Drug Detail:Zerbaxa (Ceftolozane and tazobactam [ sef-tol-oh-zane-and-taz-oh-bak-tam ])
Drug Class: Cephalosporins / beta-lactamase inhibitors
Highlights of Prescribing Information
ZERBAXA® (ceftolozane and tazobactam) for injection, for intravenous use
Initial U.S. Approval: 2014
Recent Major Changes
| Indications and Usage (1) | 4/2022 |
| Dosage and Administration (2) | 4/2022 |
Indications and Usage for Zerbaxa
ZERBAXA (ceftolozane and tazobactam) is a combination of ceftolozane, a cephalosporin antibacterial, and tazobactam, a beta-lactamase inhibitor, indicated for the treatment of the following infections caused by designated susceptible microorganisms:
- Complicated Intra-abdominal Infections (cIAI), used in combination with metronidazole, in adult and pediatric patients (birth to less than 18 years old). (1.1)
- Complicated Urinary Tract Infections (cUTI), Including Pyelonephritis, in adult and pediatric patients (birth to less than 18 years old). (1.2)
- Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP), in adult patients 18 years and older. (1.3)
To reduce the development of drug-resistant bacteria and maintain the effectiveness of ZERBAXA and other antibacterial drugs, ZERBAXA should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. (1.4)
Zerbaxa Dosage and Administration
- Administer all doses of ZERBAXA every 8 hours by intravenous infusion over 1 hour in adult and pediatric patients. (2.1, 2.2)
- See Full Prescribing Information for instructions on the preparation of solutions. (2.3)
- For doses above 1.5 g, reconstitute a second vial in the same manner as the first one, withdraw an appropriate volume (per Table 4 in the Full Prescribing Information), and add to the same infusion bag. (2.3)
| Infection | Dose | Duration of Treatment |
|---|---|---|
|
||
| Complicated Intra-abdominal Infections (cIAI)* | 1.5 g | 4 to 14 days |
| Complicated Urinary Tract Infections (cUTI), Including Pyelonephritis | 1.5 g | 7 days |
| Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP) | 3 g | 8 to 14 days |
| Infection | Dose | Duration of Treatment |
|---|---|---|
|
||
| Complicated Intra-abdominal Infections† | 30 mg/kg up to a maximum dose of 1.5 g ‡ | 5 to 14 days |
| Complicated Urinary Tract Infections, including Pyelonephritis | 30 mg/kg up to a maximum dose of 1.5 g ‡ | 7 to 14 days |
| Estimated CrCl (mL/min) * | cIAI and cUTI, including pyelonephritis | HABP/VABP |
|---|---|---|
|
||
| 30 to 50 | ZERBAXA 750 mg (500 mg and 250 mg) intravenously every 8 hours | ZERBAXA 1.5 g (1 g and 0.5 g) intravenously every 8 hours |
| 15 to 29 | ZERBAXA 375 mg (250 mg and 125 mg) intravenously every 8 hours | ZERBAXA 750 mg (500 mg and 250 mg) intravenously every 8 hours |
| End-stage renal disease (ESRD) on hemodialysis (HD) | A single loading dose of ZERBAXA 750 mg (500 mg and 250 mg) followed by a ZERBAXA 150 mg (100 mg and 50 mg) maintenance dose administered intravenously every 8 hours for the remainder of the treatment period (on hemodialysis days, administer the dose at the earliest possible time following completion of dialysis) | A single loading dose of ZERBAXA 2.25 g (1.5 g and 0.75 g) followed by a ZERBAXA 450 mg (300 mg and 150 mg) maintenance dose administered intravenously every 8 hours for the remainder of the treatment period (on hemodialysis days, administer the dose at the earliest possible time following completion of dialysis) |
Dosage Forms and Strengths
- ZERBAXA 1.5 g (ceftolozane and tazobactam) for injection supplied as a sterile powder for reconstitution in single-dose vials containing ceftolozane 1 g (equivalent to 1.147 g ceftolozane sulfate) and tazobactam 0.5 g (equivalent to 0.537 g tazobactam sodium). (3)
Contraindications
- ZERBAXA is contraindicated in patients with known serious hypersensitivity to the components of ZERBAXA (ceftolozane and tazobactam), piperacillin/tazobactam, or other members of the beta-lactam class. (4)
Warnings and Precautions
- Decreased efficacy was observed in a Phase 3 cIAI trial in a subgroup of patients with baseline CrCl of 30 to 50 mL/min. Monitor CrCl at least daily in patients with changing renal function and adjust the dose of ZERBAXA accordingly. (5.1)
- Serious hypersensitivity (anaphylactic) reactions have been reported with beta-lactam antibacterial drugs. Exercise caution in patients with known hypersensitivity to beta-lactam antibacterial drugs. If an anaphylactic reaction to ZERBAXA occurs, discontinue the drug and institute appropriate therapy. (5.2)
- Clostridioides difficile-associated diarrhea (CDAD) has been reported with nearly all systemic antibacterial agents, including ZERBAXA. Evaluate if diarrhea occurs. (5.3)
Adverse Reactions/Side Effects
-
Adult cIAI, cUTI and HAB/VABP Patients:
- The most common adverse reactions in adult patients (≥5% in either the cIAI or cUTI indication) are nausea, diarrhea, headache, and pyrexia. (6.1).
- The most common adverse reactions (≥5% in the HABP/VABP indication) are increase in hepatic transaminases, renal impairment/renal failure, and diarrhea. (6.1)
- Pediatric cIAI and cUTI Patients: The most common adverse reactions in pediatric patients (≥7% in either the cIAI or cUTI indication) are thrombocytosis, diarrhea, pyrexia, leukopenia, abdominal pain, vomiting, increased aspartate aminotransferase, and anemia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Merck Sharp & Dohme LLC at 1-877-888-4231 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch .
