Drug Detail:Trinessa (Ethinyl estradiol and norgestimate [ eth-i-nil-es-tra-dye-ol-and-nor-jes-ti-mate ])
Drug Class: Contraceptives
WARNINGS: CARDIOVASCULAR RISK ASSOCIATED WITH SMOKING
Cigarette smoking increases the risk of serious cardiovascular events from combination oral contraceptive use. This risk increases with age, particularly in women over 35 years of age, and with the number of cigarettes smoked. For this reason, combination oral contraceptives, including TriNessa®, should not be used by women who are over 35 years of age and smoke.
Indications and Usage for TriNessa
TriNessa® is indicated for the prevention of pregnancy in women who elect to use oral contraceptives as a method of contraception.
TriNessa® is indicated for the treatment of moderate acne vulgaris in females at least 15 years of age, who have no known contraindications to oral contraceptive therapy and have achieved menarche. TriNessa® should be used for the treatment of acne only if the patient desires an oral contraceptive for birth control.
Oral contraceptives are highly effective for pregnancy prevention. Table 2 lists the typical accidental pregnancy rates for users of combination oral contraceptives and other methods of contraception. The efficacy of these contraceptive methods, except sterilization, the IUD, and the Norplant® System, depends upon the reliability with which they are used. Correct and consistent use of methods can result in lower failure rates.
| % of Women Experiencing an Unintended Pregnancy within the First Year of Use | % of Women Continuing Use at One Year* | ||
|---|---|---|---|
| Method | Typical Use† | Perfect Use‡ | |
| (1) | (2) | (3) | (4) |
| Hatcher et al, 1998, Ref. #1. | |||
| Emergency Contraceptive Pills: Treatment initiated within 72 hours after unprotected intercourse reduces the risk of pregnancy by at least 75%.§ | |||
| Lactational Amenorrhea Method: LAM is a highly effective, temporary method of contraception.¶ | |||
| Source: Trussell J, Contraceptive efficacy. In Hatcher RA, Trussell J, Stewart F, Cates W, Stewart GK, Kowal D, Guest F, Contraceptive Technology: Seventeenth Revised Edition. New York NY: Irvington Publishers, 1998. | |||
|
|||
| Chance# | 85 | 85 | |
| SpermicidesÞ | 26 | 6 | 40 |
| Periodic abstinence | 25 | 63 | |
| Calendar | 9 | ||
| Ovulation Method | 3 | ||
| Sympto-Thermalß | 2 | ||
| Post-Ovulation | 1 | ||
| Capà | |||
| Parous Women | 40 | 26 | 42 |
| Nulliparous Women | 20 | 9 | 56 |
| Sponge | |||
| Parous Women | 40 | 20 | 42 |
| Nulliparous Women | 20 | 9 | 56 |
| Diaphragmà | 20 | 6 | 56 |
| Withdrawal | 19 | 4 | |
| Condomè | |||
| Female (Reality®) | 21 | 5 | 56 |
| Male | 14 | 3 | 61 |
| Pill | 5 | 71 | |
| Progestin Only | 0.5 | ||
| Combined | 0.1 | ||
| IUD | |||
| Progesterone T | 2.0 | 1.5 | 81 |
| Copper T380A | 0.8 | 0.6 | 78 |
| LNg 20 | 0.1 | 0.1 | 81 |
| Depo-Provera® | 0.3 | 0.3 | 70 |
| Norplant® and Norplant-2® | 0.05 | 0.05 | 88 |
| Female Sterilization | 0.5 | 0.5 | 100 |
| Male Sterilization | 0.15 | 0.10 | 100 |
TriNessa® has not been studied for and is not indicated for use in emergency contraception.
In four clinical trials with TriNessa®, a total of 4,756 subjects completed 45,244 cycles, and the use-efficacy pregnancy rate was approximately 1 pregnancy per 100 women-years.
