Drug Detail:Thyrogen (Thyrotropin alfa [ thye-roe-troe-pin-al-fa ])
Drug Class: In vivo diagnostic biologicals Thyroid drugs
Highlights of Prescribing Information
THYROGEN® (thyrotropin alfa) for injection, for intramuscular use
Initial U.S. Approval: 1998
Indications and Usage for Thyrogen
THYROGEN® is a thyroid stimulating hormone indicated for:
-
Adjunctive Diagnostic Tool for Well-Differentiated Thyroid Cancer:
Use as an adjunctive diagnostic tool for serum thyroglobulin (Tg) testing with or without radioiodine imaging in the follow-up of patients with well-differentiated thyroid cancer who have previously undergone thyroidectomy. (1.1)
Limitations of Use:- THYROGEN-stimulated Tg levels are generally lower than, and do not correlate with Tg levels after thyroid hormone withdrawal.
- Even when THYROGEN-Tg testing is performed in combination with radioiodine imaging, there remains a risk of missing a diagnosis of thyroid cancer or underestimating the extent of the disease.
- Anti-Tg Antibodies may confound the Tg assay and render Tg levels uninterpretable.
-
Adjunct for Thyroid Remnant Ablation in Well-Differentiated Thyroid Cancer: Use as an adjunctive treatment for radioiodine ablation of thyroid tissue remnants in patients who have undergone a near-total or total thyroidectomy for well-differentiated thyroid cancer and who do not have evidence of distant metastatic thyroid cancer. (1.2)
Limitations of Use:- The effect of THYROGEN on thyroid cancer recurrence greater than 5 years post-remnant ablation has not been evaluated.
Thyrogen Dosage and Administration
- THYROGEN should be used by physicians knowledgeable in the management of patients with thyroid cancer. (2.1)
- A two-injection regimen is recommended: THYROGEN 0.9 mg is administered intramuscularly, followed by a second 0.9 mg intramuscular injection 24 hours later. (2.1)
Dosage Forms and Strengths
For injection: 0.9 mg of thyrotropin alfa as a lyophilized powder in a single-dose vial. (3)
Contraindications
- If THYROGEN is administered with radioiodine, the contraindications to radioiodine also apply to this combination regimen. (4)
Warnings and Precautions
- THYROGEN-induced hyperthyroidism: Hospitalization for administration of THYROGEN and postadministrative observation should be considered for patients at risk. (5.1)
- Stroke: Stroke in female patients as well as other neurologic events in patients with central nervous system metastases. (5.2, 5.3)
- Sudden rapid tumor enlargement: Sudden, rapid and painful enlargement in distant metastatic thyroid cancer. (5.3)
- Risks associated with radioiodine (RAI) combination treatment: If THYROGEN is administered with RAI, the warnings and precautions for RAI also apply to this combination regimen. (5.4)
Adverse Reactions/Side Effects
The most common adverse reactions (>5%) reported in clinical trials were nausea and headache. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Genzyme Corporation at 800-745-4447 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Use In Specific Populations
- Pregnancy: Concomitant use of THYROGEN and radioiodine (RAI) is contraindicated in pregnancy. (4, 8.1)
- Lactation: Concomitant use of THYROGEN and therapeutic RAI is contraindicated in lactating women. (4, 8.2)
- Renal Impairment: Elimination of THYROGEN is significantly slower in dialysis-dependent end-stage renal disease patients, resulting in prolonged elevation of TSH levels. (8.6)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 2/2023
Full Prescribing Information
1. Indications and Usage for Thyrogen
1.1 Adjunctive Diagnostic Tool for Well-Differentiated Thyroid Cancer
THYROGEN® is indicated for use as an adjunctive diagnostic tool for serum thyroglobulin (Tg) testing with or without radioiodine imaging in the follow-up of patients with well-differentiated thyroid cancer who have previously undergone thyroidectomy.
1.2 Adjunct for Thyroid Remnant Ablation in Well-Differentiated Thyroid Cancer
THYROGEN is indicated for use as an adjunctive treatment for radioiodine ablation of thyroid tissue remnants in patients who have undergone a near-total or total thyroidectomy for well-differentiated thyroid cancer and who do not have evidence of distant metastatic thyroid cancer.
2. Thyrogen Dosage and Administration
2.1 Recommended Dosage
THYROGEN should be used by physicians knowledgeable in the management of patients with thyroid cancer.
