Drug Detail:Calquence (Acalabrutinib [ a-kal-a-broo-ti-nib ])
Drug Class: BTK inhibitors
Highlights of Prescribing Information
CALQUENCE® (acalabrutinib) capsules, for oral use
Initial U.S. Approval: 2017
Indications and Usage for Calquence
CALQUENCE is a kinase inhibitor indicated for the treatment of adult patients with:
- •
- Mantle cell lymphoma (MCL) who have received at least one prior therapy. (1.1)
This indication is approved under accelerated approval based on overall response rate. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. (1.1, 14.1) - •
- Chronic lymphocytic leukemia (CLL) or small lymphocytic lymphoma (SLL). (1.2)
Calquence Dosage and Administration
- •
- Recommended dose is 100 mg orally approximately every 12 hours; swallow whole with water and with or without food. (2.1)
- •
- Advise patients not to break, open, or chew capsules. (2.1)
- •
- Manage toxicities using treatment interruption, dose reduction, or discontinuation. (2.2)
- •
- Avoid CALQUENCE in patients with severe hepatic impairment (2.2, 8.6)
Dosage Forms and Strengths
Capsules: 100 mg. (3)
Contraindications
None. (4)
Warnings and Precautions
- •
- Serious and Opportunistic Infections: Monitor for signs and symptoms of infection and treat promptly. (5.1)
- •
- Hemorrhage: Monitor for bleeding and manage appropriately. (5.2)
- •
- Cytopenias: Monitor complete blood counts regularly. (5.3)
- •
- Second Primary Malignancies: Other malignancies have occurred, including skin cancers and other solid tumors. Advise patients to use sun protection. (5.4)
- •
- Atrial Fibrillation and Flutter: Monitor for symptoms of arrhythmias and manage. (5.5)
Adverse Reactions/Side Effects
Most common adverse reactions (incidence ≥ 30%) were: anemia, neutropenia, upper respiratory tract infection, thrombocytopenia, headache, diarrhea, and musculoskeletal pain. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca at 1-800-236-9933 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- •
- CYP3A Inhibitors: Avoid co-administration with strong CYP3A inhibitors. Dose adjustments may be recommended. (2.3, 7, 12.3)
- •
- CYP3A Inducers: Avoid co-administration with strong CYP3A inducers. Dose adjustments may be recommended. (2.3, 7, 12.3)
- •
- Gastric Acid Reducing Agents: Avoid co-administration with proton pump inhibitors (PPIs). Stagger dosing with H2-receptor antagonists and antacids. (2.4, 7, 12.3)
Use In Specific Populations
- •
- Pregnancy: May cause fetal harm and dystocia. (8.1)
- •
- Lactation: Advise not to breastfeed (8.2)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 3/2022
Full Prescribing Information
1. Indications and Usage for Calquence
1.1 Mantle Cell Lymphoma
CALQUENCE is indicated for the treatment of adult patients with mantle cell lymphoma (MCL) who have received at least one prior therapy.
This indication is approved under accelerated approval based on overall response rate [see Clinical Studies (14.1)]. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials.
2. Calquence Dosage and Administration
2.1 Recommended Dosage
CALQUENCE as Monotherapy
For patients with MCL, CLL, or SLL, the recommended dose of CALQUENCE is 100 mg taken orally approximately every 12 hours until disease progression or unacceptable toxicity.
CALQUENCE in Combination with Obinutuzumab
For patients with previously untreated CLL or SLL, the recommended dose of CALQUENCE is 100 mg taken orally approximately every 12 hours until disease progression or unacceptable toxicity. Start CALQUENCE at Cycle 1 (each cycle is 28 days). Start obinutuzumab at Cycle 2 for a total of 6 cycles and refer to the obinutuzumab prescribing information for recommended dosing. Administer CALQUENCE prior to obinutuzumab when given on the same day.
Advise patients to swallow capsule whole with water. Advise patients not to open, break or chew the capsules. CALQUENCE may be taken with or without food. If a dose of CALQUENCE is missed by more than 3 hours, it should be skipped and the next dose should be taken at its regularly scheduled time. Extra capsules of CALQUENCE should not be taken to make up for a missed dose.