TriNessa® was evaluated for the treatment of acne vulgaris in two randomized, double-blind, placebo-controlled, multicenter, Phase 3, six (28 day) cycle studies. 221 patients received TriNessa® and 234 patients received placebo. Mean age at enrollment for both groups was 28 years. At the end of 6 months, the mean total lesion count changes from 55 to 31 (42% reduction) in patients treated with TriNessa® and from 54 to 38 (27% reduction) in patients similarly treated with placebo. Table 3 summarizes the changes in lesion count for each type of lesion in the ITT population. Based on the investigator's global assessment conducted at the final visit, patients treated with TriNessa® showed a statistically significant improvement in total lesions compared to those treated with placebo.
| TriNessa®
(N=221) | Placebo (N=234) | Difference in Counts between TriNessa® and Placebo at 6 Months | |||
|---|---|---|---|---|---|
| # of Lesions | Counts | % Reduction | Counts | % Reduction | |
|
|||||
| INFLAMMATORY LESIONS | |||||
| Baseline Mean | 19 | 19 | |||
| Sixth Month Mean | 10 | 48% | 13 | 30% | 3 (95%CI: -1.2, 5.1) |
| NON-INFLAMMATORY LESIONS | |||||
| Baseline Mean | 36 | 35 | |||
| Sixth Month Mean | 22 | 34% | 25 | 21% | 3 (95% CI: -0.2, 7.8) |
| TOTAL LESIONS | |||||
| Baseline Mean | 55 | 54 | |||
| Sixth Month Mean | 31 | 42% | 38 | 27% | 7 (95% CI: 2.0, 11.9) |
Contraindications
Oral contraceptives should not be used in women who currently have the following conditions:
- Thrombophlebitis or thromboembolic disorders
- A past history of deep vein thrombophlebitis or thromboembolic disorders
- Known thrombophilic conditions
- Cerebral vascular or coronary artery disease (current or past history)
- Valvular heart disease with complications
- Persistent blood pressure values of ≥ 160 mm Hg systolic or ≥ 100 mg Hg diastolic102
- Diabetes with vascular involvement
- Headaches with focal neurological symptoms
- Major surgery with prolonged immobilization
- Known or suspected carcinoma of the breast or personal history of breast cancer
- Carcinoma of the endometrium or other known or suspected estrogen-dependent neoplasia
- Undiagnosed abnormal genital bleeding
- Cholestatic jaundice of pregnancy or jaundice with prior pill use
- Acute or chronic hepatocellular disease with abnormal liver function
- Hepatic adenomas or carcinomas
- Known or suspected pregnancy
- Hypersensitivity to any component of this product
Warnings
1. Thromboembolic Disorders and Other Vascular Problems
a. Myocardial Infarction
An increased risk of myocardial infarction has been attributed to oral contraceptive use. This risk is primarily in smokers or women with other underlying risk factors for coronary artery disease such as hypertension, hypercholesterolemia, morbid obesity, and diabetes. The relative risk of heart attack for current oral contraceptive users has been estimated to be two to six.4–10 The risk is very low under the age of 30.
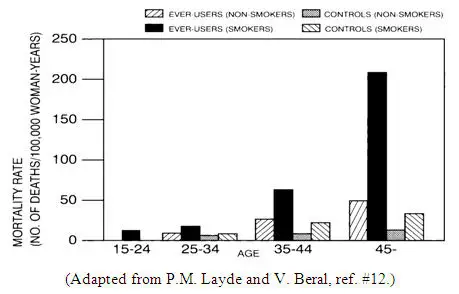
Smoking in combination with oral contraceptive use has been shown to contribute substantially to the incidence of myocardial infarctions in women in their mid-thirties or older with smoking accounting for the majority of excess cases.11 Mortality rates associated with circulatory disease have been shown to increase substantially in smokers, especially in those 35 years of age and older, and in nonsmokers over the age of 40 among women who use oral contraceptives. (See Figure 1)
Oral contraceptives may compound the effects of well-known risk factors, such as hypertension, diabetes, hyperlipidemias, age and obesity.13 In particular, some progestogens are known to decrease HDL cholesterol and cause glucose intolerance, while estrogens may create a state of hyperinsulinism.14–18 Oral contraceptives have been shown to increase blood pressure among users (see Section 9 in WARNINGS). Similar effects on risk factors have been associated with an increased risk of heart disease. Oral contraceptives must be used with caution in women with cardiovascular disease risk factors.
