Drug Detail:Uptravi (Selexipag (oral/injection) [ se-lex-i-pag ])
Drug Class: Agents for pulmonary hypertension
Highlights of Prescribing Information
UPTRAVI ® (selexipag) tablets, for oral use
UPTRAVI ® (selexipag) for injection, for intravenous use
Initial U.S. Approval: 2015
Recent Major Changes
| Contraindications ( 4) | 10/2021 |
Indications and Usage for Uptravi
- UPTRAVI is a prostacyclin receptor agonist indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to delay disease progression and reduce the risk of hospitalization for PAH. ( 1.1)
Uptravi Dosage and Administration
- UPTRAVI tablets starting dose: 200 mcg twice daily. ( 2.1)
- Increase the dose by 200 mcg twice daily at weekly intervals to the highest tolerated dose up to 1600 mcg twice daily. ( 2.1)
- Maintenance dose is determined by tolerability. ( 2.1)
- Moderate hepatic impairment: Starting dose 200 mcg once daily, increase the dose by 200 mcg once daily at weekly intervals to the highest tolerated dose up to 1600 mcg. ( 2.5)
- UPTRAVI for injection dose is determined by the patient's current dose of UPTRAVI tablets. Administer UPTRAVI for injection by intravenous infusion, twice daily. ( 2.2)
See Full Prescribing Information for instructions on preparation and administration. ( 2.3).
Dosage Forms and Strengths
- Tablets: 200 mcg, 400 mcg, 600 mcg, 800 mcg, 1000 mcg, 1200 mcg, 1400 mcg, 1600 mcg. ( 3)
- For Injection: 1800 mcg of selexipag as a lyophilized powder in a single-dose vial for reconstitution and dilution. ( 3)
Contraindications
Concomitant use with strong CYP2C8 inhibitors. ( 4, 7.1, 12.3)
Hypersensitivity to the active substance or to any of the excipients. ( 4)
Warnings and Precautions
Pulmonary edema in patients with pulmonary veno-occlusive disease. If confirmed, discontinue treatment. ( 5.1)
Adverse Reactions/Side Effects
Adverse reactions occurring more frequently (≥5%) on UPTRAVI compared to placebo are headache, diarrhea, jaw pain, nausea, myalgia, vomiting, pain in extremity, and flushing. ( 6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Janssen at 1-800-526-7736 (1-800-JANSSEN) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- Moderate CYP2C8 inhibitors (e.g., clopidogrel, deferasirox and teriflunomide) increase exposure to the active metabolite of UPTRAVI. Reduce the dosing of UPTRAVI to once daily ( 2.6, 7.1, 12.3).
- CYP2C8 inducers (e.g., rifampin) decrease exposure to the active metabolite. Increase up to twice the dose of UPTRAVI ( 7.2, 12.3)
Use In Specific Populations
- Nursing mothers: Discontinue UPTRAVI or breastfeeding. ( 8.2)
- Severe hepatic impairment: Avoid use. ( 8.6)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 7/2022
Full Prescribing Information
1. Indications and Usage for Uptravi
1.1 Pulmonary Arterial Hypertension
UPTRAVI is indicated for the treatment of pulmonary arterial hypertension (PAH, WHO Group I) to delay disease progression and reduce the risk of hospitalization for PAH.
Effectiveness of UPTRAVI tablets was established in a long-term study in PAH patients with WHO Functional Class II–III symptoms.
Patients had idiopathic and heritable PAH (58%), PAH associated with connective tissue disease (29%), PAH associated with congenital heart disease with repaired shunts (10%) [see Clinical Studies (14.1)] .
2. Uptravi Dosage and Administration
2.2 Preparation Instructions
Reconstitute and further dilute UPTRAVI for injection prior to intravenous infusion following aseptic procedures.
Determine the dose and total volume of reconstituted UPTRAVI solution required (see Table 1).


Dilution
- UPTRAVI for injection must be diluted in glass containers only.
- Withdraw 100 mL of 0.9% Sodium Chloride Injection, USP and transfer into an empty sterile glass container.
- Withdraw the required volume of reconstituted solution (see Table 1 for reconstituted transfer volume) from the UPTRAVI vial using a single, appropriately sized polypropylene syringe and dilute into the glass container containing 100 mL 0.9% Sodium Chloride Injection, USP to obtain the desired final dose.