2.2 Recommended Dosage for Hepatic Impairment
Avoid administration of CALQUENCE in patients with severe hepatic impairment.
Dose modifications are not required for patients with mild or moderate hepatic impairment [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)].
2.3 Recommended Dosage for Drug Interactions
Dose Modifications for Use with CYP3A Inhibitors or Inducers
These are described in Table 1 [see Drug Interactions (7)].
|
CYP3A |
Co-administered Drug |
Recommended CALQUENCE use |
|
Inhibition |
Strong CYP3A inhibitor |
Avoid concomitant use. If these inhibitors will be used short-term (such as anti‑infectives for up to seven days), interrupt CALQUENCE. |
|
Moderate CYP3A inhibitor |
100 mg once daily. |
|
|
Induction |
Strong CYP3A inducer |
Avoid concomitant use. If these inducers cannot be avoided, increase CALQUENCE dose to 200 mg approximately every 12 hours. |
Concomitant Use with Gastric Acid Reducing Agents
Proton Pump Inhibitors: Avoid concomitant use [see Drug Interactions (7)].
H2-Receptor Antagonists: Take CALQUENCE 2 hours before taking a H2-receptor antagonist [see Drug Interactions (7)].
Antacids: Separate dosing by at least 2 hours [see Drug Interactions (7)].
2.4 Dose Modifications for Adverse Reactions
Recommended dose modifications of CALQUENCE for Grade 3 or greater adverse reactions are provided in Table 2.
|
Event |
Adverse Reaction Occurrence |
Dose Modification (Starting dose = 100 mg approximately every 12 hours) |
|
Grade 3 or greater non-hematologic toxicities, Grade 3 thrombocytopenia with bleeding, |
First and Second |
Interrupt CALQUENCE. Once toxicity has resolved to Grade 1 or baseline level, CALQUENCE may be resumed at 100 mg approximately every 12 hours. |
|
Grade 4 thrombocytopenia or Grade 4 neutropenia lasting longer than 7 days |
Third |
Interrupt CALQUENCE. Once toxicity has resolved to Grade 1 or baseline level, CALQUENCE may be resumed at a reduced frequency of 100 mg once daily. |
|
Fourth |
Discontinue CALQUENCE. |
|
|
Adverse reactions graded by the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE). |
||
Refer to the obinutuzumab prescribing information for management of obinutuzumab toxicities.
5. Warnings and Precautions
5.1 Serious and Opportunistic Infections
Fatal and serious infections, including opportunistic infections, have occurred in patients with hematologic malignancies treated with CALQUENCE.
Serious or Grade 3 or higher infections (bacterial, viral, or fungal) occurred in 19% of 1029 patients exposed to CALQUENCE in clinical trials, most often due to respiratory tract infections (11% of all patients, including pneumonia in 6%). These infections predominantly occurred in the absence of Grade 3 or 4 neutropenia, with neutropenic infection reported in 1.9% of all patients. Opportunistic infections in recipients of CALQUENCE have included, but are not limited to, hepatitis B virus reactivation, fungal pneumonia, Pneumocystis jiroveci pneumonia, Epstein-Barr virus reactivation, cytomegalovirus, and progressive multifocal leukoencephalopathy (PML). Consider prophylaxis in patients who are at increased risk for opportunistic infections. Monitor patients for signs and symptoms of infection and treat promptly.
5.2 Hemorrhage
Fatal and serious hemorrhagic events have occurred in patients with hematologic malignancies treated with CALQUENCE. Major hemorrhage (serious or Grade 3 or higher bleeding or any central nervous system bleeding) occurred in 3.0% of patients, with fatal hemorrhage occurring in 0.1% of 1029 patients exposed to CALQUENCE in clinical trials. Bleeding events of any grade, excluding bruising and petechiae, occurred in 22% of patients.
Use of antithrombotic agents concomitantly with CALQUENCE may further increase the risk of hemorrhage. In clinical trials, major hemorrhage occurred in 2.7% of patients taking CALQUENCE without antithrombotic agents and 3.6% of patients taking CALQUENCE with antithrombotic agents. Consider the risks and benefits of antithrombotic agents when co-administered with CALQUENCE. Monitor patients for signs of bleeding.