Norgestimate has minimal androgenic activity (see CLINICAL PHARMACOLOGY), and there is some evidence that the risk of myocardial infarction associated with oral contraceptives is lower when the progestogen has minimal androgenic activity than when the activity is greater.97
b. Thromboembolism
An increased risk of thromboembolic and thrombotic disease associated with the use of oral contraceptives is well established. Case control studies have found the relative risk of users compared to nonusers to be 3 for the first episode of superficial venous thrombosis, 4 to 11 for deep vein thrombosis or pulmonary embolism, and 1.5 to 6 for women with predisposing conditions for venous thromboembolic disease.2,3,19–24 Cohort studies have shown the relative risk to be somewhat lower, about 3 for new cases and about 4.5 for new cases requiring hospitalization.25 The risk of thromboembolic disease associated with oral contraceptives is not related to length of use and disappears after pill use is stopped.2
A two- to four-fold increase in relative risk of post-operative thromboembolic complications has been reported with the use of oral contraceptives.9 The relative risk of venous thrombosis in women who have predisposing conditions is twice that of women without such medical conditions.26 If feasible, oral contraceptives should be discontinued at least four weeks prior to and for two weeks after elective surgery of a type associated with an increase in risk of thromboembolism and during and following prolonged immobilization. Since the immediate postpartum period is also associated with an increased risk of thromboembolism, oral contraceptives should be started no earlier than four weeks after delivery in women who elect not to breastfeed.
c. Cerebrovascular Diseases
Oral contraceptives have been shown to increase both the relative and attributable risks of cerebrovascular events (thrombotic and hemorrhagic strokes), although, in general, the risk is greatest among older (>35 years), hypertensive women who also smoke. Hypertension was found to be a risk factor for both users and nonusers, for both types of strokes, and smoking interacted to increase the risk of stroke.27–29
In a large study, the relative risk of thrombotic strokes has been shown to range from 3 for normotensive users to 14 for users with severe hypertension.30 The relative risk of hemorrhagic stroke is reported to be 1.2 for non-smokers who used oral contraceptives, 2.6 for smokers who did not use oral contraceptives, 7.6 for smokers who used oral contraceptives, 1.8 for normotensive users and 25.7 for users with severe hypertension.30 The attributable risk is also greater in older women.3
d. Dose-Related Risk of Vascular Disease From Oral Contraceptives
A positive association has been observed between the amount of estrogen and progestogen in oral contraceptives and the risk of vascular disease.31–33 A decline in serum high density lipoproteins (HDL) has been reported with many progestational agents.14–16 A decline in serum high density lipoproteins has been associated with an increased incidence of ischemic heart disease. Because estrogens increase HDL cholesterol, the net effect of an oral contraceptive depends on a balance achieved between doses of estrogen and progestogen and the activity of the progestogen used in the contraceptives. The activity and amount of both hormones should be considered in the choice of an oral contraceptive.
Minimizing exposure to estrogen and progestogen is in keeping with good principles of therapeutics. For any particular estrogen/progestogen combination, the dosage regimen prescribed should be one which contains the least amount of estrogen and progestogen that is compatible with a low failure rate and the needs of the individual patient. New acceptors of oral contraceptive agents should be started on preparations containing the lowest estrogen content which is judged appropriate for the individual patient.
e. Persistence of Risk of Vascular Disease
There are two studies which have shown persistence of risk of vascular disease for ever-users of oral contraceptives. In a study in the United States, the risk of developing myocardial infarction after discontinuing oral contraceptives persists for at least 9 years for women 40–49 years who had used oral contraceptives for five or more years, but this increased risk was not demonstrated in other age groups.8 In another study in Great Britain, the risk of developing cerebrovascular disease persisted for at least 6 years after discontinuation of oral contraceptives, although excess risk was very small.34 However, both studies were performed with oral contraceptive formulations containing 50 micrograms or higher of estrogens.
2. Estimates of Mortality From Contraceptive Use
One study gathered data from a variety of sources which have estimated the mortality rate associated with different methods of contraception at different ages (Table 4). These estimates include the combined risk of death associated with contraceptive methods plus the risk attributable to pregnancy in the event of method failure. Each method of contraception has its specific benefits and risks. The study concluded that with the exception of oral contraceptive users 35 and older who smoke, and 40 and older who do not smoke, mortality associated with all methods of birth control is low and below that associated with childbirth. The observation of an increase in risk of mortality with age for oral contraceptive users is based on data gathered in the 1970's.35 Current clinical recommendation involves the use of lower estrogen dose formulations and a careful consideration of risk factors. In 1989, the Fertility and Maternal Health Drugs Advisory Committee was asked to review the use of oral contraceptives in women 40 years of age and over. The Committee concluded that although cardiovascular disease risks may be increased with oral contraceptive use after age 40 in healthy non-smoking women (even with the newer low-dose formulations), there are also greater potential health risks associated with pregnancy in older women and with the alternative surgical and medical procedures which may be necessary if such women do not have access to effective and acceptable means of contraception. The Committee recommended that the benefits of low-dose oral contraceptive use by healthy non-smoking women over 40 may outweigh the possible risks.