THYROGEN is indicated as a two-injection regimen. The recommended dosage of THYROGEN is a 0.9 mg intramuscular injection to the buttock followed by a second 0.9 mg intramuscular injection to the buttock 24 hours later.
THYROGEN should be administered intramuscularly only. THYROGEN should not be administered intravenously.
Pretreatment with glucocorticoids should be considered for patients in whom tumor expansion may compromise vital anatomic structures [see Warnings and Precautions (5.3)].
Routine measurement of serum TSH levels is not recommended after THYROGEN use.
2.2 Reconstitution, Preparation, and Administration of THYROGEN
The supplied lyophilized powder must be reconstituted with Sterile Water for Injection, USP. THYROGEN should be prepared, and administered in the following manner:
- Reconstitute each 0.9 mg vial of THYROGEN with 1.2 mL of Sterile Water for Injection, USP to yield a single-dose solution containing 0.9 mg/mL of thyrotropin alfa that delivers 1 mL (0.9 mg).
- Gently swirl the contents of the vial until all the material is dissolved. Do not shake the solution.
- Visually inspect the reconstituted solution for particulate matter and discoloration prior to administration. The reconstituted THYROGEN solution should be clear and colorless. Do not use if the solution has particulate matter or is cloudy or discolored.
- Withdraw 1 mL of the reconstituted THYROGEN solution (0.9 mg of thyrotropin alfa) and inject intramuscularly in the buttocks. Discard any unused portions.
- The reconstituted THYROGEN solution must be injected within 3 hours unless refrigerated.
- If necessary, the reconstituted solution can be stored refrigerated at a temperature between 2°C and 8°C (36°F to 46°F) for up to 24 hours, while avoiding microbial contamination.
- Do not mix with other substances.
2.3 Timing of Serum Thyroglobulin Testing Following THYROGEN Administration
For serum thyroglobulin testing, the serum sample should be obtained 72 hours after the final injection of THYROGEN [see Clinical Studies (14.1)].
2.4 Timing for Remnant Ablation and Diagnostic Scanning Following THYROGEN Administration
Oral radioiodine should be given 24 hours after the second injection of THYROGEN in both remnant ablation and diagnostic scanning. The activity of 131I is carefully selected at the discretion of the nuclear medicine physician.
Diagnostic scanning should be performed 48 hours after the radioiodine administration.
3. Dosage Forms and Strengths
For injection: 0.9 mg white to off-white lyophilized powder in a single-dose vial
4. Contraindications
If THYROGEN is administered with radioiodine, the contraindications to radioiodine also apply to this combination regimen. Refer to the radioiodine prescribing information for a list of contraindications for radioiodine.
5. Warnings and Precautions
5.1 THYROGEN-Induced Hyperthyroidism
When given to patients who have substantial thyroid tissue still in situ or functional thyroid cancer metastases, THYROGEN is known to cause a transient (over 7 to 14 days) but significant rise in serum thyroid hormone concentration. There have been reports of death in non-thyroidectomized patients and in patients with distant metastatic thyroid cancer in which events leading to death occurred within 24 hours after administration of THYROGEN. Patients with residual thyroid tissue at risk for THYROGEN-induced hyperthyroidism include the elderly and those with a known history of heart disease. Hospitalization for administration of THYROGEN and postadministration observation in patients at risk should be considered.
5.2 Stroke
There are postmarketing reports of radiologically-confirmed stroke and neurological findings suggestive of stroke unconfirmed radiologically (e.g., unilateral weakness) occurring within 72 hours (range 20 minutes to three days) of THYROGEN administration in patients without known central nervous system metastases. The majority of such patients were young women taking oral contraceptives at the time of their event or had other risk factors for stroke, such as smoking or a history of migraine headaches. The relationship between THYROGEN administration and stroke is unknown. Patients should be well-hydrated prior to treatment with THYROGEN.
5.3 Sudden Rapid Tumor Enlargement
Sudden, rapid and painful enlargement of residual thyroid tissue or distant metastases can occur following treatment with THYROGEN. This may lead to acute symptoms, which depend on the anatomical location of the tissue. Such symptoms include acute hemiplegia, hemiparesis, and loss of vision one to three days after THYROGEN administration. Laryngeal edema, pain at the site of distant metastasis, and respiratory distress requiring tracheotomy have also been reported after THYROGEN administration.
Pretreatment with glucocorticoids should be considered for patients in whom tumor expansion may compromise vital anatomic structures.
