 0.01) | -- |
| FPG (mg/dL)d | ||
| Baseline (mean) | 150 | 150 |
| Change from baseline (adjusted mean) | -19 | -9 |
| Difference from glimepiride (adjusted mean) | -11 | -- |
| Body Weight | ||
| Baseline mean in kg | 82.5 | 83 |
| % change from baseline (adjusted mean) | -3.9 | 2.0 |
| Difference from glimepiride (adjusted mean) (95% CI) | -5.9c (-6.3, -5.5) | -- |
At Week 52, the adjusted mean change from baseline in systolic blood pressure was -3.6 mmHg, compared to 2.2 mmHg for glimepiride. The differences between treatment groups for systolic blood pressure was statistically significant (p-value <0.0001).
At Week 104, the adjusted mean change from baseline in HbA1c was -0.75% for empagliflozin 25 mg and -0.66% for glimepiride. The adjusted mean treatment difference was -0.09% with a 97.5% confidence interval of (-0.32%, 0.15%), excluding the pre-specified non-inferiority margin of 0.3%. The mean daily dosage of glimepiride was 2.7 mg and the maximal approved dosage in the United States is 8 mg per day. The Week 104 analysis included data with and without concomitant glycemic rescue medication, as well as off-treatment data. Missing data for patients not providing any information at the visit were imputed based on the observed off-treatment data. In this multiple imputation analysis, 13.9% of the data were imputed for empagliflozin 25 mg and 12.9% for glimepiride.
At Week 104, empagliflozin 25 mg daily resulted in a statistically significant difference in change from baseline for body weight compared to glimepiride (-3.1 kg for empagliflozin 25 mg vs. +1.3 kg for glimepiride; ANCOVA-LOCF, p-value <0.0001).
14.2 Empagliflozin Cardiovascular Outcome Study in Patients with Type 2 Diabetes Mellitus and Atherosclerotic Cardiovascular Disease
EMPA-REG OUTCOME was a multicenter, multinational, randomized, double-blind parallel group study that compared the risk of experiencing a major adverse cardiovascular event (MACE) between empagliflozin and placebo when these were added to and used concomitantly with standard of care treatments for diabetes and atherosclerotic cardiovascular disease. Concomitant antidiabetic medications were kept stable for the first 12 weeks of the trial. Thereafter, antidiabetic and atherosclerotic therapies could be adjusted, at the discretion of investigators, to ensure participants were treated according to the standard care for these diseases.
A total of 7,020 patients were treated (empagliflozin 10 mg = 2,345; empagliflozin 25 mg = 2,342; placebo = 2,333) and followed for a median of 3.1 years. Approximately 72% of the study population was Caucasian, 22% was Asian, and 5% was Black. The mean age was 63 years and approximately 72% were male.
All patients in the study had inadequately controlled type 2 diabetes mellitus at baseline (HbA1c greater than or equal to 7%). The mean HbA1c at baseline was 8.1% and 57% of participants had diabetes for more than 10 years. Approximately 31%, 22% and 20% reported a past history of neuropathy, retinopathy and nephropathy to investigators, respectively and the mean eGFR was 74 mL/min/1.73 m2. At baseline, patients were treated with one (~30%) or more (~70%) antidiabetic medications including metformin (74%), insulin (48%), and sulfonylurea (43%).
All patients had established atherosclerotic cardiovascular disease at baseline including one (82%) or more (18%) of the following: a documented history of coronary artery disease (76%), stroke (23%) or peripheral artery disease (21%). At baseline, the mean systolic blood pressure was 136 mmHg, the mean diastolic blood pressure was 76 mmHg, the mean LDL was 86 mg/dL, the mean HDL was 44 mg/dL, and the mean urinary albumin to creatinine ratio (UACR) was 175 mg/g. At baseline, approximately 81% of patients were treated with renin angiotensin system inhibitors, 65% with beta-blockers, 43% with diuretics, 77% with statins, and 86% with antiplatelet agents (mostly aspirin).