Use In Specific Populations
- Pediatrics: Safety and effectiveness in pediatric patients with HABP/VABP have not been established. (8.4)
- Geriatrics: Higher incidence of adverse reactions was observed in patients aged 65 years and older. In a Phase 3 cIAI trial, cure rates were lower in patients 65 years and older. (8.5)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 5/2022
Full Prescribing Information
1. Indications and Usage for Zerbaxa
1.1 Complicated Intra-abdominal Infections
ZERBAXA used in combination with metronidazole is indicated for the treatment of adult and pediatric patients (birth to less than 18 years old) with complicated intra-abdominal infections (cIAI) caused by the following susceptible Gram-negative and Gram-positive microorganisms: Enterobacter cloacae, Escherichia coli, Klebsiella oxytoca, Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa, Bacteroides fragilis, Streptococcus anginosus, Streptococcus constellatus, and Streptococcus salivarius.
1.2 Complicated Urinary Tract Infections, Including Pyelonephritis
ZERBAXA is indicated for the treatment of adult and pediatric patients (birth to less than 18 years old) with complicated urinary tract infections (cUTI), including pyelonephritis, caused by the following susceptible Gram-negative microorganisms: Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa.
1.3 Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP)
ZERBAXA is indicated for the treatment of adult patients (18 years and older) with hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia (HABP/VABP), caused by the following susceptible Gram-negative microorganisms: Enterobacter cloacae, Escherichia coli, Haemophilus influenzae, Klebsiella oxytoca, Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa, and Serratia marcescens.
1.4 Usage
To reduce the development of drug-resistant bacteria and maintain the effectiveness of ZERBAXA and other antibacterial drugs, ZERBAXA should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
2. Zerbaxa Dosage and Administration
2.1 Recommended Dosage in Adult Patients
The recommended dosage of ZERBAXA in adult patients 18 years and older with creatinine clearance (CrCl) greater than 50 mL/min is 1.5 gram (g) (ceftolozane 1 g and tazobactam 0.5 g for cIAI and cUTI and 3 g (ceftolozane 2 g and tazobactam 1 g) for HABP/VABP administered every 8 hours by intravenous infusion over 1 hour The duration of therapy should be guided by the severity and site of infection and the patient’s clinical and bacteriological progress as shown in Table 1.
| Infection | Dose | Frequency | Infusion Time | Duration of Treatment |
|---|---|---|---|---|
|
||||
| Complicated Intra-abdominal Infections† | 1.5 g | Every 8 Hours | 1 hour | 4 to 14 days |
| Complicated Urinary Tract Infections, Including Pyelonephritis | 1.5 g | Every 8 Hours | 1 hour | 7 days |
| Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP) | 3 g | Every 8 Hours | 1 hour | 8 to 14 days |
2.2 Recommended Dosage in Pediatric Patients with cIAI or cUTI (birth to less than 18 years of age)
The recommended dosage regimen of ZERBAXA in pediatric patients from birth to less than 18 years of age with cIAI and cUTI with an estimated glomerular filtration rate (eGFR) greater than 50 mL/min/1.73 m2 is described in Table 2. ZERBAXA is administered every 8 hours by intravenous infusion over 1 hour. The duration of treatment should be guided by the severity and site of infection and the patient’s clinical and bacteriological progress as shown in Table 2. For the treatment of cIAI, metronidazole should be given concurrently.
ZERBAXA is not recommended in pediatric patients who have an eGFR 50 mL/min/1.73m2 or less [see Use in Specific Populations (8.4)].
There is insufficient information to recommend a dosage regimen for pediatric patients with HABP/VABP [see Use in Specific Populations (8.4)].
| Infection | Dose | Frequency | Infusion time | Duration of treatment |
|---|---|---|---|---|
|
||||
| Complicated Intra-abdominal Infections† | 30 mg/kg up to a maximum dose of 1.5 g‡ | Every 8 hours | 1 hour | 5 to 14 days |
| Complicated Urinary Tract Infections including Pyelonephritis | 30 mg/kg up to a maximum dose of 1.5 g‡ | Every 8 hours | 1 hour | 7 to 14 days |
2.3 Dosage Adjustments in Adult Patients with Renal Impairment
Dose adjustment is required for adult patients (18 years and older) with CrCl 50 mL/min or less (Table 3). All doses of ZERBAXA are administered over 1 hour. For patients with changing renal function, monitor CrCl at least daily and adjust the dosage of ZERBAXA accordingly [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].
|
Estimated CrCl (mL/min)* | Complicated Intra-abdominal Infections and Complicated Urinary Tract Infections, Including Pyelonephritis | Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP) |
|---|---|---|
|
||
| 30 to 50 | 750 mg (500 mg and 250 mg) intravenously every 8 hours | 1.5 g (1 g and 0.5 g) intravenously every 8 hours |
| 15 to 29 | 375 mg (250 mg and 125 mg) intravenously every 8 hours | 750 mg (500 mg and 250 mg) intravenously every 8 hours |
| End-stage renal disease (ESRD) on hemodialysis (HD) | A single loading dose of 750 mg (500 mg and 250 mg) followed by a 150 mg (100 mg and 50 mg) maintenance dose administered intravenously every 8 hours for the remainder of the treatment period (on hemodialysis days, administer the dose at the earliest possible time following completion of dialysis) | A single loading dose of 2.25 g (1.5 g and 0.75 g) followed by a 450 mg (300 mg and 150 mg) maintenance dose administered intravenously every 8 hours for the remainder of the treatment period (on hemodialysis days, administer the dose at the earliest possible time following completion of dialysis) |
2.4 Dosage Adjustments in Pediatric Patients with Renal Impairment
Dosage adjustment of ZERBAXA in pediatric patients (birth to less than 18 years of age) with eGFR 50 mL/min/1.73 m2 or less has not been determined.