6. Adverse Reactions/Side Effects
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data described below reflect exposure to THYROGEN in 481 thyroid cancer patients who participated in a total of 6 clinical trials of THYROGEN: 4 trials for diagnostic use and 2 trials for ablation. In clinical trials, patients had undergone near-total thyroidectomy and had a mean age of 46.1 years. Thyroid cancer diagnosis was as follows: papillary (69.2%), follicular (12.9%), Hurthle cell (2.3%) and papillary/follicular (15.6%). Most patients received 2 intramuscular injections of 0.9 mg of THYROGEN injection gin 24 hours apart [see Clinical Studies (14.1, 14.2)].
The safety profile of patients who have undergone thyroidectomy and received THYROGEN as adjunctive treatment for radioiodine ablation of thyroid tissue remnants for well-differentiated thyroid cancer did not differ from that of patients who received THYROGEN for diagnostic purposes.
Reactions reported in ≥1% of patients in the combined trials are summarized in Table 1. In some studies, an individual patient may have participated in both THYROGEN and thyroid hormone withdrawal [see Clinical Studies (14.1, 14.2)].
| THYROGEN | Thyroid Hormone Withdrawal | |
|---|---|---|
| (N=481) | (N=418) | |
| Preferred Term | n (%) | n (%) |
| Nausea | 53 (11) | 2 (<1) |
| Headache | 29 (6) | 0 |
| Fatigue | 11 (2) | 2 (<1) |
| Vomiting | 11 (2) | 0 |
| Dizziness | 9 (2) | 0 (0.0) |
| Asthenia | 5 (1) | 1 (<1) |
8. Use In Specific Populations
8.3 Females and Males of Reproductive Potential
THYROGEN may be used in combination with radioiodine (RAI). If THYROGEN is administered with RAI, the information for RAI regarding pregnancy testing, contraception, and infertility also applies to the combination regimen. Refer to the RAI prescribing information for additional information.
8.5 Geriatric Use
In pooled clinical studies of THYROGEN, 60 patients (12%) were >65 years, and 421 (88%) were ≤65 years of age. Results from controlled trials do not indicate a difference in the safety and efficacy of THYROGEN between adult patients less than 65 years and those over 65 years of age [see Warnings and Precautions (5.1)].
10. Overdosage
In clinical trials of THYROGEN, three patients experienced symptoms after receiving THYROGEN doses higher than those recommended. Two patients had nausea after a 2.7 mg IM dose (3 times the recommended dose), and in one of these patients, the event was accompanied by weakness, dizziness and headache. Another patient experienced nausea, vomiting and hot flashes after a 3.6 mg IM dose (4 times the recommended dose). There is no specific therapy for THYROGEN overdose. Supportive care is recommended.
11. Thyrogen Description
Thyrotropin alfa, a recombinant human thyroid stimulating hormone, is a heterodimeric glycoprotein comprised of two non-covalently linked subunits, an alpha subunit of 92 amino acid residues containing two N-linked glycosylation sites and a beta subunit of 118 residues containing one N-linked glycosylation site. The amino acid sequence of thyrotropin alfa is identical to that of human pituitary TSH. Thyrotropin alfa is synthesized in a genetically modified Chinese hamster ovary cell line.
Both thyrotropin alfa and naturally occurring human pituitary TSH are synthesized as a mixture of glycosylation variants. Unlike pituitary TSH, which is secreted as a mixture of sialylated and sulfated forms, thyrotropin alfa is sialylated but not sulfated. The biological activity of thyrotropin alfa is determined by a cell-based bioassay. In this assay, cells expressing a functional TSH receptor and a cAMP-responsive element coupled to a heterologous reporter gene, luciferase, enable the measurement of thyrotropin alfa activity by measuring the luciferase response. The specific activity of thyrotropin alfa is determined relative to an internal Genzyme reference standard that was calibrated against the World Health Organization (WHO) human TSH reference standard.
THYROGEN (thyrotropin alfa) for injection is a sterile, white to off-white lyophilized powder in a single-dose vial for intramuscular use after reconstitution.
Each single-dose vial provides 0.9 mg of thyrotropin alfa, and contains mannitol (36 mg); sodium chloride (2.4 mg);sodium phosphate dibasic, heptahydrate (3.7 mg); and sodium phosphate monobasic, monohydrate (1.4 mg). After reconstitution with 1.2 mL of Sterile Water for Injection, USP, the concentration is 0.9 mg/mL with a deliverable volume of 1 mL (0.9 mg) and a pH of approximately 6.5 to 7.5.
