Drug Detail:Xolair (Omalizumab [ oh-ma-liz-oo-mab ])
Drug Class: Selective immunosuppressants
Highlights of Prescribing Information
XOLAIR® (omalizumab) injection, for subcutaneous use
XOLAIR® (omalizumab) for injection, for subcutaneous use
Initial U.S. Approval: 2003
WARNING: ANAPHYLAXIS
See full prescribing information for complete boxed warning.
Anaphylaxis, presenting as bronchospasm, hypotension, syncope, urticaria, and/or angioedema of the throat or tongue, has been reported to occur after administration of XOLAIR. Anaphylaxis has occurred after the first dose of XOLAIR but also has occurred beyond 1 year after beginning treatment. Initiate XOLAIR therapy in a healthcare setting, closely observe patients for an appropriate period of time after XOLAIR administration and be prepared to manage anaphylaxis which can be life-threatening. Inform patients of the signs and symptoms of anaphylaxis and have them seek immediate medical care should symptoms occur. Selection of patients for self-administration of XOLAIR should be based on criteria to mitigate risk from anaphylaxis. (2.5, 5.1, 6.1, 6.3)
Indications and Usage for Xolair
XOLAIR is an anti-IgE antibody indicated for:
- Moderate to severe persistent asthma in adults and pediatric patients 6 years of age and older with a positive skin test or in vitro reactivity to a perennial aeroallergen and symptoms that are inadequately controlled with inhaled corticosteroids (1.1)
- Chronic rhinosinusitis with nasal polyps (CRSwNP) in adult patients 18 years of age and older with inadequate response to nasal corticosteroids, as add-on maintenance treatment (1.2)
- Chronic spontaneous urticaria (CSU) in adults and adolescents 12 years of age and older who remain symptomatic despite H1 antihistamine treatment (1.3)
Limitations of Use:
- Not indicated for acute bronchospasm or status asthmaticus. (1.1, 5.3)
- Not indicated for other allergic conditions or other forms of urticaria. (1.1, 1.3)
Xolair Dosage and Administration
For subcutaneous (SC) administration only. (2.2, 2.3, 2.4, 2.5)
Divide doses of more than 150 mg among more than one injection site to limit injections to not more than 150 mg per site. (2.6, 2.7)
- Asthma: XOLAIR 75 to 375 mg SC every 2 or 4 weeks. Determine dose (mg) and dosing frequency by serum total IgE level (IU/mL), measured before the start of treatment, and body weight (kg). See the dose determination charts. (2.2)
- Chronic Rhinosinusitis with Nasal Polyps: XOLAIR 75 to 600 mg SC every 2 or 4 weeks. Determine dose (mg) and dosing frequency by serum total IgE level (IU/mL), measured before the start of treatment, and body weight (kg). See the dose determination charts. (2.3)
- Chronic Spontaneous Urticaria: XOLAIR 150 or 300 mg SC every 4 weeks. Dosing in CSU is not dependent on serum IgE level or body weight. (2.4)
Dosage Forms and Strengths
- Injection: 75 mg/0.5 mL and 150 mg/mL solution in a single-dose prefilled syringe (3)
- For Injection: 150 mg lyophilized powder in a single-dose vial for reconstitution (3)
Contraindications
Severe hypersensitivity reaction to XOLAIR or any ingredient of XOLAIR (4, 5.1)
Warnings and Precautions
- Anaphylaxis: Initiate XOLAIR therapy in a healthcare setting prepared to manage anaphylaxis which can be life-threatening and observe patients for an appropriate period of time after administration. (5.1)
- Malignancy: Malignancies have been observed in clinical studies. (5.2)
- Acute Asthma Symptoms: Do not use for the treatment of acute bronchospasm or status asthmaticus. (5.3)
- Corticosteroid Reduction: Do not abruptly discontinue corticosteroids upon initiation of XOLAIR therapy. (5.4)
- Eosinophilic Conditions: Be alert to eosinophilia, vasculitic rash, worsening pulmonary symptoms, cardiac complications, and/or neuropathy, especially upon reduction of oral corticosteroids. (5.5)
- Fever, Arthralgia, and Rash: Stop XOLAIR if patients develop signs and symptoms similar to serum sickness. (5.6)
Adverse Reactions/Side Effects
- Asthma: The most common adverse reactions (≥ 1% of patients) in clinical studies with adult and adolescent patients ≥12 years of age were arthralgia, pain (general), leg pain, fatigue, dizziness, fracture, arm pain, pruritus, dermatitis, and earache. In clinical studies with pediatric patients 6 to <12 years of age, the most common adverse reactions were nasopharyngitis, headache, pyrexia, upper abdominal pain, pharyngitis streptococcal, otitis media, viral gastroenteritis, arthropod bites, and epistaxis. (6.1)
- Chronic Rhinosinusitis with Nasal Polyps: The most common adverse reactions (≥ 3% of patients) in clinical studies with adult patients included the following: headache, injection site reaction, arthralgia, upper abdominal pain, and dizziness. (6.1)
- Chronic Spontaneous Urticaria: The most common adverse reactions (≥2% of patients) included the following: nausea, nasopharyngitis, sinusitis, upper respiratory tract infection, viral upper respiratory tract infection, arthralgia, headache, and cough. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
No formal drug interaction studies have been performed. (7)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 3/2023
Full Prescribing Information
WARNING: ANAPHYLAXIS
Anaphylaxis presenting as bronchospasm, hypotension, syncope, urticaria, and/or angioedema of the throat or tongue, has been reported to occur after administration of XOLAIR. Anaphylaxis has occurred as early as after the first dose of XOLAIR, but also has occurred beyond 1 year after beginning regularly administered treatment. Because of the risk of anaphylaxis, initiate XOLAIR therapy in a healthcare setting and closely observe patients for an appropriate period of time after XOLAIR administration. Health care providers administering XOLAIR should be prepared to manage anaphylaxis which can be life-threatening. Inform patients of the signs and symptoms of anaphylaxis and instruct them to seek immediate medical care should symptoms occur. Selection of patients for self-administration of XOLAIR should be based on criteria to mitigate risk from anaphylaxis [see Dosage and Administration (2.5), Warnings and Precautions (5.1) and Adverse Reactions (6.1, 6.3)].
1. Indications and Usage for Xolair
1.1 Asthma
XOLAIR is indicated for adults and pediatric patients 6 years of age and older with moderate to severe persistent asthma who have a positive skin test or in vitro reactivity to a perennial aeroallergen and whose symptoms are inadequately controlled with inhaled corticosteroids.
1.2 Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
XOLAIR is indicated for add-on maintenance treatment of chronic rhinosinusitis with nasal polyps (CRSwNP) in adult patients 18 years of age and older with inadequate response to nasal corticosteroids.
2. Xolair Dosage and Administration
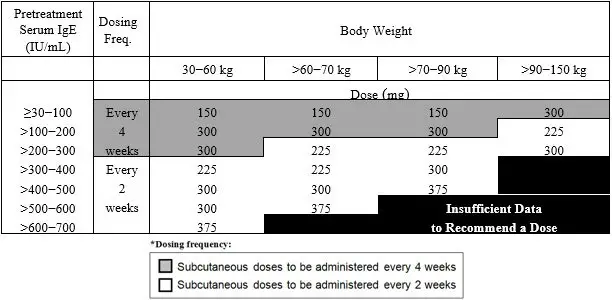
2.2 Recommended Dosage for Asthma
The recommended dosage for treatment of asthma is XOLAIR 75 mg to 375 mg by subcutaneous injection every 2 or 4 weeks based on serum total IgE level (IU/mL) measured before the start of treatment and by body weight (kg) [see Dosage and Administration (2.1)].
- Adult and adolescent patients 12 years of age and older: Initiate dosing according to Table 1.