ZERBAXA is not recommended in pediatric patients who have an eGFR 50 mL/min/1.73m2 or less [see Use in Specific Populations (8.4)].
2.5 Preparation of Solutions
ZERBAXA does not contain a bacteriostatic preservative. Aseptic technique must be followed in preparing the infusion solution.
2.6 Compatibility
Compatibility of ZERBAXA with other drugs has not been established. ZERBAXA should not be mixed with other drugs or physically added to solutions containing other drugs.
2.7 Storage of Constituted Solutions
Upon constitution with sterile water for injection or 0.9% sodium chloride injection, reconstituted ZERBAXA solution may be held for 1 hour prior to transfer and dilution in a suitable infusion bag.
Following dilution of the solution with 0.9% sodium chloride or 5% dextrose, ZERBAXA is stable for 24 hours when stored at room temperature or 7 days when stored under refrigeration at 2 to 8°C (36 to 46°F). Discard unused portion.
Constituted ZERBAXA solution or diluted ZERBAXA infusion should not be frozen.
3. Dosage Forms and Strengths
ZERBAXA 1.5 g (ceftolozane and tazobactam) for injection is supplied as a white to yellow sterile powder for reconstitution in single-dose vials; each vial contains ceftolozane 1 g (equivalent to 1.147 g of ceftolozane sulfate) and tazobactam 0.5 g (equivalent to 0.537 g of tazobactam sodium).
4. Contraindications
ZERBAXA is contraindicated in patients with known serious hypersensitivity to the components of ZERBAXA (ceftolozane and tazobactam), piperacillin/tazobactam, or other members of the beta-lactam class.
5. Warnings and Precautions
5.1 Decreased Efficacy in Patients with Baseline Creatinine Clearance of 30 to 50 mL/min
In a subgroup analysis of a Phase 3 cIAI trial of adult patients, clinical cure rates were lower in patients with baseline CrCl of 30 to 50 mL/min compared to those with CrCl greater than 50 mL/min (Table 5). The reduction in clinical cure rates was more marked in the ZERBAXA plus metronidazole arm compared to the meropenem arm. A similar trend was also seen in the cUTI trial. Monitor CrCl at least daily in patients with changing renal function and adjust the dosage of ZERBAXA accordingly [see Dosage and Administration (2.2)].
| Baseline Renal Function | ZERBAXA plus Metronidazole n/N (%) | Meropenem n/N (%) |
|---|---|---|
| CrCl greater than 50 mL/min | 312/366 (85.2) | 355/404 (87.9) |
| CrCl 30 to 50 mL/min | 11/23 (47.8) | 9/13 (69.2) |
5.2 Hypersensitivity Reactions
Serious and occasionally fatal hypersensitivity (anaphylactic) reactions have been reported in patients receiving beta-lactam antibacterial drugs.
Before initiating therapy with ZERBAXA, make careful inquiry about previous hypersensitivity reactions to other cephalosporins, penicillins, or other beta-lactams. If this product is to be given to a patient with a cephalosporin, penicillin, or other beta-lactam allergy, exercise caution because cross sensitivity has been established. If an anaphylactic reaction to ZERBAXA occurs, discontinue the drug and institute appropriate therapy.
5.3 Clostridioides difficile-associated Diarrhea
Clostridioides difficile-associated diarrhea (CDAD) has been reported for nearly all systemic antibacterial agents, including ZERBAXA, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. CDAD must be considered in all patients who present with diarrhea following antibacterial use. Careful medical history is necessary because CDAD has been reported to occur more than 2 months after the administration of antibacterial agents.
If CDAD is confirmed, discontinue antibacterials not directed against C. difficile, if possible. Manage fluid and electrolyte levels as appropriate, supplement protein intake, monitor antibacterial treatment of C. difficile, and institute surgical evaluation as clinically indicated.
6. Adverse Reactions/Side Effects
The following serious reactions are described in greater detail in the Warnings and Precautions section:
- Hypersensitivity reactions [see Warnings and Precautions (5.2)]
- Clostridioides difficile-associated diarrhea [see Warnings and Precautions (5.3)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and also may not reflect rates observed in practice.
8. Use In Specific Populations
8.4 Pediatric Use
Complicated Intra-abdominal Infections (cIAI) and Complicated Urinary Tract Infections (cUTI), including Pyelonephritis
The safety and effectiveness of ZERBAXA for the treatment of cIAI and cUTI have been established in pediatric patients aged birth to less than 18 years old. Use of ZERBAXA in these age groups is supported by evidence from adequate and well-controlled studies of ZERBAXA in adults with cUTI and cIAI and additional pharmacokinetic and safety data from pediatric trials [see Clinical Pharmacology (12.3) and Clinical Studies (14.1 and 14.2)].
The safety profile of ZERBAXA in pediatric patients was similar to adults with cIAI and cUTI, treated with ZERBAXA [see Adverse Reactions (6.1)].
There is insufficient information to recommend dosage adjustment for pediatric patients younger than 18 years of age with cIAI and cUTI with eGFR 50 mL/min/1.73m2 or less [see Dosage and Administration (2.4) and Clinical Pharmacology (12.3)].
ZERBAXA is not recommended in pediatric patients who have an eGFR 50 mL/min/1.73m2 or less. Pediatric patients born at term or pre-term may not have an eGFR of 50 mL/min/1.73m2 or greater at birth or within the first few months of life.
Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP)
The safety and effectiveness of ZERBAXA in pediatric patients have not been established for the treatment of HABP and VABP.
8.5 Geriatric Use
Of the 1015 patients treated with ZERBAXA in the Phase 3 cIAI and cUTI clinical trials, 250 (24.6%) were 65 years or older, including 113 (11.1%) 75 years or older. The incidence of adverse events in both treatment groups was higher in older subjects (65 years or older) in the trials for both indications. In the cIAI trial, cure rates in the elderly (aged 65 years and older) in the ZERBAXA plus metronidazole arm were 69/100 (69%) and in the comparator arm were 70/85 (82.4%). This finding in the elderly population was not observed in the cUTI trial.