- Mix the diluted UPTRAVI infusion solution by gentle inversion of the glass container 5 times. Do not shake.
- Protect diluted UPTRAVI infusion solution from light at all times. Assign a 4-hour expiry from the time of first vial puncture and wrap the glass container completely with light protective cover.
- The UPTRAVI infusion solution should be kept at room temperature (20°C–25°C [68°F–77°F]) and must be infused within 4 hours from the first puncture of the vial stopper (including infusion time).
- Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration. The diluted UPTRAVI infusion solution should be clear and colorless. Discard if particulate matter is observed.
UPTRAVI for injection vials are single-dose, for single administration. All remaining reconstituted product must be discarded.
| UPTRAVI tablets dose (mcg) for twice daily dosing | Corresponding IV UPTRAVI Dose (mcg) for twice daily dosing | Reconstituted transfer volume (mL) for dilution |
|---|---|---|
| 200 | 225 | 1.0 |
| 400 | 450 | 2.0 |
| 600 | 675 | 3.0 |
| 800 | 900 | 4.0 |
| 1000 | 1125 | 5.0 |
| 1200 | 1350 | 6.0 |
| 1400 | 1575 | 7.0 |
| 1600 | 1800 | 8.0 |
2.3 Administration Instructions
Administer by intravenous infusion over 80 minutes using an infusion set made of DEHP-free polyvinyl chloride (PVC), natural latex rubber-free microbore tubing protected from light.
Do not use a filter for administration.
Once the solution for infusion glass container is empty, continue the infusion at the same rate with 0.9% saline to empty the remaining solution for infusion in the IV line, to ensure that the entire solution for infusion has been administered.
2.4 Interruptions and Discontinuations
If a dose of UPTRAVI is missed, patients should take a missed dose as soon as possible unless the next dose is within the next 6 hours.
If treatment is missed for 3 days or more, restart UPTRAVI at a lower dose and then retitrate.
2.5 Dosage Adjustment in Patients with Hepatic Impairment
No dose adjustment of UPTRAVI is necessary for patients with mild hepatic impairment (Child-Pugh class A).
For patients with moderate hepatic impairment (Child-Pugh class B), the starting dose of UPTRAVI tablets is 200 mcg once daily. Increase in increments of 200 mcg once daily at weekly intervals, as tolerated [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)] .
Avoid use of UPTRAVI in patients with severe hepatic impairment (Child-Pugh class C).
3. Dosage Forms and Strengths
UPTRAVI is available in the following presentations:
Film-Coated Tablets
- 200 mcg selexipag [Light yellow tablet debossed with 2]
- 400 mcg selexipag [Red tablet debossed with 4]
- 600 mcg selexipag [Light violet tablet debossed with 6]
- 800 mcg selexipag [Green tablet debossed with 8]
- 1000 mcg selexipag [Orange tablet debossed with 10]
- 1200 mcg selexipag [Dark violet tablet debossed with 12]
- 1400 mcg selexipag [Dark yellow tablet debossed with 14]
- 1600 mcg selexipag [Brown tablet debossed with 16]
UPTRAVI for Injection
- 1800 mcg selexipag [Lyophilized powder white to almost white broken cake or powdered material, supplied in a 10 mL single-dose glass vial]
4. Contraindications
Hypersensitivity to the active substance or to any of the excipients.
Concomitant use of strong inhibitors of CYP2C8 (e.g., gemfibrozil) [see Drug Interactions (7.1) and Clinical Pharmacology (12.3)] .
6. Adverse Reactions/Side Effects
6.1 Clinical Trial Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
6.2 Postmarketing Experience
The following adverse reactions have been identified during post approval use of UPTRAVI.