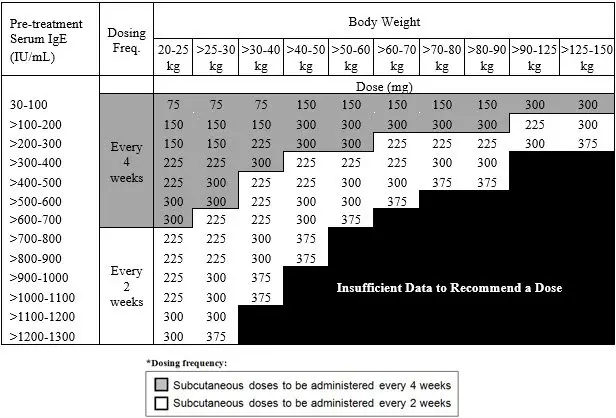
- Pediatric patients 6 to <12 years of age: Initiate dosing according to Table 2.
 |
 |
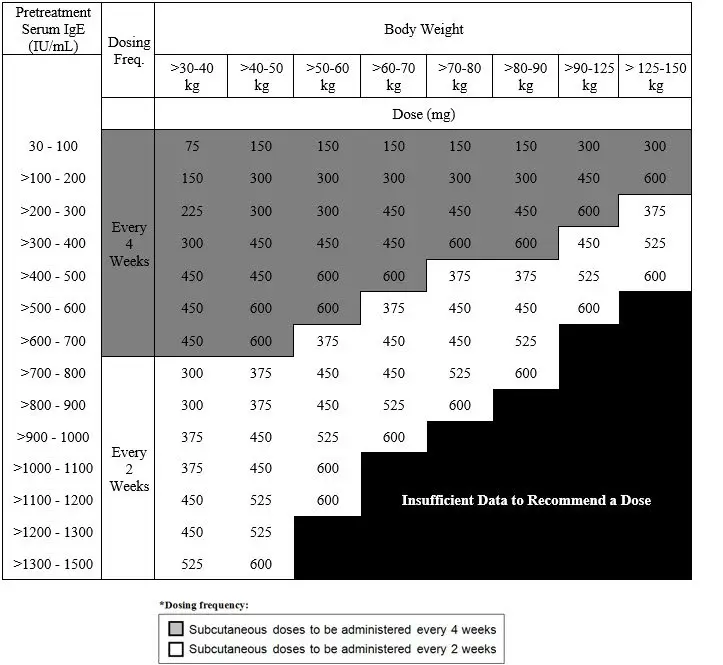
2.3 Recommended Dosage for Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
Administer XOLAIR 75 mg to 600 mg by subcutaneous injection every 2 or 4 weeks based on serum total IgE level (IU/mL) measure before the start of treatment and by body weight (kg) [see Dosage and Administration (2.1)].
 |
2.4 Recommended Dosage for Chronic Spontaneous Urticaria (CSU)
Administer XOLAIR 150 mg or 300 mg by subcutaneous injection every 4 weeks. Dosing of XOLAIR in CSU patients is not dependent on serum IgE (free or total) level or body weight.
2.5 Administration Overview
Administer XOLAIR by subcutaneous injection. XOLAIR is intended for use under the guidance of a healthcare provider. Initiate therapy in a healthcare setting and once therapy has been safely established, the healthcare provider may determine whether self-administration of XOLAIR prefilled syringe by the patient or caregiver is appropriate, based on careful assessment of risk for anaphylaxis and mitigation strategies.
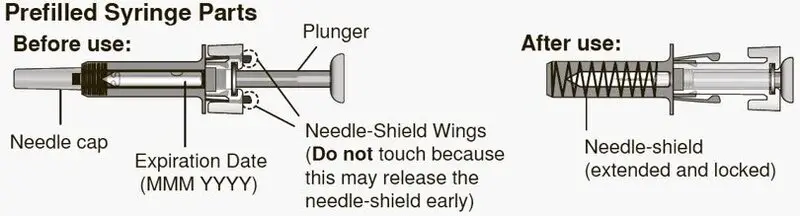
2.6 XOLAIR Prefilled Syringe
Instruct patients or caregivers to follow the directions provided in the "Instructions for Use" for preparation and administration of XOLAIR Prefilled Syringe [see Instructions for Use].
- Adolescents 12 years of age and older: XOLAIR prefilled syringe may be self-administered under adult supervision.
- Pediatric Patients 6 to 11 years of age: XOLAIR prefilled syringe should be administered by a caregiver.
Administration Instructions
- Visually inspect the contents of the prefilled syringe for particulate matter and discoloration prior to administration. XOLAIR prefilled syringe solution should be clear and colorless to pale brownish yellow. Do not use the prefilled syringe if the medicine is cloudy, discolored, or contains particles.
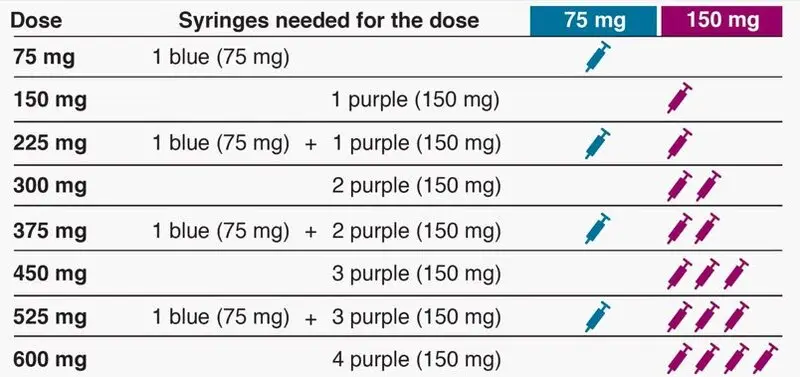
- Determine the number of Prefilled Syringes needed for patient's dosage (see Table 4).
- For patients requiring more than 1 injection to complete a full dose, administer each injection at least 1 inch apart from other injection sites.
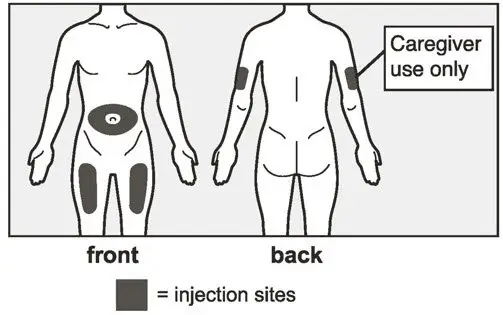
- Administer subcutaneous injection into the thigh or abdomen, avoiding the 2-inch (5 cm) area directly around the navel. The outer area of the upper arms may be used only if the injection is being given by a caregiver or healthcare provider [see Instructions for Use]. The injection may take 5-10 seconds to administer.
| XOLAIR Dose* | 75 mg Syringes | 150 mg Syringes | Total Volume Injected |
|---|---|---|---|
|
|||
| 75 mg | 1 | 0 | 0.5 mL |
| 150 mg | 0 | 1 | 1 mL |
| 225 mg | 1 | 1 | 1.5 mL |
| 300 mg | 0 | 2 | 2 mL |
| 375 mg | 1 | 2 | 2.5 mL |
| 450 mg | 0 | 3 | 3 mL |
| 525 mg | 1 | 3 | 3.5 mL |
| 600 mg | 0 | 4 | 4 mL |
2.7 Preparation for Use and Injection of XOLAIR Lyophilized Powder
XOLAIR lyophilized powder should only be prepared and injected by a healthcare provider. The supplied XOLAIR lyophilized powder must be reconstituted with Sterile Water for Injection (SWFI) USP, using the following instructions:
- 1)
- Before reconstitution, determine the number of vials that will need to be reconstituted (each vial delivers 150 mg of XOLAIR in 1.2 mL) (see Table 5).
| XOLAIR Dose* | Number of Vials | Number of Injections | Total Volume Injected |
|---|---|---|---|
|
|||
| 75 mg | 1 | 1 | 0.6 mL |
| 150 mg | 1 | 1 | 1.2 mL |
| 225 mg | 2 | 2 | 1.8 mL |
| 300 mg | 2 | 2 | 2.4 mL |
| 375 mg | 3 | 3 | 3.0 mL |
| 450 mg | 3 | 3 | 3.6 mL |
| 525 mg | 4 | 4 | 4.2 mL |
| 600 mg | 4 | 4 | 4.8 mL |
- 2)
- Draw 1.4 mL of SWFI, USP, into a 3 mL syringe equipped with a 1-inch, 18-gauge needle.
- 3)
- Place the vial upright on a flat surface and using standard aseptic technique, insert the needle and inject the SWFI, USP, directly onto the product.