12. Thyrogen - Clinical Pharmacology
12.1 Mechanism of Action
Thyrotropin (TSH) is a pituitary hormone that stimulates the thyroid gland to produce thyroid hormone. Binding of thyrotropin alfa to TSH receptors on normal thyroid epithelial cells or on well-differentiated thyroid cancer tissue stimulates iodine uptake and organification, and synthesis and secretion of thyroglobulin (Tg), triiodothyronine (T3) and thyroxine (T4).
The effect of thyroid stimulating hormone activation of thyroid cells is to increase uptake of radioiodine to allow scan detection or radioiodine killing of thyroid cells. TSH activation also leads to the release of thyroglobulin by thyroid cells. Thyroglobulin functions as a tumor marker which is detected in blood specimens.
12.3 Pharmacokinetics
The pharmacokinetics of THYROGEN was studied in 16 patients with well-differentiated thyroid cancer given a single 0.9 mg IM dose. Mean peak serum TSH concentrations of 116±38 mU/L were reached between 3 and 24 hours after injection (median of 10 hours). The mean apparent elimination half-life was 25±10 hours. The organ(s) of TSH clearance in man have not been identified, but studies of pituitary-derived TSH suggest the involvement of the liver and kidneys.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term toxicity studies in animals have not been performed with THYROGEN to evaluate the carcinogenic potential of the drug. THYROGEN was not mutagenic in the bacterial reverse mutation assay. Studies have not been performed with THYROGEN to evaluate the effects on fertility.
14. Clinical Studies
14.1 Clinical Trials of THYROGEN as an Adjunctive Diagnostic Tool for Well-Differentiated Thyroid Cancer
Two prospective, randomized phase 3 clinical trials were conducted in patients with well-differentiated thyroid cancer to compare 131I whole body scans obtained after THYROGEN injection to 131I whole body scans after thyroid hormone withdrawal. A cross-over, non-blinded design was used in both trials. Oral radioiodine was given 24 hours after the second injection of THYROGEN, and scanning was done 48 hours after the radioiodine administration. Each patient was scanned first following THYROGEN and then scanned after thyroid hormone withdrawal. In both studies, the primary endpoint was the rate of concordant scans (scan findings in agreement in a given patient using each preparation method).
Study 1 (n=127) compared the diagnostic scanning following a THYROGEN regimen of 0.9 mg IM daily on two consecutive days to thyroid hormone withdrawal. In addition to body scans, Study 2 (n=229) also compared thyroglobulin (Tg) levels obtained after THYROGEN to those at baseline and to those after thyroid hormone withdrawal. All Tg testing was performed in a central laboratory using a radioimmunoassay (RIA) with a functional sensitivity of 2.5 ng/mL. Patients who were included in the Tg analysis were those who had undergone total or near-total thyroidectomy with or without 131I ablation, had <1% uptake in the thyroid bed on a scan after thyroid hormone withdrawal, and did not have detectable anti-Tg antibodies. The maximum THYROGEN Tg value was obtained 72 hours after the final THYROGEN injection, and this value was used in the analysis.
14.2 Clinical Trials of THYROGEN as an Adjunct for Thyroid Remnant Ablation in Well-Differentiated Thyroid Cancer
A randomized, prospective clinical trial compared the rates of thyroid remnant ablation achieved after preparation of patients with thyroid hormone withdrawal or THYROGEN. Patients (n=63) with low-risk, well-differentiated thyroid cancer who underwent near-total thyroidectomy were made euthyroid after surgery by receiving thyroid hormone replacement and were subsequently randomized to a thyroid hormone withdrawal or THYROGEN. Patients in the THYROGEN group received THYROGEN 0.9 mg IM daily on 2 consecutive days and radioiodine 24 hours after the second dose of THYROGEN. Patients in the thyroid hormone withdrawal group had the thyroid replacement withheld until they became hypothyroid. Patients in both groups received 100 mCi 131I ± 10% with the intent to ablate any thyroid remnant tissue. The primary endpoint of the study was the rate of successful ablation, and was assessed 8 months later by a THYROGEN-stimulated radioiodine scan. Patients were considered successfully ablated if there was no visible thyroid bed uptake on the scan, or if visible, uptake was less than 0.1%. Table 3 summarizes the results of this evaluation.