Of the 361 patients treated with ZERBAXA in the Phase 3 HABP/VABP clinical trial, 160 (44.3%) were 65 years or older, including 83 (23%) 75 years or older. The incidence of adverse events in both treatment groups was higher in older subjects (65 years or older). In the trial, Day 28 all-cause mortality rates in the elderly (aged 65 years and older) were comparable between treatment arms:50/160 (31.3%) in the ZERBAXA arm and 54/160 (33.8%) in the comparator arm.
ZERBAXA is substantially excreted by the kidney and the risk of adverse reactions to ZERBAXA may be greater in patients with renal impairment. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function. Adjust dosage for elderly patients based on renal function [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)].
8.6 Patients with Renal Impairment
Adult Patients
Dosage adjustment is required in adult patients with CrCl 50 mL/min or less, including adult patients with ESRD on HD [see Dosage and Administration (2.2), Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)].
Pediatric Patients
No dose adjustment has been established in pediatric patients aged birth to less than 18 years of age with eGFR 50 mL/min/1.73 m2 or less [see Clinical Pharmacology (12.3)].
10. Overdosage
In the event of overdose, discontinue ZERBAXA and provide general supportive treatment. ZERBAXA can be removed by hemodialysis. Approximately 66% of ceftolozane, 56% of tazobactam, and 51% of the tazobactam metabolite M1 were removed by dialysis. No information is available on the use of hemodialysis to treat overdosage.
11. Zerbaxa Description
ZERBAXA (ceftolozane and tazobactam) is an antibacterial combination product consisting of the cephalosporin antibacterial drug ceftolozane sulfate and the beta-lactamase inhibitor tazobactam sodium for intravenous administration.
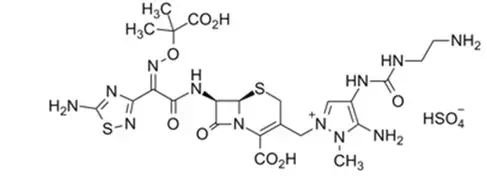
Ceftolozane sulfate is a semi-synthetic antibacterial drug of the beta-lactam class for parenteral administration. The chemical name of ceftolozane sulfate is 1H-Pyrazolium, 5-amino-4-[[[(2-aminoethyl)amino]carbonyl]amino]-2-[[(6R,7R)-7-[[(2Z)-2-(5-amino-1,2,4-thiadiazol-3-yl)-2-[(1-carboxy-1-methylethoxy)imino]acetyl]amino]-2-carboxy-8-oxo-5-thia-1-azabicyclo[4.2.0]oct-2-en-3-yl]methyl]-1-methyl-,sulfate (1:1). The molecular formula is C23H31N12O8S2+∙HSO4- and the molecular weight is 764.77.
Figure 1: Chemical structure of ceftolozane sulfate
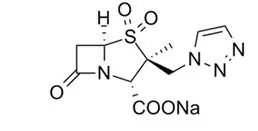
Tazobactam sodium, a derivative of the penicillin nucleus, is a penicillanic acid sulfone. Its chemical name is sodium (2S,3S,5R)-3-methyl-7-oxo-3-(1H-1,2,3-triazol-1-ylmethyl)-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylate-4,4-dioxide. The chemical formula is C10H11N4NaO5S and the molecular weight is 322.3.
Figure 2: Chemical structure of tazobactam sodium
ZERBAXA 1.5 g (ceftolozane and tazobactam) for injection is a white to yellow sterile powder for reconstitution consisting of ceftolozane 1 g (equivalent to 1.147 g of ceftolozane sulfate) and tazobactam 0.5 g (equivalent to 0.537 g of tazobactam sodium) per vial, packaged in single-dose glass vials. The product contains sodium chloride (487 mg/vial) as a stabilizing agent, citric acid (21 mg/vial), and L-arginine (approximately 600 mg/vial) as excipients.
12. Zerbaxa - Clinical Pharmacology
12.2 Pharmacodynamics
As with other beta-lactam antibacterial agents, the percent time of dosing interval that the plasma concentration of ceftolozane exceeds the minimum inhibitory concentration (MIC) of the infecting organism has been shown to be the best predictor of efficacy in animal models of infection. The percent time of dosing interval that the plasma concentration of tazobactam exceeds a threshold concentration has been determined to be the parameter that best predicts the efficacy of tazobactam in in vitro and in vivo models. The exposure-response analyses in efficacy and safety clinical trials for cIAI, cUTI, and HABP/VABP support the recommended dose regimens of ZERBAXA.
12.3 Pharmacokinetics
Ceftolozane and tazobactam pharmacokinetics are similar following single- and multiple-dose administrations. The Cmax and AUC of ceftolozane and tazobactam increase in proportion to dose.
The mean steady-state population pharmacokinetic parameters of ZERBAXA in patients with cIAI and cUTI receiving 1-hour intravenous infusions of ZERBAXA 1.5 g (ceftolozane 1 g and tazobactam 0.5 g) or patients with HABP/VABP receiving 1-hour intravenous infusions of ZERBAXA 3 g (ceftolozane 2 g and tazobactam 1 g) every 8 hours are summarized in Table 9.
| PK parameters | ZERBAXA 1.5 g (ceftolozane 1 g and tazobactam 0.5 g) in cIAI and cUTI Patients | ZERBAXA 3 g (ceftolozane 2 g and tazobactam 1 g) in HABP/VABP Patients | ||
|---|---|---|---|---|
| Ceftolozane (n=317) | Tazobactam (n=244) | Ceftolozane (n=247) | Tazobactam (n=247) |
|
| Cmax (mcg/mL) | 65.7 (27) | 17.8 (9) | 105 (46) | 26.4 (13) |
| AUC0-8,ss (mcg∙h/mL) | 186 (74) | 35.8 (57) | 392 (236) | 73.3 (76) |
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term carcinogenicity studies in animals have not been conducted with ZERBAXA, ceftolozane, or tazobactam.