- 4)
- Keeping the vial upright, gently swirl the upright vial for approximately 1 minute to evenly wet the powder. Do not shake.
- 5)
- Gently swirl the vial for 5 to 10 seconds approximately every 5 minutes in order to dissolve any remaining solids. The lyophilized product takes 15 to 20 minutes to dissolve. If it takes longer than 20 minutes to dissolve completely, gently swirl the vial for 5 to 10 seconds approximately every 5 minutes until there are no visible gel-like particles in the solution. Do not use if the contents of the vial do not dissolve completely by 40 minutes.
- 6)
- After reconstitution, XOLAIR solution is somewhat viscous and will appear clear or slightly opalescent. It is acceptable if there are a few small bubbles or foam around the edge of the vial; there should be no visible gel-like particles in the reconstituted solution. Do not use if foreign particles are present.
- 7)
- Invert the vial for 15 seconds in order to allow the solution to drain toward the stopper.
- 8)
- Use the XOLAIR solution within 8 hours following reconstitution when stored in the vial at 2ºC to 8ºC (36ºF to 46ºF), or within 4 hours of reconstitution when stored at room temperature. Reconstituted XOLAIR vials should be protected from sunlight.
- 9)
- Using a new 3 mL syringe equipped with a 1-inch, 18-gauge needle, insert the needle into the inverted vial. Position the needle tip at the very bottom of the solution in the vial stopper when drawing the solution into the syringe. The reconstituted product is somewhat viscous. Withdraw all of the product from the vial before expelling any air or excess solution from the syringe. Before removing the needle from the vial, pull the plunger all the way back to the end of the syringe barrel in order to remove all of the solution from the inverted vial.
- 10)
- Replace the 18-gauge needle with a 25-gauge needle for subcutaneous injection.
- 11)
- Expel air, large bubbles, and any excess solution in order to obtain a volume of 1.2 mL corresponding to a dose of 150 mg of XOLAIR. To obtain a volume of 0.6 mL corresponding to a dose of 75 mg of XOLAIR, expel air, large bubbles and discard 0.6 mL from the syringe. A thin layer of small bubbles may remain at the top of the solution in the syringe.
- 12)
- Administer XOLAIR by subcutaneous injection. The injection may take 5-10 seconds to administer because the solution is slightly viscous. Do not administer more than 150 mg (contents of one vial) per injection site. Divide doses of more than 150 mg between two or more injection sites. Choose a different injection site for each new injection at least 1 inch from the area used for other injections.
3. Dosage Forms and Strengths
- Injection: 75 mg/0.5 mL is a clear to slightly opalescent and colorless to pale brownish-yellow solution in a single-dose prefilled syringe with blue needle shield
- Injection: 150 mg/mL is a clear to slightly opalescent and colorless to pale brownish-yellow solution in a single-dose prefilled syringe with purple needle shield
- For injection: 150 mg white lyophilized powder in a single-dose vial for reconstitution
4. Contraindications
XOLAIR is contraindicated in patients with severe hypersensitivity reaction to XOLAIR or any ingredient of XOLAIR [see Warnings and Precautions (5.1)].
5. Warnings and Precautions
5.1 Anaphylaxis
Anaphylaxis has been reported to occur after administration of XOLAIR in premarketing clinical trials and in postmarketing spontaneous reports [see Boxed Warning and Adverse Reactions (6.3)]. Signs and symptoms in these reported cases have included bronchospasm, hypotension, syncope, urticaria, and/or angioedema of the throat or tongue. Some of these events have been life-threatening. In premarketing clinical trials in patients with asthma, anaphylaxis was reported in 3 of 3507 (0.1%) patients. Anaphylaxis occurred with the first dose of XOLAIR in two patients and with the fourth dose in one patient. The time to onset of anaphylaxis was 90 minutes after administration in two patients and 2 hours after administration in one patient.
A case-control study showed that, among XOLAIR users, patients with a history of anaphylaxis to foods, medications, or other causes were at increased risk of anaphylaxis associated with XOLAIR, compared to those with no prior history of anaphylaxis [see Adverse Reactions (6.1)].
In postmarketing spontaneous reports, the frequency of anaphylaxis attributed to XOLAIR use was estimated to be at least 0.2% of patients based on an estimated exposure of about 57,300 patients from June 2003 through December 2006. Anaphylaxis has occurred as early as after the first dose of XOLAIR, but also has occurred beyond one year after beginning regularly scheduled treatment. Approximately 60% to 70% of anaphylaxis cases have been reported to occur within the first three doses of XOLAIR, with additional cases occurring sporadically beyond the third dose.
Initiate XOLAIR only in a healthcare setting equipped to manage anaphylaxis, which can be life-threatening. Observe patients closely for an appropriate period of time after administration of XOLAIR, taking into account the time to onset of anaphylaxis seen in premarketing clinical trials and postmarketing spontaneous reports [see Adverse Reactions (6)]. Inform patients of the signs and symptoms of anaphylaxis, and instruct them to seek immediate medical care should signs or symptoms occur.
Once XOLAIR therapy has been established, administration of XOLAIR Prefilled Syringe outside of a healthcare setting by a patient or a caregiver may be appropriate for selected patients. Patient selection, determined by the healthcare provider in consultation with the patient, should take into account the pattern of anaphylaxis events seen in premarketing clinical trials and postmarketing spontaneous reports, as well as individual patient risk factors (e.g. prior history of anaphylaxis), ability to recognize signs and symptoms of anaphylaxis, and ability to perform subcutaneous injections with XOLAIR Prefilled Syringe with proper technique according to the prescribed dosing regimen and Instructions for Use [see Dosage and Administration (2.5), Adverse Reactions (6)].
Discontinue XOLAIR in patients who experience a severe hypersensitivity reaction [see Contraindications (4)].
5.2 Malignancy
Malignant neoplasms were observed in 20 of 4127 (0.5%) XOLAIR-treated patients compared with 5 of 2236 (0.2%) control patients in clinical studies of adults and adolescents ≥12 years of age with asthma and other allergic disorders. The observed malignancies in XOLAIR-treated patients were a variety of types, with breast, non-melanoma skin, prostate, melanoma, and parotid occurring more than once, and five other types occurring once each. The majority of patients were observed for less than 1 year. The impact of longer exposure to XOLAIR or use in patients at higher risk for malignancy (e.g., elderly, current smokers) is not known.
In a subsequent observational study of 5007 XOLAIR-treated and 2829 non-XOLAIR-treated adolescent and adult patients with moderate to severe persistent asthma and a positive skin test reaction or in vitro reactivity to a perennial aeroallergen, patients were followed for up to 5 years. In this study, the incidence rates of primary malignancies (per 1000 patient years) were similar among XOLAIR-treated (12.3) and non-XOLAIR-treated patients (13.0) [see Adverse Reactions (6)]. However, study limitations preclude definitively ruling out a malignancy risk with XOLAIR. Study limitations include: the observational study design, the bias introduced by allowing enrollment of patients previously exposed to XOLAIR (88%), enrollment of patients (56%) while a history of cancer or a premalignant condition were study exclusion criteria, and the high study discontinuation rate (44%).
5.3 Acute Asthma Symptoms and Deteriorating Disease
XOLAIR has not been shown to alleviate asthma exacerbations acutely. Do not use XOLAIR to treat acute bronchospasm or status asthmaticus. Patients should seek medical advice if their asthma remains uncontrolled or worsens after initiation of treatment with XOLAIR.
5.4 Corticosteroid Reduction
Do not discontinue systemic or inhaled corticosteroids abruptly upon initiation of XOLAIR therapy for asthma or CRSwNP. Decrease corticosteroids gradually under the direct supervision of a physician. In CSU patients, the use of XOLAIR in combination with corticosteroids has not been evaluated.
5.5 Eosinophilic Conditions
In rare cases, patients with asthma on therapy with XOLAIR may present with serious systemic eosinophilia sometimes presenting with clinical features of vasculitis consistent with Churg-Strauss syndrome, a condition which is often treated with systemic corticosteroid therapy. These events usually, but not always, have been associated with the reduction of oral corticosteroid therapy. Physicians should be alert to eosinophilia, vasculitic rash, worsening pulmonary symptoms, cardiac complications, and/or neuropathy presenting in their patients. A causal association between XOLAIR and these underlying conditions has not been established.