| Group* | Mean Age (Yr) | Gender (F:M) | Cancer Type (Pap:Fol) | Ablation Criterion (Measure at 8 Months) |
|
|---|---|---|---|---|---|
| Thyroid Bed Activity <0.1% | No Visible Thyroid Bed Activity† | ||||
| Abbreviations: fol = follicular, pap = papillary | |||||
|
|||||
| Thyroid Hormone Withdrawal (N=28) | 43 | 24:6 | 29:1 | 28/28 (100%) | 24/28 (86%) |
| THYROGEN (N=32) | 44 | 26:7 | 30:3 | 32/32 (100%) | 24/32 (75%) |
The mean radiation dose to blood was 0.266 ± 0.061 mGy/MBq in the THYROGEN group and 0.395 ± 0.135 mGy/MBq in the thyroid hormone withdrawal group. Radioiodine residence time in remnant tissue was 0.9 ± 1.3 hours in the THYROGEN group and 1.4 ± 1.5 hours in the thyroid hormone withdrawal group. It is not known whether this difference in radiation exposure would convey a clinical benefit.
Patients who completed were followed up for a median duration of 3.7 years (range 3.4 to 4.4 years) following radioiodine ablation. Tg testing was also performed. The main objective of the follow-up study was to evaluate the status of thyroid remnant ablation by using THYROGEN-stimulated neck imaging. Of the fifty-one patients enrolled, forty-eight patients received THYROGEN for remnant neck/whole body imaging and/or thyroglobulin testing. Only 43 patients had imaging. Patients were still considered to be successfully ablated if there was no visible thyroid bed uptake on the scan, or if visible, uptake was less than 0.1%. All patients from both original treatment groups who had scanning were found to still be ablated. Of 37 patients who were Tg-antibody negative, 16/17 (94%) of patients in the former thyroid hormone withdrawal group and 19/20 (95%) of patients in the former THYROGEN group maintained successful ablation measured as stimulated serum Tg levels of <2 ng/mL.
No patient had a definitive cancer recurrence during the 3.7 years of follow-up. Overall, 48/51 patients (94%) had no evidence of cancer recurrence, 1 patient had possible cancer recurrence (although it was not clear whether this patient had a true recurrence or persistent tumor from the regional disease noted at the start of the initial study), and 2 patients could not be assessed.
Two large prospective multicenter randomized studies compared THYROGEN to thyroid hormone withdrawal using two different doses of radioactive iodine in patients with differentiated thyroid cancer who had been thyroidectomized. In both studies, patients were randomized to 1 of 4 treatment groups: THYROGEN + 30 mCi 131I, THYROGEN + 100 mCi 131I, thyroid hormone withdrawal + 30 mCi 131I, or thyroid hormone withdrawal + 100 mCi 131I. Patients were assessed for efficacy (ablation success rates) at approximately 8 months.
The first study (Study A) randomized 438 patients (tumor stages T1–T3, Nx, N0 and N1, M0). Ablation success was defined as radioiodine uptake of <0.1% in the thyroid bed and stimulated thyroglobulin levels of <2.0 ng/mL. Results are summarized below (Table 4).
| THYROGEN | Thyroid Hormone Withdrawal | Total | |
|---|---|---|---|
| 95% CI of difference in ablation rate (low dose minus high dose): -10.2% to 2.6% 95% CI of difference in ablation rate (THYROGEN - Thyroid Hormone Withdrawal): -6.0% to 6.8% |
|||
| Low-dose radioiodine | 91/108 (84.3%) | 91/106 (85.8%) | 182/214 (85.0%) |
| High-dose Radioiodine | 92/102 (90.2%) | 92/105 (87.6%) | 184/207 (88.9%) |
| Total | 183/210 (87.1%) | 183/211 (86.7%) | 366/421 (86.9%) |
For Study A, 434 (99%) of the original 438 patients were followed up for disease recurrence. The median follow-up was 6.5 years (0.03 to 10.6 years).