ZERBAXA was negative for genotoxicity in an in vitro mouse lymphoma assay and an in vivo rat bone-marrow micronucleus assay. In an in vitro chromosomal aberration assay in Chinese hamster ovary cells, ZERBAXA was positive for structural aberrations.
Ceftolozane was negative for genotoxicity in an in vitro microbial mutagenicity (Ames) assay, an in vitro chromosomal aberration assay in Chinese hamster lung fibroblast cells, an in vitro mouse lymphoma assay, an in vitro HPRT assay in Chinese hamster ovary cells, an in vivo mouse micronucleus assay, and an in vivo unscheduled DNA synthesis (UDS) assay.
Tazobactam was negative for genotoxicity in an in vitro microbial mutagenicity (Ames) assay, an in vitro chromosomal aberration assay in Chinese hamster lung cells, an in vitro mammalian point-mutation (Chinese hamster ovary cell HPRT) assay, an in vivo mouse bone-marrow micronucleus assay, and an in vivo UDS assay.
Ceftolozane was administered in a fertility study at intravenous doses of 100, 300, and 1000 mg/kg/day to male rats for 28 days before mating and through the mating period and to female rats for 14 days before mating, through the mating period, and until the 7th day of gestation. Ceftolozane had no adverse effect on fertility in male or female rats at doses up to 1000 mg/kg/day (approximately 1.4 times the maximum recommended human dose (MRHD) of 2 grams every 8 hours based on AUC comparison).
In a rat fertility study, intraperitoneal tazobactam doses of 40, 160, and 640 mg/kg/day were administered twice-daily to male rats beginning 70 days before mating and through the mating period, and to female rats beginning 14 days before mating, during the mating period, and until Gestation Day 21. Male and female fertility parameters were not affected at doses less than or equal to 640 mg/kg/day (approximately 2 times the MRHD of 1 gram every 8 hours based on body surface comparison).
14. Clinical Studies
14.1 Complicated Intra-abdominal Infections
Adult Patients
A total of 979 adults hospitalized with cIAI were randomized and received study medications in a multinational, double-blind study comparing ZERBAXA 1.5 g (ceftolozane 1 g and tazobactam 0.5 g) intravenously every 8 hours plus metronidazole (500 mg intravenously every 8 hours) to meropenem (1 g intravenously every 8 hours) for 4 to 14 days of therapy. Complicated intra-abdominal infections included appendicitis, cholecystitis, diverticulitis, gastric/duodenal perforation, perforation of the intestine, and other causes of intra-abdominal abscesses and peritonitis. The majority of patients (75%) were from Eastern Europe; 6.3% were from the United States.
The primary efficacy endpoint was clinical response, defined as complete resolution or significant improvement in signs and symptoms of the index infection at the test-of-cure (TOC) visit which occurred 24 to 32 days after the first dose of study drug. The primary efficacy analysis population was the microbiological intent-to-treat (MITT) population, which included all patients who had at least 1 baseline intra-abdominal pathogen regardless of the susceptibility to study drug. The key secondary efficacy endpoint was clinical response at the TOC visit in the microbiologically evaluable (ME) population, which included all protocol-adherent MITT patients.
The MITT population consisted of 806 patients; the median age was 52 years and 57.8% were male. The most common diagnosis was appendiceal perforation or peri-appendiceal abscess, occurring in 47% of patients. Diffuse peritonitis at baseline was present in 34.2% of patients.
ZERBAXA plus metronidazole was non-inferior to meropenem with regard to clinical cure rates at the TOC visit in the MITT population. Clinical cure rates at the TOC visit are displayed by patient population in Table 12. Clinical cure rates at the TOC visit by pathogen in the MITT population are presented in Table 13.
| Analysis Population | ZERBAXA plus Metronidazole*
n/N (%) | Meropenem†
n/N (%) | Treatment Difference (95% CI)‡ |
|---|---|---|---|
|
|||
|
MITT | 323/389 (83) | 364/417 (87.3) | -4.3 (-9.2, 0.7) |
| ME | 259/275 (94.2) | 304/321 (94.7) | -0.5 (-4.5, 3.2) |
| Organism Group Pathogen | ZERBAXA plus Metronidazole n/N (%) | Meropenem n/N (%) |
|---|---|---|
| Aerobic Gram-negative | ||
| Escherichia coli | 216/255 (84.7) | 238/270 (88.1) |
| Klebsiella pneumoniae | 31/41 (75.6) | 27/35 (77.1) |
| Pseudomonas aeruginosa | 30/38 (79) | 30/34 (88.2) |
| Enterobacter cloacae | 21/26 (80.8) | 24/25 (96) |
| Klebsiella oxytoca | 14/16 (87.5) | 24/25 (96) |
| Proteus mirabilis | 11/12 (91.7) | 9/10 (90) |
| Aerobic Gram-positive | ||
| Streptococcus anginosus | 26/36 (72.2) | 24/27 (88.9) |
| Streptococcus constellatus | 18/24 (75) | 20/25 (80) |
| Streptococcus salivarius | 9/11 (81.8) | 9/11 (81.8) |
| Anaerobic Gram-negative | ||
| Bacteroides fragilis | 42/47 (89.4) | 59/64 (92.2) |
| Bacteroides ovatus | 38/45 (84.4) | 44/46 (95.7) |
| Bacteroides thetaiotaomicron | 21/25 (84) | 40/46 (87) |
| Bacteroides vulgatus | 12/15 (80) | 24/26 (92.3) |
In a subset of the E. coli and K. pneumoniae isolates from both arms of the cIAI Phase 3 trial that met pre-specified criteria for beta-lactam susceptibility, genotypic testing identified certain ESBL groups (e.g., TEM, SHV, CTX-M, OXA) in 53/601 (9%). Cure rates in this subset were similar to the overall trial results. In vitro susceptibility testing showed that some of these isolates were susceptible to ZERBAXA (MIC ≤2 mcg/mL), while some others were not susceptible (MIC >2 mcg/mL). Isolates of a specific genotype were seen in patients who were deemed to be either successes or failures.