5.6 Fever, Arthralgia, and Rash
In post-approval use, some patients have experienced a constellation of signs and symptoms including arthritis/arthralgia, rash, fever, and lymphadenopathy with an onset 1 to 5 days after the first or subsequent injections of XOLAIR. These signs and symptoms have recurred after additional doses in some patients. Although circulating immune complexes or a skin biopsy consistent with a Type III reaction were not seen with these cases, these signs and symptoms are similar to those seen in patients with serum sickness. Physicians should stop XOLAIR if a patient develops this constellation of signs and symptoms [see Adverse Reactions (6.3)].
5.7 Parasitic (Helminth) Infection
Monitor patients at high risk of geohelminth infection while on XOLAIR therapy. Insufficient data are available to determine the length of monitoring required for geohelminth infections after stopping XOLAIR treatment.
In a one-year clinical trial conducted in Brazil in adult and adolescent patients at high risk for geohelminthic infections (roundworm, hookworm, whipworm, threadworm), 53% (36/68) of XOLAIR-treated patients experienced an infection, as diagnosed by standard stool examination, compared to 42% (29/69) of placebo controls. The point estimate of the odds ratio for infection was 1.96, with a 95% confidence interval (0.88, 4.36) indicating that in this study a patient who had an infection was anywhere from 0.88 to 4.36 times as likely to have received XOLAIR than a patient who did not have an infection. Response to appropriate anti-geohelminth treatment of infection as measured by stool egg counts was not different between treatment groups.
5.8 Laboratory Tests
Serum total IgE levels increase following administration of XOLAIR due to formation of XOLAIR:IgE complexes [see Clinical Pharmacology (12.2)]. Elevated serum total IgE levels may persist for up to 1 year following discontinuation of XOLAIR. Do not use serum total IgE levels obtained less than 1 year following discontinuation to reassess the dosing regimen for asthma or CRSwNP patients, because these levels may not reflect steady-state free IgE levels [see Dosage and Administration (2.2, 2.3)].
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions are described elsewhere in the labeling:
- Anaphylaxis [see Boxed Warning and Warnings and Precautions (5.1)]
- Malignancies [see Warnings and Precautions (5.2)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Adverse Reactions from Clinical Studies in Adult and Adolescent Patients 12 Years of Age and Older with Asthma
The data described below reflect XOLAIR exposure for 2076 adult and adolescent patients ages 12 and older, including 1687 patients exposed for six months and 555 exposed for one year or more, in either placebo-controlled or other controlled asthma studies. The mean age of patients receiving XOLAIR was 42 years, with 134 patients 65 years of age or older; 60% were women, and 85% Caucasian. Patients received XOLAIR 150 mg to 375 mg every 2 or 4 weeks or, for patients assigned to control groups, standard therapy with or without a placebo.
The adverse reactions most frequently resulting in clinical intervention (e.g., discontinuation of XOLAIR, or the need for concomitant medication to treat an adverse reaction) were injection site reaction (45%), viral infections (23%), upper respiratory tract infection (20%), sinusitis (16%), headache (15%), and pharyngitis (11%). These reactions were observed at similar rates in XOLAIR-treated patients and control patients.
Table 6 shows adverse reactions from four placebo-controlled asthma trials that occurred ≥1% and more frequently in adult and adolescent patients 12 years of age and older receiving XOLAIR than in those receiving placebo. Adverse reactions were classified using preferred terms from the International Medical Nomenclature (IMN) dictionary. Injection site reactions were recorded separately from the reporting of other adverse reactions.
| Adverse reaction | XOLAIR n=738 | Placebo n=717 |
|---|---|---|
| Body as a whole | ||
| Pain | 7% | 5% |
| Fatigue | 3% | 2% |
| Musculoskeletal system | ||
| Arthralgia | 8% | 6% |
| Fracture | 2% | 1% |
| Leg pain | 4% | 2% |
| Arm pain | 2% | 1% |
| Nervous system | ||
| Dizziness | 3% | 2% |
| Skin and appendages | ||
| Pruritus | 2% | 1% |
| Dermatitis | 2% | 1% |
| Special senses | ||
| Earache | 2% | 1% |
There were no differences in the incidence of adverse reactions based on age (among patients under 65), gender or race.
Adverse Reactions from Clinical Studies in Adult Patients with Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
The data described below reflect XOLAIR exposure for 135 patients ≥ 18 years of age, exposed for six months in two placebo-controlled studies. The mean age of patients receiving XOLAIR was 49.7 years; 64% were male, and 94% were Caucasian. Patients received XOLAIR or placebo SC every 2 or 4 weeks, with dosage and frequency according to Table 3. All patients received background nasal mometasone therapy throughout the study. Table 7 lists the adverse reactions occurring in ≥3% of XOLAIR-treated patients and more frequently than in patients treated with placebo in CRSwNP Trials 1 and 2; results were pooled.
| Adverse reaction | XOLAIR n=135 | Placebo n=130 |
|---|---|---|
| CRSwNP = Chronic Rhinosinusitis with Nasal Polyps. | ||
|
||
| Gastrointestinal disorder | ||
| Upper abdominal pain | 4 (3.0%) | 1 (0.8%) |
| General disorders and administration site conditions | ||
| Injection site reactions* | 7 (5.2%) | 2 (1.5%) |
| Musculoskeletal system and connective tissue disorders | ||
| Arthralgia | 4 (3.0%) | 2 (1.5%) |
| Nervous system disorders | ||
| Headache | 11 (8.1%) | 7 (5.4%) |
| Dizziness | 4 (3.0%) | 1 (0.8%) |
Adverse Reactions from Clinical Studies in Patients with Chronic Spontaneous Urticaria (CSU)
The safety of XOLAIR for the treatment of CSU was assessed in three placebo-controlled, multiple-dose clinical trials of 12 weeks' (CSU Trial 2) and 24 weeks' duration (CSU Trials 1 and 3). In CSU Trials 1 and 2, patients received XOLAIR 75 mg, 150 mg, or 300 mg or placebo every 4 weeks in addition to their baseline level of H1 antihistamine therapy throughout the treatment period. In CSU Trial 3 patients were randomized to XOLAIR 300 mg or placebo every 4 weeks in addition to their baseline level of H1 antihistamine therapy. The data described below reflect XOLAIR exposure for 733 patients enrolled and receiving at least one dose of XOLAIR in the three clinical trials, including 684 patients exposed for 12 weeks and 427 exposed for 24 weeks. The mean age of patients receiving XOLAIR 300 mg was 43 years, 75% were women, and 89% were white. The demographic profiles for patients receiving XOLAIR 150 mg and 75 mg were similar.
Table 8 shows adverse reactions that occurred in ≥2% of patients receiving XOLAIR (150 or 300 mg) and more frequently than those receiving placebo. Adverse reactions are pooled from Trial 2 and the first 12 weeks of Trials 1 and 3.
| Adverse Reactions* | CSU Trials 1, 2 and 3 Pooled | ||
|---|---|---|---|
| 150mg (n=175) | 300mg (n=412) | Placebo (n=242) |
|
|
|||
| Gastrointestinal disorders | |||
| Nausea | 2 (1.1%) | 11 (2.7%) | 6 (2.5%) |
| Infections and infestations | |||
| Nasopharyngitis | 16 (9.1%) | 27 (6.6%) | 17 (7.0%) |
| Sinusitis | 2 (1.1%) | 20 (4.9%) | 5 (2.1%) |
| Upper respiratory tract infection | 2 (1.1%) | 14 (3.4%) | 5 (2.1%) |
| Viral upper respiratory tract infection | 4 (2.3%) | 2 (0.5%) | (0.0%) |
| Musculoskeletal and connective tissue disorders | |||
| Arthralgia | 5 (2.9%) | 12 (2.9%) | 1 (0.4%) |
| Nervous system disorders | |||
| Headache | 21 (12.0%) | 25 (6.1%) | 7 (2.9%) |
| Respiratory, thoracic, and mediastinal disorders | |||
| Cough | 2 (1.1%) | 9 (2.2%) | 3 (1.2%) |
Additional reactions reported during the 24-week treatment period in Trials 1 and 3 [≥2% of patients receiving XOLAIR (150 mg or 300 mg) and more frequently than those receiving placebo] included: toothache, fungal infection, urinary tract infection, myalgia, pain in extremity, musculoskeletal pain, peripheral edema, pyrexia, migraine, sinus headache, anxiety, oropharyngeal pain, asthma, urticaria, and alopecia.