The primary endpoint in EMPA-REG OUTCOME was the time to first occurrence of a Major Adverse Cardiac Event (MACE). A major adverse cardiac event was defined as occurrence of either a cardiovascular death or a non-fatal myocardial infarction (MI) or a non-fatal stroke. The statistical analysis plan had pre-specified that the 10 and 25 mg dosages would be combined. A Cox proportional hazards model was used to test for non-inferiority against the pre-specified risk margin of 1.3 for the hazard ratio of MACE and superiority on MACE if non-inferiority was demonstrated. Type-1 error was controlled across multiples tests using a hierarchical testing strategy.
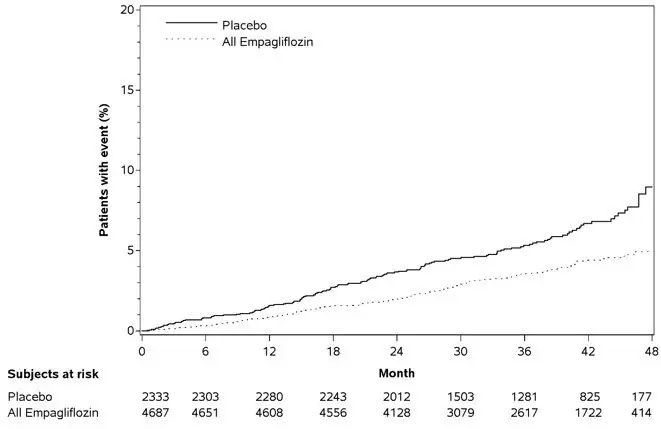
Empagliflozin significantly reduced the risk of first occurrence of primary composite endpoint of cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke (HR: 0.86; 95% CI: 0.74, 0.99). The treatment effect was due to a significant reduction in the risk of cardiovascular death in subjects randomized to empagliflozin (HR: 0.62; 95% CI: 0.49, 0.77), with no change in the risk of non-fatal myocardial infarction or non-fatal stroke (see Table 11 and Figures 4 and 5). Results for the 10 mg and 25 mg empagliflozin dosages were consistent with results for the combined dosage groups.
| Placebo N=2,333 | Empagliflozin N=4,687 | Hazard ratio vs placebo (95% CI) |
|
|---|---|---|---|
| aTreated set (patients who had received at least one dose of study drug) | |||
| bp-value for superiority (2-sided) 0.04 | |||
| cTotal number of events | |||
| Composite of cardiovascular death, non-fatal myocardial infarction, non-fatal stroke (time to first occurrence)b | 282 (12.1%) | 490 (10.5%) | 0.86 (0.74, 0.99) |
| Non-fatal myocardial infarctionc | 121 (5.2%) | 213 (4.5%) | 0.87 (0.70, 1.09) |
| Non-fatal strokec | 60 (2.6%) | 150 (3.2%) | 1.24 (0.92, 1.67) |
| Cardiovascular deathc | 137 (5.9%) | 172 (3.7%) | 0.62 (0.49, 0.77) |
Figure 4 Estimated Cumulative Incidence of First MACE
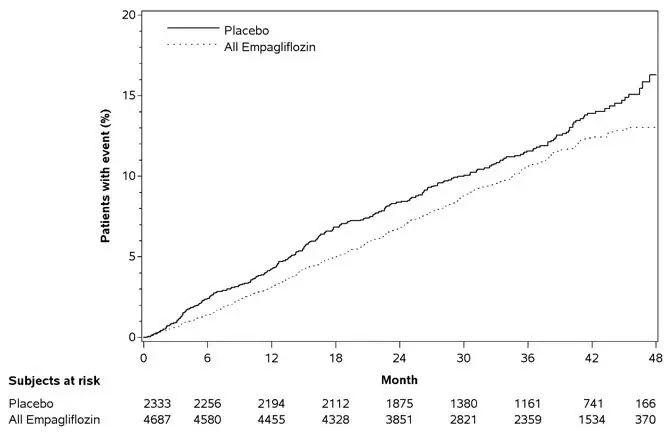
Figure 5 Estimated Cumulative Incidence of Cardiovascular Death
The efficacy of empagliflozin on cardiovascular death was generally consistent across major demographic and disease subgroups.