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Vascular disorders: symptomatic hypotension
7. Drug Interactions
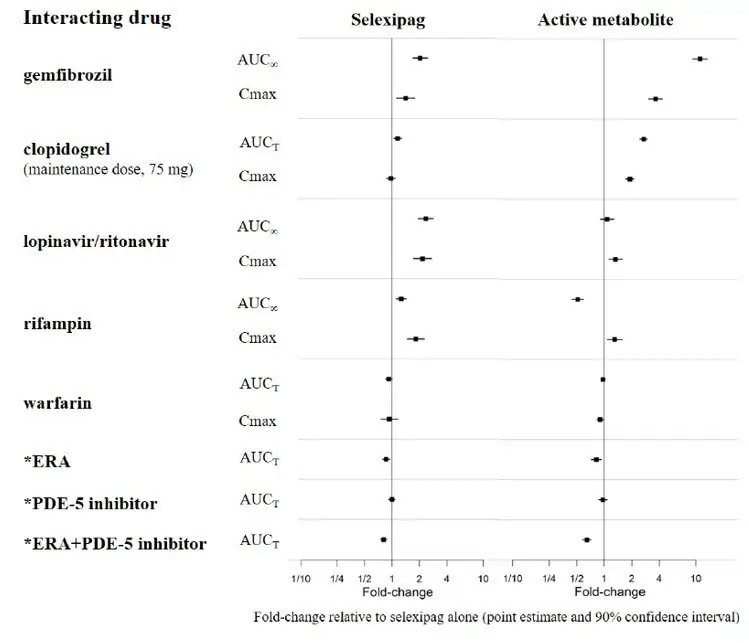
7.1 CYP2C8 Inhibitors
Concomitant administration with gemfibrozil, a strong inhibitor of CYP2C8, doubled the exposure to selexipag and increased exposure to the active metabolite by approximately 11-fold. Concomitant administration of UPTRAVI with strong inhibitors of CYP2C8 (e.g., gemfibrozil) is contraindicated [see Contraindications (4) and Clinical Pharmacology (12.3)] .
Concomitant administration of UPTRAVI tablets with clopidogrel, a moderate inhibitor of CYP2C8, had no relevant effect on the exposure to selexipag and increased the exposure to the active metabolite by approximately 2.7-fold [see Clinical Pharmacology (12.3)] . Reduce the dosing of UPTRAVI to once daily in patients on a moderate CYP2C8 inhibitor [see Dosage and Administration (2.6)] .
7.2 CYP2C8 Inducers
Concomitant administration with an inducer of CYP2C8 and UGT 1A3 and 2B7 enzymes (rifampin) halved exposure to the active metabolite. Increase dose up to twice of UPTRAVI when co-administered with rifampin. Reduce UPTRAVI when rifampin is stopped [see Clinical Pharmacology (12.3)] .
8. Use In Specific Populations
8.2 Lactation
It is not known if UPTRAVI is present in human milk. Selexipag or its metabolites were present in the milk of rats. Because many drugs are present in the human milk and because of the potential for serious adverse reactions in nursing infants, discontinue nursing or discontinue UPTRAVI.
8.5 Geriatric Use
Of the 1,368 subjects in clinical studies of UPTRAVI tablets, 248 subjects were 65 years of age and older, while 19 were 75 and older. No overall differences were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity cannot be ruled out.
8.6 Patients with Hepatic Impairment
No adjustment to the dosing regimen is needed in patients with mild hepatic impairment (Child-Pugh class A).
A once-daily regimen is recommended in patients with moderate hepatic impairment (Child-Pugh class B) due to the increased exposure to selexipag and its active metabolite. There is no experience with UPTRAVI in patients with severe hepatic impairment (Child-Pugh class C). Avoid use of UPTRAVI in patients with severe hepatic impairment [see Dosage and Administration (2.5) and Clinical Pharmacology (12.3)] .
8.7 Patients with Renal Impairment
No adjustment to the dosing regimen is needed in patients with estimated glomerular filtration rate >15 mL/min/1.73 m 2.
There is no clinical experience with UPTRAVI in patients undergoing dialysis or in patients with glomerular filtration rates <15 mL/min/1.73 m 2 [see Clinical Pharmacology (12.3)] .
10. Overdosage
Isolated cases of overdose with UPTRAVI tablets up to 3200 mcg were reported. Mild, transient nausea was the only reported consequence. In the event of overdose, supportive measures must be taken as required. Dialysis is unlikely to be effective because selexipag and its active metabolite are highly protein-bound.
11. Uptravi Description
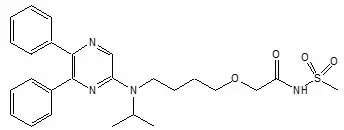
UPTRAVI contains selexipag, a prostacyclin receptor agonist. The chemical name of selexipag is 2-{4-[(5,6-diphenylpyrazin-2-yl)(isopropyl)amino]butoxy}- N-(methylsulfonyl) acetamide. It has a molecular formula of C 26H 32N 4O 4S and a molecular weight of 496.62. Selexipag has the following structural formula:
Selexipag is a pale yellow crystalline powder that is practically insoluble in water. In the solid state selexipag is very stable, is not hygroscopic, and is not light sensitive.