6.2 Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to omalizumab in the studies described below with the incidence of antibodies in other studies or to other products may be misleading.
Antibodies to XOLAIR were detected in approximately 1/1723 (<0.1%) of patients treated with XOLAIR in the clinical studies evaluated for asthma in patients 12 years of age and older. In three pediatric studies, antibodies to XOLAIR were detected in one patient out of 581 patients 6 to <12 years of age treated with XOLAIR and evaluated for antibodies. There were no detectable antibodies in the patients treated in the CSU clinical trials, but due to levels of XOLAIR at the time of anti-therapeutic antibody sampling and missing samples for some patients, antibodies to XOLAIR could only have been determined in 88% of the 733 patients treated in these clinical studies. The data reflect the percentage of patients whose test results were considered positive for antibodies to XOLAIR in ELISA assays and are highly dependent on the sensitivity and specificity of the assays.
6.3 Postmarketing Experience
The following adverse reactions have been identified during post-approval use of XOLAIR in adult and adolescent patients 12 years of age and older. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
7. Drug Interactions
No formal drug interaction studies have been performed with XOLAIR.
In patients with asthma and CRSwNP, the concomitant use of XOLAIR and allergen immunotherapy has not been evaluated.
In patients with CSU, the use of XOLAIR in combination with immunosuppressive therapies has not been studied.
8. Use In Specific Populations
8.5 Geriatric Use
In clinical studies, 134 asthma patients, 20 CRSwNP patients, and 37 CSU phase 3 study patients 65 years of age or older were treated with XOLAIR. Although there were no apparent age-related differences observed in these studies, the number of patients aged 65 and over is not sufficient to determine whether they respond differently from younger patients.
11. Xolair Description
Omalizumab is a recombinant DNA-derived humanized IgG1κ monoclonal antibody that selectively binds to human immunoglobulin E (IgE). The antibody has a molecular weight of approximately 149 kiloDaltons. XOLAIR is produced by a Chinese hamster ovary cell suspension culture.
XOLAIR (omalizumab) is administered as a subcutaneous (SC) injection and is available in prefilled syringes and in vials.
12. Xolair - Clinical Pharmacology
12.3 Pharmacokinetics
After SC administration, omalizumab was absorbed with an average absolute bioavailability of 62%. Following a single SC dose in adult and adolescent patients with asthma, omalizumab was absorbed slowly, reaching peak serum concentrations after an average of 7–8 days. In patients with CSU, the peak serum concentration was reached at a similar time after a single SC dose. The pharmacokinetics of omalizumab was linear at doses greater than 0.5 mg/kg. In patients with asthma, following multiple doses of XOLAIR, areas under the serum concentration-time curve from Day 0 to Day 14 at steady state were up to 6-fold of those after the first dose. In patients with CSU, omalizumab exhibited linear pharmacokinetics across the dose range of 75 mg to 600 mg given as single subcutaneous dose. Following repeat dosing from 75 to 300 mg every 4 weeks, trough serum concentrations of omalizumab increased proportionally with the dose levels.
In vitro, omalizumab formed complexes of limited size with IgE. Precipitating complexes and complexes larger than 1 million daltons in molecular weight were not observed in vitro or in vivo. Tissue distribution studies in Cynomolgus monkeys showed no specific uptake of 125I-omalizumab by any organ or tissue. The apparent volume of distribution of omalizumab in patients with asthma following SC administration was 78 ± 32 mL/kg. In patients with CSU, based on population pharmacokinetics, distribution of omalizumab was similar to that in patients with asthma.
Clearance of omalizumab involved IgG clearance processes as well as clearance via specific binding and complex formation with its target ligand, IgE. Liver elimination of IgG included degradation in the liver reticuloendothelial system (RES) and endothelial cells. Intact IgG was also excreted in bile. In studies with mice and monkeys, omalizumab:IgE complexes were eliminated by interactions with Fcγ receptors within the RES at rates that were generally faster than IgG clearance. In asthma patients omalizumab serum elimination half-life averaged 26 days, with apparent clearance averaging 2.4 ± 1.1 mL/kg/day. Doubling body weight approximately doubled apparent clearance. In CSU patients, at steady state, based on population pharmacokinetics, omalizumab serum elimination half-life averaged 24 days and apparent clearance averaged 240 mL/day (corresponding to 3.0 mL/kg/day for an 80 kg patient).
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term studies have been performed in animals to evaluate the carcinogenic potential of XOLAIR.
There were no effects on fertility and reproductive performance in male and female Cynomolgus monkeys that received XOLAIR at subcutaneous doses up to 75 mg/kg/week (approximately 5 times the maximum recommended human dose on a mg/kg basis).
14. Clinical Studies
14.1 Asthma
Adult and Adolescent Patients 12 Years of Age and Older
The safety and efficacy of XOLAIR were evaluated in three randomized, double-blind, placebo-controlled, multicenter trials.
The trials enrolled patients 12 to 76 years old, with moderate to severe persistent (NHLBI criteria) asthma for at least one year, and a positive skin test reaction to a perennial aeroallergen. In all trials, XOLAIR dosing was based on body weight and baseline serum total IgE concentration. All patients were required to have a baseline IgE between 30 and 700 IU/mL and body weight not more than 150 kg. Patients were treated according to a dosing table to administer at least 0.016 mg/kg/IU (IgE/mL) of XOLAIR or a matching volume of placebo over each 4-week period. The maximum XOLAIR dose per 4 weeks was 750 mg.
In all three trials an exacerbation was defined as a worsening of asthma that required treatment with systemic corticosteroids or a doubling of the baseline ICS dose. Most exacerbations were managed in the outpatient setting and the majority were treated with systemic steroids. Hospitalization rates were not significantly different between XOLAIR and placebo-treated patients; however, the overall hospitalization rate was small. Among those patients who experienced an exacerbation, the distribution of exacerbation severity was similar between treatment groups.
Asthma Trials 1 and 2
At screening, patients in Asthma Trials 1 and 2 had a forced expiratory volume in one second (FEV1) between 40% and 80% predicted. All patients had a FEV1 improvement of at least 12% following beta2-agonist administration. All patients were symptomatic and were being treated with inhaled corticosteroids (ICS) and short-acting beta2-agonists. Patients receiving other concomitant controller medications were excluded, and initiation of additional controller medications while on study was prohibited. Patients currently smoking were excluded.
Each trial was comprised of a run-in period to achieve a stable conversion to a common ICS (beclomethasone dipropionate), followed by randomization to XOLAIR or placebo. Patients received XOLAIR for 16 weeks with an unchanged corticosteroid dose unless an acute exacerbation necessitated an increase. Patients then entered an ICS reduction phase of 12 weeks during which ICS dose reduction was attempted in a step-wise manner.
The distribution of the number of asthma exacerbations per patient in each group during a study was analyzed separately for the stable steroid and steroid-reduction periods.
In both Asthma Trials 1 and 2 the number of exacerbations per patient was reduced in patients treated with XOLAIR compared with placebo (Table 9).