Pediatric Patients
The pediatric cIAI trial was a randomized, double-blind, multi-center, active controlled trial conducted in hospitalized patients from birth to less than 18 years (NCT03217136). Patients were randomized in a 3:1 ratio to either intravenous (IV) ZERBAXA [see Dosage and Administration (2.2)] plus metronidazole (10 mg/kg IV every 8 hours), or meropenem (20 mg/kg IV every 8 hours) plus placebo. Patients received IV study treatment for a minimum of 3 days before an optional switch to oral step-down therapy at the discretion of the investigator to complete a total of 5 to 14 days of antibacterial therapy.
The modified intent-to-treat (MITT) population consisted of 91 patients (N=70 in the ZERBAXA plus metronidazole group; N=21 in the meropenem plus placebo group) who were randomized and received at least one dose of study treatment. The median age of patients was 8.2 years and 8.5 years in the ZERBAXA plus metronidazole and meropenem plus placebo groups, respectively. In the ZERBAXA plus metronidazole group, enrollment by age group was as follows: 12 to <18 y: n=16, 6 to <12 y: n=30, 2 to <6 y: n=22, 3 months to <2 y: n=1, birth to <3 months: n=1. Patients treated with ZERBAXA plus metronidazole were predominantly male (67%) and White (87%). Patients treated with meropenem plus placebo were predominantly female (71%) and White (91%). Most patients in the MITT population had a diagnosis of complicated appendicitis at baseline (ZERBAXA plus metronidazole: 91.4%; meropenem plus placebo: 100%). The median (range) duration of IV study treatment was comparable between patients in the ZERBAXA plus metronidazole (6.3 [0.3 to 14.0] days) and meropenem plus placebo (6.0 [2.3 to 8.8] days) groups.
The primary objective of the study was to evaluate the safety and tolerability of ZERBAXA. Efficacy assessments were not powered for formal hypothesis testing of between-treatment group comparisons. At the TOC visit, which occurred 7 to 14 days after the last dose of study drug, a favorable clinical response was defined as complete resolution or marked improvement in signs and symptoms of the cIAI or return to pre-infection signs and symptoms such that no further antibiotic therapy (IV or oral) or surgical or drainage procedure was required for treatment of the cIAI. A summary of clinical response rates in the MITT and clinically evaluable (CE) populations at the TOC visit are presented in Table 14. The CE included all protocol adherent MITT patients with a clinical outcome at the visit of interest.
| Analysis Population | ZERBAXA plus metronidazole n/N (%) | Meropenem n/N (%) | Treatment Difference (95% CI)* |
|---|---|---|---|
|
|||
| MITT Population | 56/70 (80.0) | 21/21 (100.0) | -19.1 (-30.2, -2.9) |
| CE Population | 52/58 (89.7) | 19/19 (100.0) | -10.7 (-21.5, 6.8) |
14.2 Complicated Urinary Tract Infections, Including Pyelonephritis
Adult Patients
A total of 1068 adults hospitalized with cUTI (including pyelonephritis) were randomized and received study medications in a multinational, double-blind study comparing ZERBAXA 1.5 g (ceftolozane 1 g and tazobactam 0.5 g) intravenously every 8 hours to levofloxacin (750 mg intravenously once daily) for 7 days of therapy. The primary efficacy endpoint was defined as complete resolution or marked improvement of the clinical symptoms and microbiological eradication (all uropathogens found at baseline at ≥105 were reduced to <104 CFU/mL) at the test-of-cure (TOC) visit 7 (± 2) days after the last dose of study drug. The primary efficacy analysis population was the microbiologically modified intent-to-treat (mMITT) population, which included all patients who received study medication and had at least 1 baseline uropathogen. The key secondary efficacy endpoint was the composite microbiological and clinical cure response at the TOC visit in the microbiologically evaluable (ME) population, which included protocol-adherent mMITT patients with a urine culture at the TOC visit.
The mMITT population consisted of 800 patients with cUTI, including 656 (82%) with pyelonephritis. The median age was 50.5 years and 74% were female. Concomitant bacteremia was identified in 62 (7.8%) patients at baseline; 608 (76%) patients were enrolled in Eastern Europe and 14 (1.8%) patients were enrolled in the United States.
ZERBAXA demonstrated efficacy with regard to the composite endpoint of microbiological and clinical cure at the TOC visit in both the mMITT and ME populations (Table 15). Composite microbiological and clinical cure rates at the TOC visit by pathogen in the mMITT population are presented in Table 16.
In the mMITT population, the composite cure rate in ZERBAXA-treated patients with concurrent bacteremia at baseline was 23/29 (79.3%).