UPTRAVI ® (selexipag) tablets: depending on the dose strength, each round film-coated tablet for oral administration contains 200, 400, 600, 800, 1000, 1200, 1400, or 1600 mcg of selexipag. The tablets include the following inactive ingredients: corn starch, D-mannitol, hydroxypropyl cellulose, low substituted hydroxypropyl cellulose, and magnesium stearate. The tablets are film coated with a coating material containing carnauba wax, hypromellose, propylene glycol, titanium dioxide, along with mixtures of iron oxide black, iron oxide red or iron oxide yellow.
UPTRAVI ® (selexipag) for injection: contains 1800 mcg of selexipag per vial. UPTRAVI for injection includes the following inactive ingredients: glycine (180 mg), phosphoric acid (3.53 mg), polysorbate 20 (10.8 mg) and sodium hydroxide (for pH adjustment). UPTRAVI for injection is provided in 10 mL Type I clear glass vials closed by a stopper and tear-off aluminum seal.
12. Uptravi - Clinical Pharmacology
12.1 Mechanism of Action
Selexipag is a prostacyclin receptor (IP receptor) agonist that is structurally distinct from prostacyclin. Selexipag is hydrolyzed by carboxylesterase 1 to yield its active metabolite, which is approximately 37-fold as potent as selexipag. Selexipag and the active metabolite are selective for the IP receptor versus other prostanoid receptors (EP 1–4, DP, FP, and TP).
12.3 Pharmacokinetics
The pharmacokinetics of selexipag and its active metabolite have been studied primarily in healthy subjects. The pharmacokinetics of selexipag and the active metabolite, after both single- and multiple-dose oral administration, were dose-proportional up to a single dose of 800 mcg and multiple doses of up to 1800 mcg twice daily. The pharmacokinetics of selexipag and the active metabolite, after multiple-dose intravenous administration, were dose-proportional in the tested dose range from 450 to 1800 mcg twice a day.
In healthy subjects, inter-subject variability in exposure (area under the curve over a dosing interval, AUC) at steady-state following oral administration was 43% and 39% for selexipag and the active metabolite, respectively. Intra-subject variability in exposure was 24% and 19% for selexipag and the active metabolite, respectively.
Exposures to selexipag and the active metabolite at steady-state in PAH patients and healthy subjects were similar. The pharmacokinetics of selexipag and the active metabolite in PAH patients were not influenced by the severity of the disease and did not change with time.
The corresponding UPTRAVI tablets and UPTRAVI for injection doses (Table 1) provide similar exposure to the active metabolite in PAH patients at steady-state, whereas the exposure to selexipag is approximately twice as high after intravenous administration compared to oral administration.
Both in healthy subjects and PAH patients, after oral administration, exposure at steady-state to the active metabolite is approximately 3- to 4-fold that of selexipag.
14. Clinical Studies
14.1 Efficacy of UPTRAVI Tablets in Patients with Pulmonary Arterial Hypertension
The effect of UPTRAVI tablets on progression of PAH was demonstrated in a multi-center, double-blind, placebo-controlled, parallel group, event-driven study (GRIPHON) in 1,156 patients with symptomatic (WHO Functional Class I [0.8%], II [46%], III [53%], and IV [1%]) PAH. Patients were randomized to either placebo (N=582), or UPTRAVI tablets (N=574). The dose was increased in weekly intervals by increments of 200 mcg twice a day to the highest tolerated dose up to 1600 mcg twice a day.
The primary study endpoint was the time to first occurrence up to end-of-treatment of: a) death, b) hospitalization for PAH, c) PAH worsening resulting in need for lung transplantation, or balloon atrial septostomy, d) initiation of parenteral prostanoid therapy or chronic oxygen therapy, or e) other disease progression based on a 15% decrease from baseline in 6MWD plus worsening of Functional Class or need for additional PAH-specific therapy.
The mean age was 48 years, the majority of patients were white (65%) and female (80%). Nearly all patients were in WHO Functional Class II and III at baseline.