Measures of airflow (FEV1) and asthma symptoms were also evaluated in these trials. The clinical relevance of the treatment-associated differences is unknown. Results from the stable steroid phase Asthma Trial 1 are shown in Table 10. Results from the stable steroid phase of Asthma Trial 2 and the steroid reduction phases of both Asthma Trials 1 and 2 were similar to those presented in Table 10.
| Stable Steroid Phase (16 wks) | ||||
| Asthma Trial 1 | Asthma Trial 2 | |||
| Exacerbations per patient | XOLAIR N=268 | Placebo N=257 | XOLAIR N=274 | Placebo N=272 |
| 0 | 85.8% | 76.7% | 87.6% | 69.9% |
| 1 | 11.9% | 16.7% | 11.3% | 25.0% |
| ≥2 | 2.2% | 6.6% | 1.1% | 5.1% |
| p-Value | 0.005 | <0.001 | ||
| Mean number exacerbations/patient | 0.2 | 0.3 | 0.1 | 0.4 |
| Steroid Reduction Phase (12 wks) | ||||
| Exacerbations per patient | XOLAIR N=268 | Placebo N=257 | XOLAIR N=274 | Placebo N=272 |
| 0 | 78.7% | 67.7% | 83.9% | 70.2% |
| 1 | 19.0% | 28.4% | 14.2% | 26.1% |
| ≥2 | 2.2% | 3.9% | 1.8% | 3.7% |
| p-Value | 0.004 | <0.001 | ||
| Mean number exacerbations/patient | 0.2 | 0.4 | 0.2 | 0.3 |
| XOLAIR N=268* | Placebo N=257* |
|||
|---|---|---|---|---|
| Endpoint | Mean Baseline | Median Change (Baseline to Wk 16) | Mean Baseline | Median Change (Baseline to Wk 16) |
| Asthma symptom scale: total score from 0 (least) to 9 (most); nocturnal and daytime scores from 0 (least) to 4 (most symptoms). | ||||
|
||||
| Total asthma symptom score | 4.3 | –1.5† | 4.2 | –1.1† |
| Nocturnal asthma score | 1.2 | –0.4† | 1.1 | –0.2† |
| Daytime asthma score | 2.3 | –0.9† | 2.3 | –0.6† |
| FEV1 % predicted | 68 | 3† | 68 | 0† |
Asthma Trial 3
In Asthma Trial 3, there was no restriction on screening FEV1, and unlike Asthma Trials 1 and 2, long-acting beta2-agonists were allowed. Patients were receiving at least 1000 µg/day fluticasone propionate and a subset was also receiving oral corticosteroids. Patients receiving other concomitant controller medications were excluded, and initiation of additional controller medications while on study was prohibited. Patients currently smoking were excluded.
The trial was comprised of a run-in period to achieve a stable conversion to a common ICS (fluticasone propionate), followed by randomization to XOLAIR or placebo. Patients were stratified by use of ICS-only or ICS with concomitant use of oral steroids. Patients received XOLAIR for 16 weeks with an unchanged corticosteroid dose unless an acute exacerbation necessitated an increase. Patients then entered an ICS reduction phase of 16 weeks during which ICS or oral steroid dose reduction was attempted in a step-wise manner.
The number of exacerbations in patients treated with XOLAIR was similar to that in placebo-treated patients (Table 11). The absence of an observed treatment effect may be related to differences in the patient population compared with Asthma Trials 1 and 2, study sample size, or other factors.
| Stable Steroid Phase (16 wks) | ||||
| Inhaled Only | Oral + Inhaled | |||
| XOLAIR N=126 | Placebo N=120 | XOLAIR N=50 | Placebo N=45 |
|
| % Patients with ≥1 exacerbations | 15.9% | 15.0% | 32.0% | 22.2% |
| Difference (95% CI) | 0.9 (–9.7, 13.7) | 9.8 (–10.5, 31.4) |
||
| Steroid Reduction Phase (16 wks) | ||||
| XOLAIR N=126 | Placebo N=120 | XOLAIR N=50 | Placebo N=45 |
|
| % Patients with ≥1 exacerbations | 22.2% | 26.7% | 42.0% | 42.2% |
| Difference (95% CI) | –4.4 (–17.6, 7.4) | –0.2 (–22.4, 20.1) |
||
In all three of the trials, a reduction of asthma exacerbations was not observed in the XOLAIR-treated patients who had FEV1>80% at the time of randomization. Reductions in exacerbations were not seen in patients who required oral steroids as maintenance therapy.
14.2 Chronic Rhinosinusitis with Nasal Polyps (CRSwNP)
Adult Patients 18 Years of Age and Older
The safety and efficacy of XOLAIR was evaluated in two, randomized, multicenter, double-blind, placebo-controlled clinical trials that enrolled patients with CRSwNP with inadequate response to nasal corticosteroids (CRSwNP Trial 1, n=138; CRSwNP Trial 2, n=127). Patients received XOLAIR or placebo SC every 2 or 4 weeks, with XOLAIR dosage and frequency according to Table 3, for 24 weeks followed by a 4-week follow-up period. All patients received background nasal mometasone therapy during both the treatment period and during a 5-week run-in period. Prior to randomization, patients were required to have evidence of bilateral polyps as determined by a nasal polyp score (NPS) ≥ 5 with NPS ≥ 2 in each nostril, despite use of nasal mometasone during the run-in period. NPS was measured via endoscopy and scored (range 0-4 per nostril: 0= no polyps; 1=small polyps in the middle meatus not reaching below the inferior border of the middle turbinate; 2=polyps reaching below the lower border of the middle turbinate; 3=large polyps reaching the lower border of the inferior turbinate or polyps medial to the middle turbinate; 4=large polyps causing complete obstruction of the inferior nasal cavity) for a total NPS (range 0-8). Patients were furthermore required to have a weekly average of nasal congestion score (NCS) > 1 prior to randomization, despite use of nasal mometasone. Nasal congestion was measured by a daily assessment on a 0 to 3 point severity scale (0=none, 1=mild, 2=moderate, 3=severe). Prior sino-nasal surgery or prior systemic corticosteroid usage were not required for inclusion in the trials and sinus CT scans were not performed to evaluate for sinus opacification. Demographics and baseline characteristics, including allergic comorbidities, are described in Table 12.
| Parameter | CRSwNP Trial 1 (n=138) | CRSwNP Trial 2 (n=127) |
|---|---|---|
| CRSwNP= chronic rhinosinusitis with nasal polyps; SD=standard deviation; NPS=nasal polyp score; IgE = Immunoglobulin E; IU=international units. For NPS, NCS, sense of smell, post nasal drip, and runny nose, higher scores indicate greater disease severity. | ||
| Mean age (years) (SD) | 51 (13) | 50 (12) |
| % Male | 64 | 65 |
| Patients with systemic corticosteroid use in the previous year (%) | 19 | 26 |
| Patients with prior surgery for nasal polyps (%) | 79 (57) | 79 (62) |
| Mean bilateral endoscopic NPS (SD), range 0-8 | 6.2 (1.0) | 6.3 (0.9) |
| Mean nasal congestion score (SD) range 0-3 | 2.4 (0.6) | 2.3 (0.7) |
| Mean sense of smell score (SD) range 0-3 | 2.7 (0.7) | 2.7 (0.7) |
| Mean post nasal drip score (SD) range 0-3 | 1.8 (0.9) | 1.7 (0.9) |
| Mean runny nose score (SD) range 0-3 | 2.0 (0.8) | 1.9 (0.9) |
| Mean blood eosinophils (cells/mcL) (SD) | 346 (284) | 335 (188) |
| Mean total IgE IU/mL (SD) | 161 (140) | 190 (201) |
| Asthma (%) | 54 | 61 |
| Aspirin exacerbated respiratory disease (%) | 20 | 35 |
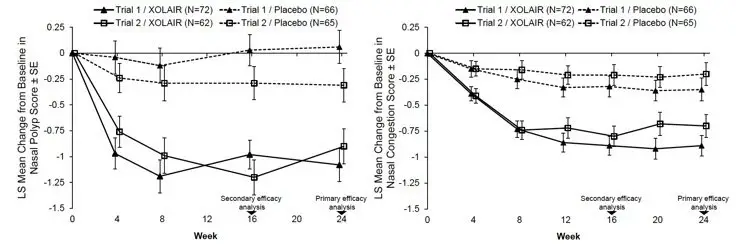
The co-primary endpoints in Trials 1 and 2 were NPS and average daily NCS at Week 24. In both trials, patients who received XOLAIR had a statistically significant greater improvement from baseline at Week 24 in NPS and weekly average NCS, than patients who received placebo. Results from CRSwNP Trials 1 and 2 are shown in Table 13.