Of course, older women, as all women, who take oral contraceptives, should take an oral contraceptive which contains the least amount of estrogen and progestogen that is compatible with a low failure rate and individual patient needs.
| Method of control and outcome | 15–19 | 20–24 | 25–29 | 30–34 | 35–39 | 40–44 |
|---|---|---|---|---|---|---|
| Adapted from H.W. Ory, ref. #35. | ||||||
|
||||||
| No fertility control methods* | 7.0 | 7.4 | 9.1 | 14.8 | 25.7 | 28.2 |
| Oral contraceptives non-smoker† | 0.3 | 0.5 | 0.9 | 1.9 | 13.8 | 31.6 |
| Oral contraceptives, smoker† | 2.2 | 3.4 | 6.6 | 13.5 | 51.1 | 117.2 |
| IUD† | 0.8 | 0.8 | 1.0 | 1.0 | 1.4 | 1.4 |
| Condom* | 1.1 | 1.6 | 0.7 | 0.2 | 0.3 | 0.4 |
| Diaphragm/spermicide* | 1.9 | 1.2 | 1.2 | 1.3 | 2.2 | 2.8 |
| Periodic abstinence* | 2.5 | 1.6 | 1.6 | 1.7 | 2.9 | 3.6 |
9. Elevated Blood Pressure
Women with significant hypertension should not be started on hormonal contraception.98 An increase in blood pressure has been reported in women taking oral contraceptives68 and this increase is more likely in older oral contraceptive users69 and with extended duration of use.61 Data from the Royal College of General Practitioners12 and subsequent randomized trials have shown that the incidence of hypertension increases with increasing progestational activity.
Women with a history of hypertension or hypertension-related diseases, or renal disease70 should be encouraged to use another method of contraception. If these women elect to use oral contraceptives, they should be monitored closely and if a clinically significant persistent elevation of blood pressure (BP) occurs (≥ 160 mm Hg systolic or ≥ 100 mm Hg diastolic) and cannot be adequately controlled, oral contraceptives should be discontinued. In general, women who develop hypertension during hormonal contraceptive therapy should be switched to a non-hormonal contraceptive. If other contraceptive methods are not suitable, hormonal contraceptive therapy may continue combined with antihypertensive therapy. Regular monitoring of BP throughout hormonal contraceptive therapy is recommended.102 For most women, elevated blood pressure will return to normal after stopping oral contraceptives, and there is no difference in the occurrence of hypertension between former and never users.68–71
Precautions
8. Drug Interactions
Consult the labeling of concurrently-used drugs to obtain further information about interactions with hormonal contraceptives or the potential for enzyme alterations.
Effects of Other Drugs on Combined Hormonal Contraceptives
12. Nursing Mothers
Small amounts of oral contraceptive steroids have been identified in the milk of nursing mothers and a few adverse effects on the child have been reported, including jaundice and breast enlargement. In addition, combination oral contraceptives given in the postpartum period may interfere with lactation by decreasing the quantity and quality of breast milk. If possible, the nursing mother should be advised not to use combination oral contraceptives but to use other forms of contraception until she has completely weaned her child.
TriNessa Dosage and Administration
Oral Contraception
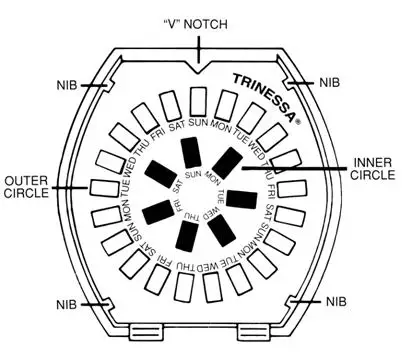
To achieve maximum contraceptive effectiveness, TriNessa® must be taken exactly as directed and at intervals not exceeding 24 hours. The possibility of ovulation and conception prior to initiation of medication should be considered. TriNessa® is available in a blister card with a tablet dispenser which is preset for a Sunday Start. Day 1 Start is also provided.
BRIEF SUMMARY PATIENT PACKAGE INSERT
This product (like all oral contraceptives) does not protect against HIV infection (AIDS) and other sexually transmitted diseases.
Oral contraceptives, also known as "birth control pills" or "the pill," are taken to prevent pregnancy. When taken correctly to prevent pregnancy, oral contraceptives have a failure rate of approximately 1% per year (1 pregnancy per 100 women per year of use) when used without missing any pills. The typical failure rate is approximately 5% per year (5 pregnancies per 100 women per year of use) when women who miss pills are included. For most women oral contraceptives are also free of serious or unpleasant side effects. However, forgetting to take pills considerably increases the chances of pregnancy.