Idiopathic or heritable PAH was the most common etiology in the study population (58%) followed by PAH associated with connective tissue disease (29%), PAH associated with congenital heart disease with repaired shunts (10%), drugs and toxins (2%), and HIV (1%).
At baseline, the majority of enrolled patients (80%) were being treated with a stable dose of an endothelin receptor antagonist (15%), a PDE-5 inhibitor (32%), or both (33%).
Patients on UPTRAVI tablets achieved doses within the following groups: 200–400 mcg (23%), 600–1000 mcg (31%) and 1200–1600 mcg (43%).
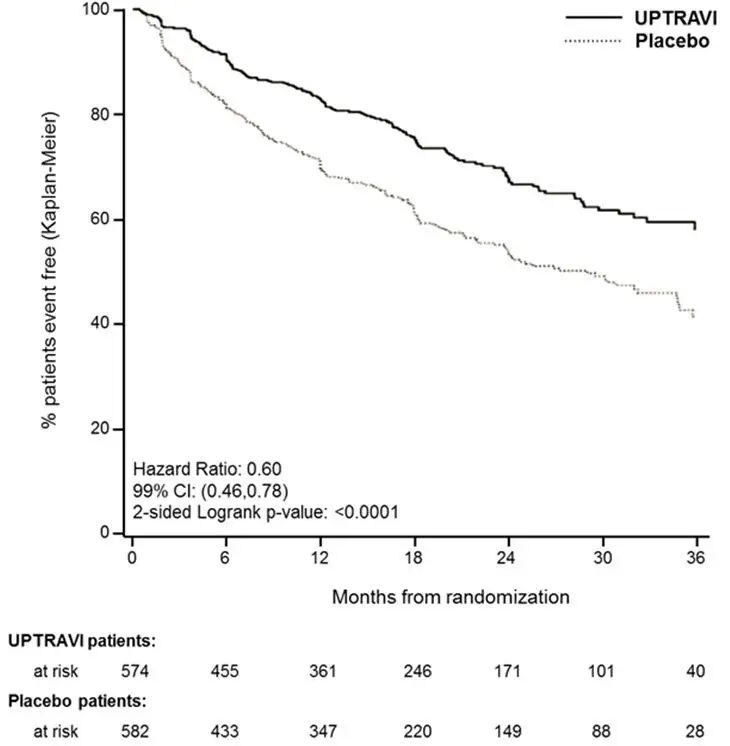
Treatment with UPTRAVI tablets resulted in a 40% reduction (99% CI: 22 to 54%; two-sided log-rank p-value <0.0001) of the occurrence of primary endpoint events compared to placebo (Table 3; Figure 3). The beneficial effect of UPTRAVI was primarily attributable to a reduction in hospitalization for PAH and a reduction in other disease progression events (Table 3). The observed benefit of UPTRAVI was similar regardless of the dose achieved when patients were titrated to their highest tolerated dose [see Dosage and Administration (2.1)] .
Figure 3 Kaplan-Meier Estimates of the First Morbidity-Mortality Event in GRIPHON
| UPTRAVI
N=574 | Placebo
N=582 | Hazard Ratio
(99% CI) | p-value | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Primary endpoint events up to the end of treatment | ||||||
| All primary endpoint events
As first event: | 155 | 27.0 | 242 | 41.6 | 0.60 [0.46, 0.78] | <0.0001 |
| 78 | 13.6 | 109 | 18.7 | ||
| 38 | 6.6 | 100 | 17.2 | ||
| 28 | 4.9 | 18 | 3.1 | ||
| 10 | 1.7 | 13 | 2.2 | ||
| 1 | 0.2 | 2 | 0.3 | ||
It is not known if the excess number of deaths in the UPTRAVI group is drug-related because there were so few deaths and the imbalance was not observed until 18 months into GRIPHON.