The greater improvements in NPS and NCS in the XOLAIR group compared to the placebo group were observed as early as the first assessment at Week 4 in both studies, as seen in Figure 1.
| Trial 1 | Trial 2 | |||
|---|---|---|---|---|
| Placebo | XOLAIR | Placebo | XOLAIR | |
| CRSwNP= chronic rhinosinusitis with nasal polyps; LS=least-square. Change from baseline was analyzed using a mixed-effect model of repeated measures (MMRM) model with baseline score, baseline score/timepoint (week) interaction as covariates, and the following factors: geographic region, asthma/aspirin sensitivity comorbidity status, timepoint, treatment group, treatment/timepoint interaction. | ||||
| Number of patients | 65 | 72 | 65 | 62 |
| Nasal Polyp Score | ||||
| Mean Baseline Score | 6.3 | 6.2 | 6.1 | 6.4 |
| LS Mean Change From Baseline at Week 24 | 0.1 | -1.1 | -0.3 | -0.9 |
| Difference in LS means vs. placebo | -1.1 | -0.6 | ||
| 95% CI for difference | -1.6, -0.7 | -1.1, -0.1 | ||
| p-value | <0.0001 | 0.0140 | ||
| 7-day Average of Daily Nasal Congestion Score | ||||
| Mean Baseline Score | 2.5 | 2.4 | 2.3 | 2.3 |
| LS Mean Change From Baseline at Week 24 | -0.4 | -0.9 | -0.2 | -0.7 |
| Difference in LS means vs. placebo | -0.6 | -0.5 | ||
| 95% CI for difference | -0.8, -0.3 | -0.8, -0.2 | ||
| p-value | 0.0004 | 0.0017 | ||
The mean NPS and NCS at each study week by treatment group is shown in Figure 1.
|
|
XOLAIR had statistically significant improvements on sense of smell score compared to placebo. Sense of smell was measured by a daily assessment on a 0 to 3 point severity scale (0=no symptoms, 1=mild symptoms, 2=moderate symptoms, 3=severe symptoms). The LS mean difference for change from baseline at Week 24 in sense of smell score in XOLAIR compared to placebo was -0.3 (95% CI: -0.6, -0.1) in Trial 1 and -0.5 (95% CI: -0.7, -0.2) in Trial 2.
XOLAIR had statistically significant improvements on post-nasal drip compared to placebo. The LS mean difference for change from baseline at Week 24 in post-nasal drip score in XOLAIR compared to placebo was -0.6 (95% CI: -0.8, -0.3) in Trial 1 and -0.5 (95% CI: -0.8, -0.3) in Trial 2.
XOLAIR had statistically significant improvements on runny nose compared to placebo. The LS mean difference for change from baseline at Week 24 in runny nose score in XOLAIR compared to placebo was -0.4 (95% CI: -0.7, -0.2) in Trial 1 and -0.6 (95% CI: -0.9, -0.4) in Trial 2.
In a pre-specified pooled analysis of systemic corticosteroid use during the 24-week treatment period, there was no significant reduction in systemic corticosteroid use between the treatment arms. The proportion of patients taking systemic corticosteroid in XOLAIR was 2.3% compared to 6.2% in placebo. The odds-ratio of systemic corticosteroid use with XOLAIR compared to placebo was 0.4 (95% CI: 0.1, 1.5).
There were no sino-nasal surgeries reported, in either placebo or XOLAIR arms, in either Trial.
14.3 Chronic Spontaneous Urticaria (CSU)
Adult and Adolescent Patients 12 Years of Age and Older
The safety and efficacy of XOLAIR for the treatment of CSU, previously referred to as chronic idiopathic urticaria (CIU) was assessed in two placebo-controlled, multiple-dose clinical trials of 24 weeks' duration (CSU Trial 1; n= 319) and 12 weeks' duration (CSU Trial 2; n=322). Patients received XOLAIR 75 mg, 150 mg, or 300 mg or placebo by SC injection every 4 weeks in addition to their baseline level of H1 antihistamine therapy for 24 or 12 weeks, followed by a 16-week washout observation period. A total of 640 patients (165 males, 475 females) were included for the efficacy analyses. Most patients were white (84%) and the median age was 42 years (range 12–72).
Disease severity was measured by a weekly urticaria activity score (UAS7, range 0–42), which is a composite of the weekly itch severity score (range 0–21) and the weekly hive count score (range 0–21). All patients were required to have a UAS7 of ≥16, and a weekly itch severity score of ≥8 for the 7 days prior to randomization, despite having used an H1 antihistamine for at least 2 weeks.
The mean weekly itch severity scores at baseline were fairly balanced across treatment groups and ranged between 13.7 and 14.5 despite use of an H1 antihistamine at an approved dose. The reported median durations of CSU at enrollment across treatment groups were between 2.5 and 3.9 years (with an overall subject-level range of 0.5 to 66.4 years).
In both CSU Trials 1 and 2, patients who received XOLAIR 150 mg or 300 mg had greater decreases from baseline in weekly itch severity scores and weekly hive count scores than placebo at Week 12. Representative results from CSU Trial 1 are shown (Table 14); similar results were observed in CSU Trial 2. The 75-mg dose did not demonstrate consistent evidence of efficacy and is not approved for use.
| XOLAIR 75mg | XOLAIR 150mg | XOLAIR 300mg | Placebo | |
|---|---|---|---|---|
|
||||
| n | 77 | 80 | 81 | 80 |
| Weekly Itch Severity Score | ||||
| Mean Baseline Score (SD) | 14.5 (3.6) | 14.1 (3.8) | 14.2 (3.3) | 14.4 (3.5) |
| Mean Change Week 12 (SD) | −6.46 (6.14) | −6.66 (6.28) | −9.40 (5.73) | −3.63 (5.22) |
| Difference in LS means vs. placebo | −2.96 | −2.95 | −5.80 | |
| 95% CI for difference | −4.71, −1.21 | −4.72, −1.18 | −7.49, −4.10 | - |
| Weekly Hive Count Score † | ||||
| Mean Baseline Score (SD) | 17.2 (4.2) | 16.2 (4.6) | 17.1 (3.8) | 16.7 (4.4) |
| Mean Change Week 12 (SD) | −7.36 (7.52) | −7.78 (7.08) | −11.35 (7.25) | −4.37 (6.60) |
| Difference in LS means vs. placebo | −2.75 | −3.44 | −6.93 | |
| 95% CI for difference | −4.95, −0.54 | −5.57, −1.32 | −9.10, −4.76 | - |
The mean weekly itch severity score at each study week by treatment groups is shown in Figure 2. Representative results from CSU Trial 1 are shown; similar results were observed in CSU Trial 2. The appropriate duration of therapy for CSU with XOLAIR has not been determined.
|
|

In CSU Trial 1, a larger proportion of patients treated with XOLAIR 300 mg (36%) reported no itch and no hives (UAS7=0) at Week 12 compared to patients treated with XOLAIR 150 mg (15%), XOLAIR 75 mg (12%), and placebo group (9%). Similar results were observed in CSU Trial 2.
16. How is Xolair supplied
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
| This Medication Guide has been approved by the U.S. Food and Drug Administration | Revised: 03/2023 | |
| MEDICATION GUIDE | ||
| XOLAIR® (ZOHL-air)
(omalizumab) injection, for subcutaneous use | XOLAIR® (ZOHL-air)
(omalizumab) for injection, for subcutaneous use |
|
| What is the most important information I should know about XOLAIR? XOLAIR may cause serious side effects, including: Severe allergic reaction. A severe allergic reaction called anaphylaxis can happen when you receive XOLAIR. The reaction can occur after the first dose, or after many doses. It may also occur right after a XOLAIR injection or days later. Anaphylaxis is a life-threatening condition and can lead to death. Go to the nearest emergency room right away if you have any of these symptoms of an allergic reaction:
|
||
| What is XOLAIR?