Vital status was obtained for 99.2% of subjects in the trial. A total of 463 deaths were recorded during the EMPA-REG OUTCOME trial. Most of these deaths were categorized as cardiovascular deaths. The non-cardiovascular deaths were only a small proportion of deaths and were balanced between the treatment groups (2.1% in patients treated with empagliflozin, and 2.4% of patients treated with placebo).
14.3 Empagliflozin Heart Failure Studies, Including Patients with Type 2 Diabetes Mellitus
16. How is Synjardy XR supplied
SYNJARDY XR tablets are available as follows:
| Tablet Strength | Color/Shape | Tablet Markings | Package Size | NDC Number |
|---|---|---|---|---|
| 5 mg Empagliflozin 1,000 mg Metformin HCl | olive green, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S5" on the top line and "1000 M" on the bottom line. | Bottles of 60 Bottles of 180 | 0597-0290-74 0597-0290-59 |
| 10 mg Empagliflozin 1,000 mg Metformin HCl | orange, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S10" on the top line and "1000 M" on the bottom line. | Bottles of 30 Bottles of 90 | 0597-0280-73 0597-0280-90 |
| 12.5 mg Empagliflozin 1,000 mg Metformin HCl | blue, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S12" on the top line and "1000 M" on the bottom line. | Bottles of 60 Bottles of 180 | 0597-0300-45 0597-0300-93 |
| 25 mg Empagliflozin 1,000 mg Metformin HCl | light green, oval, biconvex, film-coated tablet | Printed on one side in black ink with the Boehringer Ingelheim company logo and "S25" on the top line and "1000 M" on the bottom line. | Bottles of 30 Bottles of 90 | 0597-0295-88 0597-0295-78 |
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
| MEDICATION GUIDE SYNJARDY® XR (sin-JAR-dee XR) (empagliflozin and metformin hydrochloride extended-release tablets) for oral use |
|||||
|---|---|---|---|---|---|
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: February 2023 | ||||
| What is the most important information I should know about SYNJARDY XR?
SYNJARDY XR can cause serious side effects, including:
|
|||||
|
|
||||
You have a higher chance of getting lactic acidosis with SYNJARDY XR if you:
|
|||||
|
|||||
|
|
||||
| If you get any of these symptoms during treatment with SYNJARDY XR, if possible, check for ketones in your urine, even if your blood sugar is less than 250 mg/dL. | |||||
|
|||||
|
|
||||
| Talk to your healthcare provider about what you can do to prevent dehydration including how much fluid you should drink on a daily basis. Talk to your healthcare provider right away if you reduce the amount of food or liquid you drink, for example if you are sick or cannot eat or start to lose liquids from your body, for example from vomiting, diarrhea or being in the sun too long. |
|||||
| What is SYNJARDY XR?
SYNJARDY XR is a prescription medicine that contains 2 diabetes medicines, empagliflozin (JARDIANCE) and metformin hydrochloride. SYNJARDY XR can be used along with diet and exercise to improve blood sugar in adults with type 2 diabetes. One of the medicines in SYNJARDY XR, empagliflozin (JARDIANCE), can also be used in adults with type 2 diabetes: |
|||||
|
|||||
|
|||||
| Who should not take SYNJARDY XR? Do not take SYNJARDY XR if you:
|
|||||
| What should I tell my healthcare provider before taking SYNJARDY XR? Before taking SYNJARDY XR, tell your healthcare provider about all of your medical conditions, including if you:
SYNJARDY XR may affect the way other medicines work, and other medicines may affect how SYNJARDY XR works. Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine. |
|||||
How should I take SYNJARDY XR?
|
|||||
| What should I avoid while taking SYNJARDY XR?