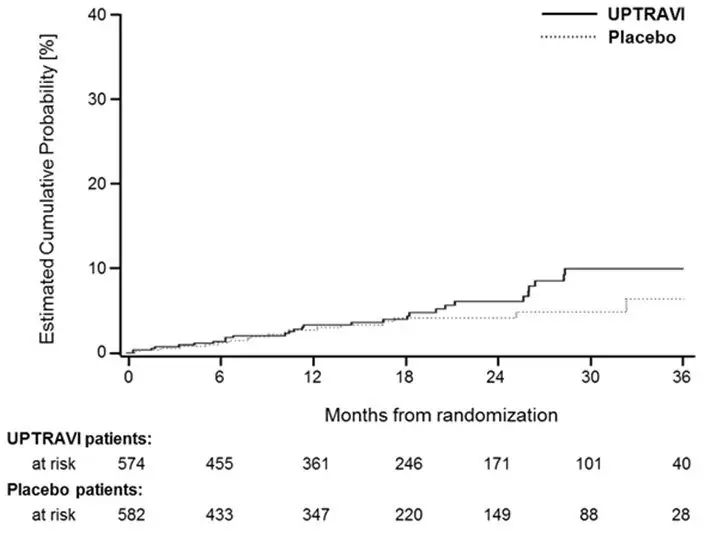
Figures 4A, B, and C show time to first event analyses for primary endpoint components of hospitalization for PAH (A), other disease progression (B), and death (C) all censored 7 days after any primary end point event (because many patients on placebo transitioned to open-label UPTRAVI at this point).
Figure 4A Hospitalization for PAH as the First Endpoint in GRIPHON
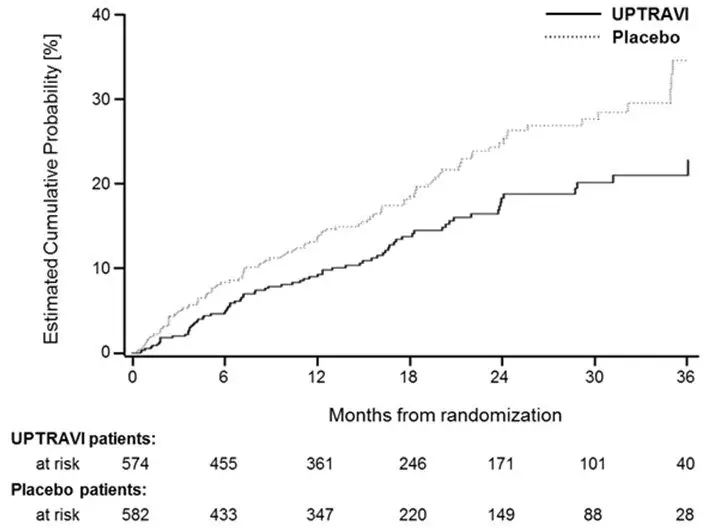
Figure 4B Disease Progression as the First Endpoint in GRIPHON
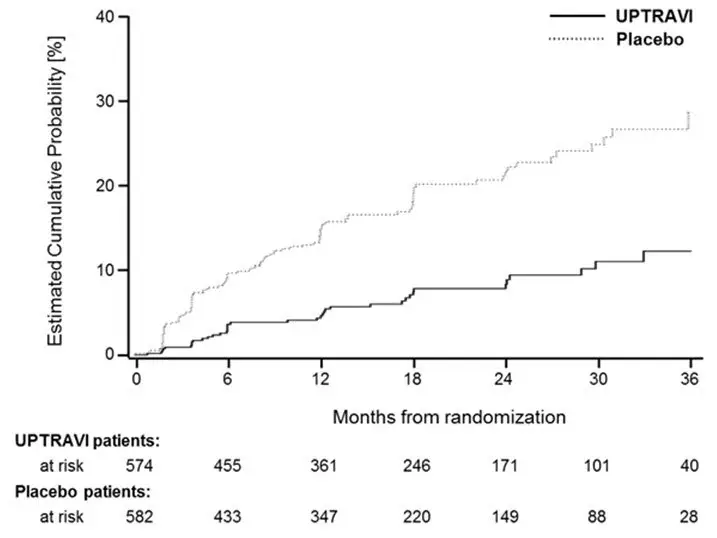
Figure 4C Death as the First Endpoint in GRIPHON
The treatment effect of UPTRAVI on time to first primary event was consistent irrespective of background PAH therapy (i.e., in combination with an ERA, PDE-5i, both, or without background therapy) (Figure 5).