XOLAIR is an injectable prescription medicine used to treat:
|
||
| Who should not receive and use XOLAIR? Do not receive and use XOLAIR if you:
|
||
| What should I tell my healthcare provider before receiving XOLAIR? Before receiving XOLAIR, tell your healthcare provider about all of your medical conditions, including if you:
|
||
How should I receive and use XOLAIR?
|
||
| What are the possible side effects of XOLAIR? XOLAIR may cause serious side effects, including:
|
||
|
|
|
|
||
How should I store XOLAIR?
|
||
| General information about the safe and effective use of XOLAIR.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use XOLAIR for a condition for which it was not prescribed. Do not give XOLAIR to other people, even if they have the same symptoms that you have. It may harm them. You can ask your pharmacist or healthcare provider for information about XOLAIR that is written for health professionals. For more information, go to www.xolair.com or call 1-866-4XOLAIR (1-866-496-5247). |
||
| What are the ingredients in XOLAIR? Active ingredient: omalizumab Inactive ingredients: Prefilled syringe: L-arginine hydrochloride, L-histidine, L-histidine hydrochloride monohydrate, and polysorbate 20 Vial: L-histidine, L-histidine hydrochloride monohydrate, polysorbate 20 and sucrose Manufactured by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990. U.S. License No.: 1048 Jointly marketed by: Genentech USA, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 Novartis Pharmaceuticals Corporation, One Health Plaza, East Hanover, NJ 07936-1080 XOLAIR® is a registered trademark of Novartis AG. ©2023 Genentech USA, Inc. |
||
| Instructions for Use Xolair® (ZOHL-air) (omalizumab) Prefilled Syringe |
|
| Read this Instructions for Use before you start using the XOLAIR prefilled syringe and each time you get a refill. Before you use the XOLAIR prefilled syringe for the first time, make sure your healthcare provider shows you the right way to use it. Contact your healthcare provider if you have any questions. | |
|
|
|
Supplies needed to give your injection
| 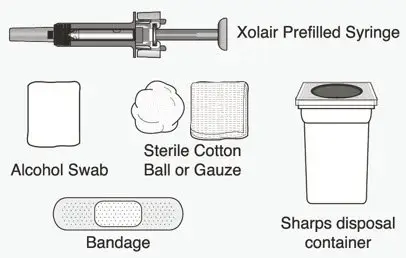 |
|
Choose the correct prefilled syringe or combination of prefilled syringes |
|
| XOLAIR prefilled syringes are available in 2 dose strengths. These instructions are to be used for both dose strengths. | |
| Your prescribed dose may require more than 1 injection. The table below shows the combination of prefilled syringes needed to give your full dose. Check the label on the XOLAIR carton to make sure you have received the correct prefilled syringe or combination of prefilled syringes for your prescribed dose. If your dose requires more than 1 injection, inject the medicine from all of your prescribed prefilled syringes, immediately one after another. Contact your healthcare provider if you have any questions. | |
|
|
|
|
|
|
How should I store XOLAIR?
|
|
Important Information
|
|
| Preparing for the Injection | |
| 1 Take the carton containing the prefilled syringe out of the refrigerator. | |
|
|
| 2 Check the expiration date on the XOLAIR carton. | |
|
|
|
| 3 Place the carton on a clean, flat surface. | |
|
|
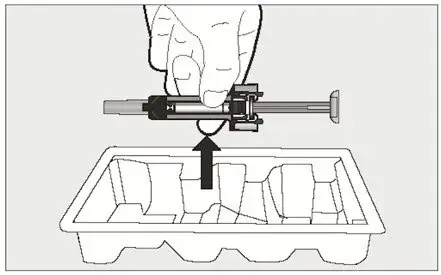
| 4 Open the carton. | |
|
|
|
|
|
|
|
|
 |
|
5 Inspect the prefilled syringe closely.
|
|
 |
|
| 6 Choose an injection site. | |
|
|
 |
|
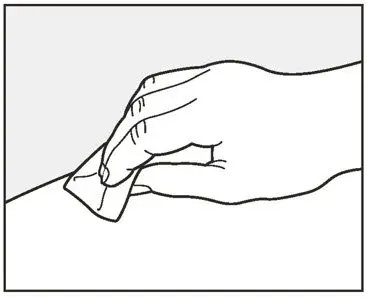
| 7 Wipe the injection site with an alcohol swab in a circular motion and let it air dry for 10 seconds. | |
|
|
 |
|
| Giving the Injection | |
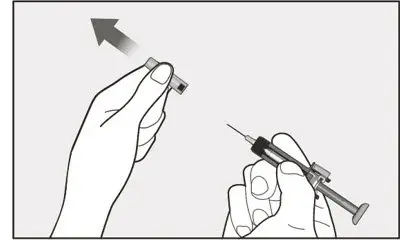
| 8 Hold the prefilled syringe firmly by the center with 1 hand and pull the needle cap straight off with your other hand. | |
|
|
|
|
|
| 9 Use your other hand and gently pinch the area of skin that was cleaned. Hold the pinched skin tight. | |
|
|
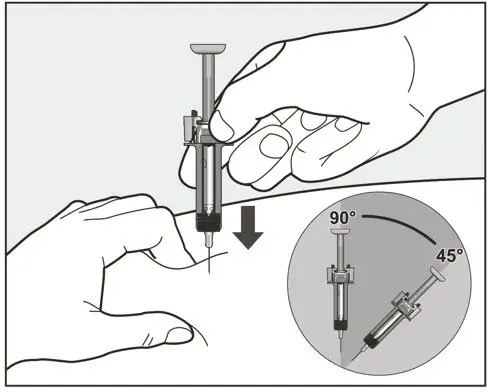
| 10 Continue holding the prefilled syringe by the center and use a quick, dart-like motion to insert the needle all the way into the pinched skin at an angle between 45 degrees to 90 degrees as shown. | |
 |
|
|
|
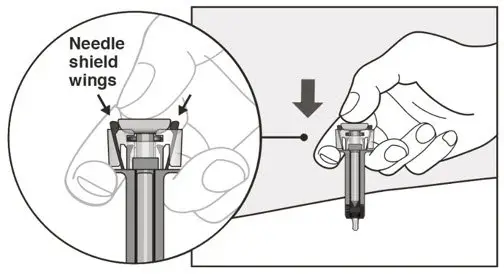
| 11 Slowly inject all of the medicine by gently pushing the plunger all the way down until the needle-shield wings are pushed apart. | |
|
|
 |
|
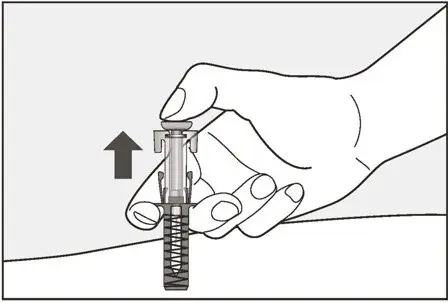
| 12 Release the plunger and allow the needle to be covered by the needle-shield. | |
|
|
 |
|
| 13 There may be a little bleeding at the injection site. You can press a cotton ball or gauze over the injection site. | |
|
|
| If your prescribed dose requires more than 1 injection: | |
|
|
| After the Injection | |
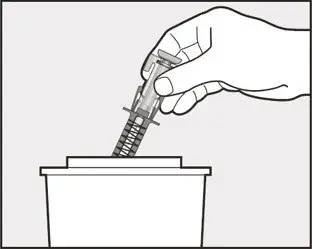
|
|
| If you do not have an FDA-cleared sharps disposal container, you may use a household container that is: | |
|
|
| Manufactured by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 U.S. License No.: 1048 |
|
| Jointly marketed by: Genentech USA, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 Novartis Pharmaceuticals Corporation, One Health Plaza, East Hanover, NJ 07936-1080 |
|
| XOLAIR® is a registered trademark of Novartis AG. ©2021 Genentech USA, Inc. |
|
| This Instructions for Use has been approved by the U.S. Food and Drug Administration. | |
| Approved: 07/ 2021 | |

| XOLAIR
omalizumab injection, solution |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| XOLAIR PFS
omalizumab injection, solution |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| XOLAIR PFS
omalizumab injection, solution |
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||
| Labeler - Genentech, Inc. (080129000) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genentech, Inc. | 080129000 | ANALYSIS(50242-040, 50242-214, 50242-215) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genentech, Inc. | 146373191 | ANALYSIS(50242-040, 50242-214, 50242-215) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Roche Diagnostics GmbH | 323105205 | ANALYSIS(50242-040, 50242-214, 50242-215) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Roche Singapore Technical Operations Pte. Ltd | 937189173 | ANALYSIS(50242-040, 50242-214, 50242-215) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genentech, Inc. | 004074162 | ANALYSIS(50242-040, 50242-214, 50242-215) , API MANUFACTURE(50242-040, 50242-214, 50242-215) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Genentech, Inc. | 833220176 | PACK(50242-040) , LABEL(50242-040) , ANALYSIS(50242-040) | |