Although a statistically significant difference was observed in the ZERBAXA arm compared to the levofloxacin arm with respect to the primary endpoint, it was likely attributable to the 212/800 (26.5%) patients with baseline organisms non-susceptible to levofloxacin. Among patients infected with a levofloxacin-susceptible organism at baseline, the response rates were similar (Table 15).
| Analysis Population | ZERBAXA*
n/N (%) | Levofloxacin†
n/N (%) | Treatment Difference (95% CI)‡ |
|---|---|---|---|
|
|||
| mMITT | 306/398 (76.9) | 275/402 (68.4) | 8.5 (2.3, 14.6) |
| Levofloxacin resistant baseline pathogen(s) | 60/100 (60) | 44/112 (39.3) | |
| No levofloxacin resistant baseline pathogen(s) | 246/298 (82.6) | 231/290 (79.7) | |
| ME | 284/341 (83.3) | 266/353 (75.4) | 8.0 (2.0, 14.0) |
| Pathogen | ZERBAXA n/N (%) | Levofloxacin n/N (%) |
|---|---|---|
| Escherichia coli | 247/305 (81) | 228/324 (70.4) |
| Klebsiella pneumoniae | 22/33 (66.7) | 12/25 (48) |
| Proteus mirabilis | 11/12 (91.7) | 6/12 (50) |
| Pseudomonas aeruginosa | 6/8 (75) | 7/15 (46.7) |
In a subset of the E. coli and K. pneumoniae isolates from both arms of the cUTI Phase 3 trial that met pre-specified criteria for beta-lactam susceptibility, genotypic testing identified certain ESBL groups (e.g., TEM, SHV, CTX-M, OXA) in 104/687 (15%). Cure rates in this subset were similar to the overall trial results. In vitro susceptibility testing showed that some of these isolates were susceptible to ZERBAXA (MIC ≤2 mcg/mL), while some others were not susceptible (MIC >2 mcg/mL). Isolates of a specific genotype were seen in patients who were deemed to be either successes or failures.
Pediatric Patients
The cUTI pediatric trial was a randomized, double-blind multi-center, active controlled trial conducted in hospitalized patients from birth to less than 18 years (NCT03230838). Eligible patients were randomized in a 3:1 ratio to IV ZERBAXA or meropenem, respectively. Patients received IV study treatment for a minimum of 3 days before an optional switch to oral step-down therapy at the discretion of the investigator to complete a total of 7 to 14 days of antibacterial therapy.
The microbiologic modified intent-to-treat (mMITT) population consisted of 95 patients (N=71 in the ZERBAXA group; N=24 in the meropenem group) who were randomized and received at least one dose of study treatment and had an eligible uropathogen isolated from a baseline urine culture.
The median age of patients was 2.7 years and 1.6 years in the ZERBAXA and meropenem groups, respectively. In the ZERBAXA group, enrollment by age group was as follows: 12 to <18 y: n=10, 6 to <12 y: n=13, 2 to <6 y: n=14, 3 months to <2 y: n=20, birth to <3 months: n=14. Patients treated with ZERBAXA were predominantly female (56%) and White (99%). Patients treated with meropenem were predominantly female (63%) and White (100%). Most patients in the mMITT population had a diagnosis of pyelonephritis (ZERBAXA: 84.5%; meropenem: 79.2%). The most common baseline qualifying gram-negative uropathogens were Escherichia coli (ZERBAXA: 74.6%; meropenem: 87.5%), Klebsiella pneumoniae (8.5%; 4.2%), and Pseudomonas aeruginosa (7.0%; 8.3%).
The primary objective of the study was to evaluate the safety and tolerability of ZERBAXA. Efficacy assessments were not powered for formal hypothesis testing of between treatment group comparisons. At the TOC visit, which occurred 7 to 14 days after the last dose of study drug, a favorable clinical response was defined as complete resolution or marked improvement in signs and symptoms of the cUTI or return to pre-infection signs and symptoms, such that no further antibiotic therapy (IV or oral) was required for the treatment of the cUTI. A favorable microbiological response at the TOC was defined as eradication (all uropathogens found at baseline at ≥105 were reduced to <104 CFU/mL) of baseline uropathogens from the urine culture. A summary of clinical and microbiologic response rates in the mMITT population at the TOC visit is presented in Table 17.
| mMITT Population | ZERBAXA n/N (%) | Meropenem n/N (%) | Treatment Difference (95% CI)* |
|---|---|---|---|
|
|||
| Clinical Response Rate | 63/71 (88.7) | 23/24 (95.8) | -7.3 (-18.0, 10.1) |
| Microbiologic Response Rate | 60/71 (84.5) | 21/24 (87.5) | -3.0 (-17.1, 17.4) |
14.3 Hospital-acquired Bacterial Pneumonia and Ventilator-associated Bacterial Pneumonia (HABP/VABP)
Adult Patients
A total of 726 adult patients hospitalized with HABP/VABP were enrolled in a multinational, double-blind study (NCT02070757) comparing ZERBAXA 3 g (ceftolozane 2 g and tazobactam 1 g) intravenously every 8 hours to meropenem (1 g intravenously every 8 hours) for 8 to 14 days of therapy. All patients had to be intubated and on mechanical ventilation at randomization.
Efficacy was assessed based on all-cause mortality at Day 28 and clinical cure, defined as complete resolution or significant improvement in signs and symptoms of the index infection at the test-of-cure (TOC) visit which occurred 7 to 14 days after the end of treatment. The analysis population was the intent-to-treat (ITT) population, which included all randomized patients.
Following a diagnosis of HABP/VABP and prior to receipt of first dose of study drug, if required, patients could have received up to a maximum of 24 hours of active non-study antibacterial drug therapy in the 72 hours preceding the first dose of study drug. Patients who had failed prior antibacterial drug therapy for the current episode of HABP/VABP could be enrolled if the baseline lower respiratory tract (LRT) culture showed growth of a Gram-negative pathogen while the patient was on the antibacterial therapy and all other eligibility criteria were met. Empiric therapy at baseline with linezolid or other approved therapy for Gram-positive coverage was required in all patients pending baseline LRT culture results. Adjunctive Gram-negative therapy was optional and allowed for a maximum of 72 hours in centers with a prevalence of meropenem-resistant P. aeruginosa more than 15%.