Figure 5 Subgroup Analyses of the Primary Endpoint in GRIPHON
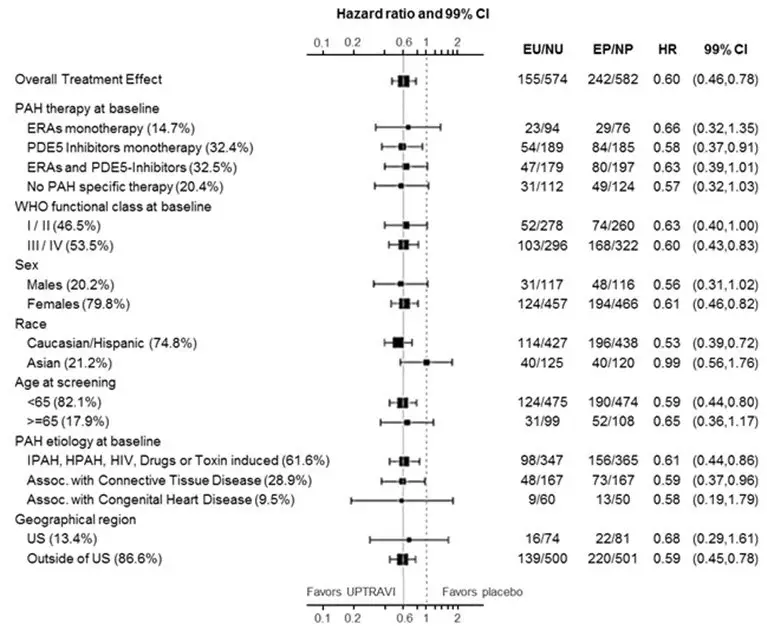
Note: Race group "Other" is not displayed in analysis, as the population is less than 30. EU = Number of UPTRAVI patients with events, NU = Number of patients randomized to UPTRAVI, EP = Number of Placebo patients with events, NP = Number of patients randomized to Placebo, HR = Hazard Ratio, CI = Confidence Interval, the size of the squares represent the number of patients in the subgroup.
Note: The figure above presents effects in various subgroups all of which are baseline characteristics and all were pre-specified. The 99% confidence limits that are shown do not take into account how many comparisons were made, nor do they reflect the effect of a particular factor after adjustment for all other factors. Apparent homogeneity or heterogeneity among groups should not be over-interpreted.
16. How is Uptravi supplied
UPTRAVI ® (selexipag) film-coated, round tablets are supplied in the following configurations:
| Strength
(mcg) | Color | Debossing | NDC-XXX
Bottle of 60 | NDC-XXX
Bottle of 140 |
|---|---|---|---|---|
| 200 | Light yellow | 2 | 66215-602-06 | 66215-602-14 |
| 400 | Red | 4 | 66215-604-06 | Not Available |
| 600 | Light violet | 6 | 66215-606-06 | Not Available |
| 800 | Green | 8 | 66215-608-06 | Not Available |
| 1000 | Orange | 10 | 66215-610-06 | Not Available |
| 1200 | Dark violet | 12 | 66215-612-06 | Not Available |
| 1400 | Dark yellow | 14 | 66215-614-06 | Not Available |
| 1600 | Brown | 16 | 66215-616-06 | Not Available |
UPTRAVI ® (selexipag) tablets are also supplied in a Titration Pack [NDC 66215-628-20] that includes a 140-count bottle of 200-mcg tablets and a 60-count bottle of 800-mcg tablets.










| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
|
||||||||||||||||||||||||
| UPTRAVI
selexipag tablet, coated |
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||
| UPTRAVI TITRATION PACK
selexipag kit |
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
|
||||||||||||||||||||||||||
| UPTRAVI
selexipag injection, powder, for solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Actelion Pharmaceuticals US, Inc. (002641228) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Excella GmbH | 329809800 | analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) , label(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) , manufacture(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) , pack(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Almac Sciences Limited | 232665666 | api manufacture(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628, 66215-718) , analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628, 66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Butterworth Laboratories Ltd | 225081538 | analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Almac Pharma Services Limited | 233170864 | analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628, 66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| SGS Institut Fresenius GmbH | 317219699 | analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| SGS Institut Fresenius GmbH | 341259550 | analysis(66215-602, 66215-604, 66215-606, 66215-608, 66215-610, 66215-612, 66215-614, 66215-616, 66215-628) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| EUROFINS AMATSIGROUP SAS | 265402977 | manufacture(66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Wickham Micro Limited | 228216353 | analysis(66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Eurofins Amatsi Analytics | 270324185 | analysis(66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Confarma France | 492738125 | analysis(66215-718) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Konapharma AG | 482314432 | manufacture(66215-718) | |