Consider the benefit-risk of withholding CALQUENCE for 3-7 days pre- and post-surgery depending upon the type of surgery and the risk of bleeding.
5.3 Cytopenias
Grade 3 or 4 cytopenias, including neutropenia (23%), anemia (8%), thrombocytopenia (7%), and lymphopenia (7%), developed in patients with hematologic malignancies treated with CALQUENCE. Grade 4 neutropenia developed in 12% of patients. Monitor complete blood counts regularly during treatment. Interrupt treatment, reduce the dose, or discontinue treatment as warranted [see Dose Modifications for Adverse Reactions (2.4)].
5.4 Second Primary Malignancies
Second primary malignancies, including skin cancers and other solid tumors, occurred in 12% of 1029 patients exposed to CALQUENCE in clinical trials. The most frequent second primary malignancy was skin cancer, reported in 6% of patients. Monitor patients for skin cancers and advise protection from sun exposure.
5.5 Atrial Fibrillation and Flutter
Grade 3 atrial fibrillation or flutter occurred in 1.1% of 1029 patients treated with CALQUENCE, with all grades of atrial fibrillation or flutter reported in 4.1% of all patients. The risk may be increased in patients with cardiac risk factors, hypertension, previous arrhythmias, and acute infection. Monitor for symptoms of arrhythmia (e.g., palpitations, dizziness, syncope, dyspnea) and manage as appropriate.
6. Adverse Reactions/Side Effects
The following clinically significant adverse reactions are discussed in greater detail in other sections of the labeling:
- •
- Serious and Opportunistic Infections [see Warnings and Precautions (5.1)]
- •
- Hemorrhage [see Warnings and Precautions (5.2)]
- •
- Cytopenias [see Warnings and Precautions (5.3)]
- •
- Second Primary Malignancies [see Warnings and Precautions (5.4)]
- •
- Atrial Fibrillation and Flutter [see Warnings and Precautions (5.5)]
6.1 Clinical Trials Experience
As clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The data in the Warnings and Precautions reflect exposure to CALQUENCE 100 mg approximately every 12 hours in 1029 patients with hematologic malignancies. Treatment includes CALQUENCE monotherapy in 820 patients in 6 trials, and CALQUENCE with obinutuzumab in 209 patients in 2 trials. Among these recipients of CALQUENCE, 88% were exposed for at least 6 months and 79% were exposed for at least one year. In this pooled safety population, adverse reactions in ≥ 30% of 1029 patients were anemia, neutropenia, upper respiratory tract infection, thrombocytopenia, headache, diarrhea, and musculoskeletal pain.
Mantle Cell Lymphoma
The safety data described in this section reflect exposure to CALQUENCE (100 mg approximately every 12 hours) in 124 patients with previously treated MCL in Trial LY-004 [see Clinical Studies (14.1)]. The median duration of treatment with CALQUENCE was 16.6 (range: 0.1 to 26.6) months. A total of 91 (73.4%) patients were treated with CALQUENCE for ≥ 6 months and 74 (59.7%) patients were treated for ≥ 1 year.
The most common adverse reactions (≥ 20%) of any grade were anemia, thrombocytopenia, headache, neutropenia, diarrhea, fatigue, myalgia, and bruising. Grade 1 severity for the non-hematologic, most common events were as follows: headache (25%), diarrhea (16%), fatigue (20%), myalgia (15%), and bruising (19%). The most common Grade ≥ 3 non-hematological adverse reaction (reported in at least 2% of patients) was diarrhea.
Dose reductions and discontinuation due to any adverse reaction were reported in 1.6% and 6.5% of patients, respectively.
Tables 3 and 4 present the frequency category of adverse reactions observed in patients with MCL treated with CALQUENCE.