Of the 726 patients in the ITT population, the median age was 62 years and 44% of the population was 65 years of age and older, with 22% of the population 75 years of age and older. The majority of patients were White (83%), male (71%) and were from Eastern Europe (64%). The median APACHE II score was 17 and 33% of subjects had a baseline APACHE II score of greater than or equal to 20. All subjects were on mechanical ventilation and 519 (71%) had VABP. At randomization, 92% of subjects were in the ICU, 77% had been hospitalized for 5 days or longer, and 49% were ventilated for 5 days or longer. A total of 258 of 726 (36%) patients had CrCl less than 80 mL/min at baseline; among these, 99 (14%) had CrCl less than 50 mL/min. Patients with end-stage renal disease (CrCl less than 15 mL/min) were excluded from the trial. Approximately 13% of subjects were failing their current antibacterial drug therapy for HABP/VABP, and bacteremia was present at baseline in 15% of patients. Key comorbidities included diabetes mellitus, congestive heart failure, and chronic obstructive pulmonary disease at rates of 22%, 16%, and 12%, respectively. In both treatment groups, most subjects (63.1%) received between 8 and 14 days of study therapy as specified in the protocol.
Table 18 presents the results for Day 28 all-cause mortality and clinical cure at the TOC visit overall and by ventilated HABP and VABP.
| Endpoint | ZERBAXA n/N (%) | Meropenem n/N (%) | Treatment Difference (95% CI)* |
|---|---|---|---|
|
|||
| Day 28 All-cause Mortality | 87/362 (24.0) | 92/364 (25.3) | 1.1 (-5.13, 7.39) |
| VABP | 63/263 (24.0) | 52/256 (20.3) | -3.6 (-10.74, 3.52) |
| Ventilated HABP | 24/99 (24.2) | 40/108 (37.0) | 12.8 (0.18, 24.75) |
| Clinical Cure at TOC Visit | 197/362 (54.4) | 194/364 (53.3) | 1.1 (-6.17, 8.29) |
| VABP | 147/263 (55.9) | 146/256 (57.0) | -1.1 (-9.59, 7.35) |
| Ventilated HABP | 50/99 (50.5) | 48/108 (44.4) | 6.1 (-7.44, 19.27) |
In the ITT population, Day 28 all-cause mortality and clinical cure rates in patients with CrCl greater than or equal to 150 mL/min were similar between ZERBAXA and meropenem. In patients with bacteremia at baseline, Day 28 all-cause mortality rates were 23/64 (35.9%) for ZERBAXA-treated patients and 13/41 (31.7%) for meropenem-treated patients; clinical cure rates were 30/64 (46.9%) and 15/41 (36.6%), respectively.
Per pathogen Day 28 all-cause mortality and clinical cure at TOC were assessed in the microbiologic intention to treat population (mITT), which consisted of all randomized subjects who had a baseline lower respiratory tract (LRT) pathogen that was susceptible to both study treatments. In the mITT population, Klebsiella pneumoniae (113/425, 26.6%) and Pseudomonas aeruginosa (103/425, 24.2%) were the most prevalent pathogens isolated from baseline LRT cultures.
Day 28 all-cause mortality and clinical cure rates at TOC by pathogen in the mITT population are presented in Table 19. In the mITT population, clinical cure rates in patients with a Gram-negative pathogen at baseline were 139/215 (64.7%) for ZERBAXA and 115/204 (56.4%) for meropenem, respectively.
| Baseline Pathogen Category | Day 28 All-cause Mortality | Clinical Cure at TOC | ||
|---|---|---|---|---|
| Baseline Pathogen | ZERBAXA n/N (%) | Meropenem n/N (%) | ZERBAXA n/N (%) | Meropenem n/N (%) |
| Pseudomonas aeruginosa | 12/47 (25.5) | 10/56 (17.9) | 29/47 (61.7) | 34/56 (60.7) |
| Enterobacteriaceae | 27/161 (16.8) | 42/157 (26.8) | 103/161 (64.0) | 87/157 (55.4) |
| Enterobacter cloacae | 2/15 (13.3) | 8/14 (57.1) | 8/15 (53.3) | 4/14 (28.6) |
| Escherichia coli | 10/50 (20.0) | 11/42 (26.2) | 32/50 (64.0) | 26/42 (61.9) |
| Klebsiella oxytoca | 3/14 (21.4) | 3/12 (25.0) | 9/14 (64.3) | 7/12 (58.3) |
| Klebsiella pneumoniae | 7/51 (13.7) | 13/62 (21.0) | 34/51 (66.7) | 39/62 (62.9) |
| Proteus mirabilis | 5/22 (22.7) | 5/18 (27.8) | 13/22 (59.1) | 11/18 (61.1) |
| Serratia marcescens | 3/14 (21.4) | 1/12 (8.3) | 8/14 (57.1) | 7/12 (58.3) |
| Haemophilus influenzae | 0/20 (0) | 2/15 (13.3) | 17/20 (85.0) | 8/15 (53.3) |
In a subset of Enterobacteriaceae isolates from both arms of the trial that met pre-specified criteria for beta-lactam susceptibility, genotypic testing identified certain ESBL groups (e.g., TEM, SHV, CTX-M, OXA) in 101/425 (23.8%). Day 28 all-cause mortality and clinical cure rates in this subset were similar to the overall trial results.
16. How is Zerbaxa supplied
16.1 How Supplied
ZERBAXA 1.5 g (ceftolozane and tazobactam) for injection is supplied in single-dose vials containing ceftolozane 1 g (equivalent to 1.147 g of ceftolozane sulfate) and tazobactam 0.5 g (equivalent to 0.537 g of tazobactam sodium) per vial. Vials are supplied in cartons containing 10 vials.
(NDC 67919-030-01)
| ZERBAXA
ceftolozane and tazobactam injection, powder, lyophilized, for solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Merck Sharp & Dohme LLC (118446553) |
| Registrant - CUBIST PHARMACEUTICALS LLC (808394928) |