The second study (Study B) randomized 752 patients with low-risk thyroid cancer (tumor stages pT1 <1 cm and N1 or Nx, pT1 >1–2 cm and any N stage, or pT2 N0, all patients M0). Ablation success was defined by neck ultrasound and stimulated thyroglobulin of ≤1.0 ng/mL. Results are summarized below (Table 5).
| THYROGEN | Thyroid Hormone Withdrawal | Total | |
|---|---|---|---|
| 95% CI of difference in ablation rate (low dose minus high dose): -5.8% to 0.9% 95% CI of difference in ablation rate (THYROGEN minus Thyroid Hormone Withdrawal): -4.5% to 2.2% |
|||
| Low-dose radioiodine | 160/177 (90.4%) | 156/170 (91.8%) | 316/347 (91.1%) |
| High-dose Radioiodine | 159/171 (93.0%) | 156/166 (94.0%) | 315/337 (93.5%) |
| Total | 319/348 (91.6%) | 312/336 (92.9%) | 631/684 (92.3%) |
For Study B, 726 (97%) of the original 752 patients were followed up for disease recurrence. The median follow-up was 5.4 years (0.5 to 9.2 years).
Five-year follow-up data of THYROGEN for remnant ablation with two different RAI doses in Study A and Study B observed similar rates of thyroid cancer recurrence as thyroid hormone withdrawal.
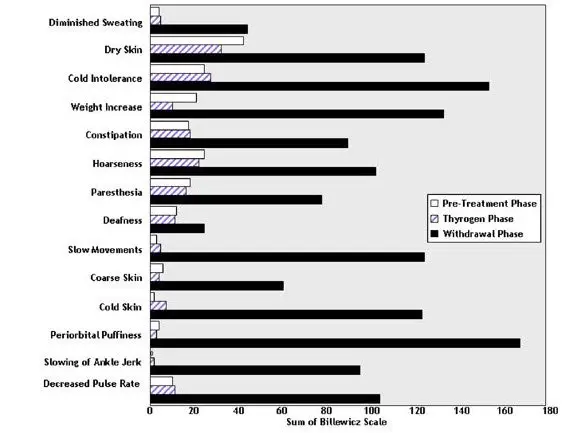
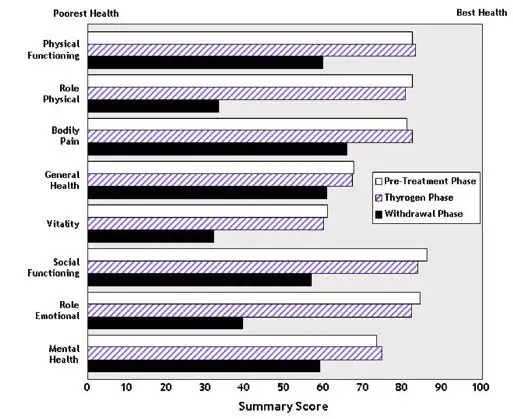
14.3 Quality of Life
Quality of Life (QOL) was measured during both the diagnostic study [see Clinical Studies (14.1)] and the ablation of thyroid remnant study [see Clinical Studies (14.2)] using the SF-36 Health Survey, a standardized, patient-administered instrument assessing QOL across eight domains measuring both physical and mental functioning. In the diagnostic study and in the remnant ablation study, following THYROGEN administration, little change from baseline was observed in any of the eight QOL domains of the SF-36. Following thyroid hormone withdrawal in the diagnostic study, statistically significant negative changes were noted in all eight QOL domains of the SF-36. The difference between treatment groups was statistically significant (p<0.0001) for all eight QOL domains, favoring THYROGEN over thyroid hormone withdrawal (Figure 2). In the remnant ablation study, following thyroid hormone withdrawal, statistically significant negative changes were noted in five of the eight QOL domains (physical functioning, role physical, vitality, social functioning and mental health).
Figure 2: SF-36 Health Survey Results Quality of Life Domains Diagnostic Indication
16. How is Thyrogen supplied
THYROGEN (thyrotropin alfa) for injection is as a sterile white to off-white lyophilized powder in a single-dose vial. Each carton (NDC 58468-0030-2) contains two 0.9 mg single-dose vials of THYROGEN (NDC 58468-0030-1).

| THYROGEN
thyrotropin alfa injection, powder, lyophilized, for solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| THYROGEN
thyrotropin alfa kit |
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
|
|||||||||||||||
| Labeler - Genzyme Corporation (025322157) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Corporation | 968278874 | MANUFACTURE(58468-0030, 58468-1849) , API MANUFACTURE(58468-0030, 58468-1849) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Ireland Limited | 985127419 | MANUFACTURE(58468-0030, 58468-1849) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Corporation | 050424395 | LABEL(58468-0030, 58468-1849) , PACK(58468-0030, 58468-1849) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Corporation | 968278916 | ANALYSIS(58468-0030, 58468-1849) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genzyme Corporation | 968302658 | ANALYSIS(58468-0030, 58468-1849) | |