TriNessa® may also be taken to treat moderate acne in females at least 15 years of age, who have started having menstrual periods, are able to take the pill and want to use the pill for birth control.
For the majority of women, oral contraceptives can be taken safely. But there are some women who are at high risk of developing certain serious diseases that can be fatal or may cause temporary or permanent disability. The risks associated with taking oral contraceptives increase significantly if you:
- smoke
- have high blood pressure, diabetes, high cholesterol
- have or have had clotting disorders, heart attack, stroke, angina pectoris, cancer of the breast or sex organs, jaundice or malignant or benign liver tumors.
Although cardiovascular disease risks may be increased with oral contraceptive use after age 40 in healthy, non-smoking women (even with the newer low-dose formulations), there are also greater potential health risks associated with pregnancy in older women.
You should not take the pill if you suspect you are pregnant or have unexplained vaginal bleeding.
DETAILED PATIENT LABELING
PLEASE NOTE: This labeling is revised from time to time as important new medical information becomes available. Therefore, please review this labeling carefully.
This product (like all oral contraceptives) does not protect against HIV infection (AIDS) and other sexually transmitted diseases.
TriNessa® Regimen
Each white tablet contains 0.180 mg norgestimate and 0.035 mg ethinyl estradiol. Each light blue tablet contains 0.215 mg norgestimate and 0.035 mg ethinyl estradiol. Each blue tablet contains 0.250 mg norgestimate and 0.035 mg ethinyl estradiol. Each dark green tablet contains inert ingredients.
INTRODUCTION
Any woman who considers using oral contraceptives (the birth control pill or the pill) should understand the benefits and risks of using this form of birth control. This patient labeling will give you much of the information you will need to make this decision and will also help you determine if you are at risk of developing any of the serious side effects of the pill. It will tell you how to use the pill properly so that it will be as effective as possible. However, this labeling is not a replacement for a careful discussion between you and your healthcare professional. You should discuss the information provided in this labeling with him or her, both when you first start taking the pill and during your revisits. You should also follow your healthcare professional's advice with regard to regular check-ups while you are on the pill.
EFFECTIVENESS OF ORAL CONTRACEPTIVES FOR CONTRACEPTION
Oral contraceptives or "birth control pills" or "the pill" are used to prevent pregnancy and are more effective than most other non-surgical methods of birth control. When they are taken correctly without missing any pills, the chance of becoming pregnant is approximately 1% (1 pregnancy per 100 women per year of use). Typical failure rates, including women who do not always take the pill correctly, are approximately 5% per year (5 pregnancies per 100 women per year of use). The chance of becoming pregnant increases with each missed pill during a menstrual cycle.
In comparison, typical failure rates for other non-surgical methods of birth control during the first year of use are as follows:
| Implant: <1% | Male sterilization: <1% |
| Injection: <1% | Cervical Cap with spermicides: 20 to 40% |
| IUD: 1 to 2% | Condom alone (male): 14% |
| Diaphragm with spermicides: 20% | Condom alone (female): 21% |
| Spermicides alone: 26% | Periodic abstinence: 25% |
| Vaginal sponge: 20 to 40% | Withdrawal: 19% |
| Female sterilization: <1% | No methods: 85% |
TriNessa® may also be taken to treat moderate acne if all of the following are true:
- You have started having menstrual cycles
- You are at least 15 years old
- Your healthcare professional says it is safe for you to use the pill
- You want to use the pill for birth control
WHO SHOULD NOT TAKE ORAL CONTRACEPTIVES
| TRINESSA
norgestimate and ethinyl estradiol kit |
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
| Labeler - Actavis Pharma, Inc (119723554) |
| Registrant - Janssen Ortho LLC (062191882) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Janssen Ortho, LLC | 084894661 | MANUFACTURE(52544-248) , ANALYSIS(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Gedeon Richter Plc | 644781932 | API MANUFACTURE(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Gedeon Richter Plc. | 401140279 | API MANUFACTURE(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Janssen Pharmaceuticals, Inc. | 010779978 | ANALYSIS(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Janssen Pharmaceuticals, Inc. | 063137772 | ANALYSIS(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Aspen Oss B.V. | 491013870 | API MANUFACTURE(52544-248) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Aspen Oss B.V. | 491017488 | API MANUFACTURE(52544-248) | |