Avoid drinking alcohol very often, or drinking a lot of alcohol in a short period of time ("binge" drinking). It can increase your chances of getting serious side effects. |
|||||
| What are the possible side effects of SYNJARDY XR? SYNJARDY XR may cause serious side effects, including:
|
|||||
|
|
|
|
||
|
|||||
|
|
|
|||
|
|||||
|
|
||||
| These are not all the possible side effects of SYNJARDY XR. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|||||
How should I store SYNJARDY XR?
|
|||||
| General information about the safe and effective use of SYNJARDY XR.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use SYNJARDY XR for a condition for which it was not prescribed. Do not give SYNJARDY XR to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about SYNJARDY XR that is written for health professionals. |
|||||
| What are the ingredients in SYNJARDY XR? Active Ingredients: empagliflozin and metformin hydrochloride Inactive Ingredients: Tablet core contains: polyethylene oxide, hypromellose, and magnesium stearate. The Film Coatings and Printing Ink contain: hypromellose, titanium dioxide, polydextrose, polyethylene glycol, talc, carnauba wax, purified water, ferrosoferric oxide, propylene glycol, isopropyl alcohol, ferric oxide yellow (5 mg/1,000 mg, 10 mg/1,000 mg, 25 mg/1,000 mg), ferric oxide red (10 mg/1,000 mg), FD&C blue#2/indigo carmine aluminum lake (12.5 mg/1,000 mg, 25 mg/1,000 mg). |
|||||
| Distributed by: Boehringer Ingelheim Pharmaceuticals, Inc.; Ridgefield, CT 06877 USA Marketed by: Boehringer Ingelheim Pharmaceuticals, Inc.; Ridgefield, CT 06877 USA and Eli Lilly and Company, Indianapolis, IN 46285 USA Licensed from: Boehringer Ingelheim International GmbH, Ingelheim, Germany SYNJARDY is a registered trademark of and used under license from Boehringer Ingelheim International GmbH. Boehringer Ingelheim Pharmaceuticals, Inc. either owns or uses the Jardiance®, EMPA-REG OUTCOME®, EMPEROR-Reduced® and EMPEROR-Preserved® trademarks under license. The other brands listed are trademarks of their respective owners and are not trademarks of Boehringer Ingelheim Pharmaceuticals, Inc. Copyright © 2023 Boehringer Ingelheim International GmbH ALL RIGHTS RESERVED COL8977HB072023 For more information about SYNJARDY XR including current prescribing information and Medication Guide, go to www.synjardyxr.com, or scan the code, or call Boehringer Ingelheim Pharmaceuticals, Inc. at 1-800-542-6257.
|
|||||


| SYNJARDY
XR
empagliflozin, metformin hydrochloride tablet, extended release |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| SYNJARDY
XR
empagliflozin, metformin hydrochloride tablet, extended release |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| SYNJARDY
XR
empagliflozin, metformin hydrochloride tablet, extended release |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| SYNJARDY
XR
empagliflozin, metformin hydrochloride tablet, extended release |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| Labeler - Boehringer Ingelheim Pharmaceuticals, Inc. (603175944) |
| Registrant - Boehringer Ingelheim Pharmaceuticals, Inc. (603175944) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Patheon Pharmaceuticals Inc. | 005286822 | ANALYSIS(0597-0280, 0597-0290, 0597-0295, 0597-0300) , LABEL(0597-0280, 0597-0290, 0597-0295, 0597-0300) , MANUFACTURE(0597-0280, 0597-0290, 0597-0295, 0597-0300) , PACK(0597-0280, 0597-0290, 0597-0295, 0597-0300) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Sixarp, LLC | 016329513 | PACK(0597-0280, 0597-0290, 0597-0295, 0597-0300) | |