|
||
|
Body System Adverse Reactions* |
CALQUENCE Monotherapy N=124 |
|
|
All Grades (%) |
Grade ≥ 3 (%) |
|
|
Nervous system disorders |
||
|
Headache |
39 |
1.6 |
|
Gastrointestinal disorders |
||
|
Diarrhea |
31 |
3.2 |
|
Nausea |
19 |
0.8 |
|
Abdominal pain |
15 |
1.6 |
|
Constipation |
15 |
- |
|
Vomiting |
13 |
1.6 |
|
General disorders |
||
|
Fatigue |
28 |
0.8 |
|
Musculoskeletal and connective tissue disorders |
||
|
Myalgia |
21 |
0.8 |
|
Skin and subcutaneous tissue disorders |
||
|
Bruising† |
21 |
- |
|
Rash‡ |
18 |
0.8 |
|
Vascular disorders |
||
|
Hemorrhage§ |
8 |
0.8 |
|
Respiratory, thoracic and mediastinal disorders |
||
|
Epistaxis |
6 |
- |
|
||
|
Hematologic Adverse Reactions* |
CALQUENCE Monotherapy N=124 |
|
|
All Grades (%) |
Grade ≥ 3 (%) |
|
|
Hemoglobin decreased |
46 |
10 |
|
Platelets decreased |
44 |
12 |
|
Neutrophils decreased |
36 |
15 |
Increases in creatinine 1.5 to 3 times the upper limit of normal occurred in 4.8% of patients.
Chronic Lymphocytic Leukemia
The safety data described below reflect exposure to CALQUENCE (100 mg approximately every 12 hours, with or without obinutuzumab) in 511 patients with CLL from two randomized controlled clinical trials [see Clinical Studies (14.2)].
The most common adverse reactions (≥ 30%) of any grade in patients with CLL were anemia, neutropenia, thrombocytopenia, headache, upper respiratory tract infection, and diarrhea.
ELEVATE-TN
The safety of CALQUENCE plus obinutuzumab (CALQUENCE+G), CALQUENCE monotherapy, and obinutuzumab plus chlorambucil (GClb) was evaluated in a randomized, multicenter, open-label, actively controlled trial in 526 patients with previously untreated CLL [see Clinical Studies (14.2)].
Patients randomized to the CALQUENCE+G arm were treated with CALQUENCE and obinutuzumab in combination for six cycles, then with CALQUENCE as monotherapy until disease progression or unacceptable toxicity. Patients initiated obinutuzumab on Day 1 of Cycle 2, continuing for a total of 6 cycles. Patient randomized to CALQUENCE monotherapy received CALQUENCE approximately every 12 hours until disease progression or unacceptable toxicity. The trial required age ≥ 65 years of age or 18 to < 65 years of age with a total Cumulative Illness Rating Scale (CIRS) > 6 or creatinine clearance of 30 to 69 mL/min, hepatic transaminases ≤ 3 times upper limit of normal (ULN) and total bilirubin ≤ 1.5 times ULN, and allowed patients to receive antithrombotic agents other than warfarin or equivalent vitamin K antagonists.
During randomized treatment, the median duration of exposure to CALQUENCE in the CALQUENCE+G and CALQUENCE monotherapy arms was 27.7 months (range 0.3 to 40 months), with 95% and 92% and 89% and 86% of patients with at least 6 months and 12 months of exposure, respectively. In the obinutuzumab and chlorambucil arm the median number of cycles was 6 with 84% of patients receiving at least 6 cycles of obinutuzumab, 70% of patients received at least 6 cycles of chlorambucil. Eighty-five percent of patients in the CALQUENCE+G arm received at least 6 cycles of obinutuzumab.
In the CALQUENCE+G and CALQUENCE monotherapy arms, fatal adverse reactions that occurred in the absence of disease progression and with onset within 30 days of the last study treatment were reported in 2% for each treatment arm, most often from infection. Serious adverse reactions were reported in 39% of patients in the CALQUENCE+G arm and 32% in the CALQUENCE monotherapy arm, most often due to events of pneumonia (2.8% to 7%).
In the CALQUENCE+G arm, adverse reactions led to treatment discontinuation in 11% of patients and a dose reduction of CALQUENCE in 7% of patients. In the CALQUENCE monotherapy arm, adverse reactions led to discontinuation in 10% and dose reduction in 4% of patients.
Tables 5 and 6 presents adverse reactions and laboratory abnormalities identified in the ELEVATE-TN trial.
|
||||||
|
Body System Adverse Reaction*
|
CALQUENCE plus Obinutuzumab
|
CALQUENCE Monotherapy N=179 |
Obinutuzumab plus Chlorambucil
|
|||
|
All Grades (%) |
Grade ≥ 3 (%) |
All Grades (%) |
Grade ≥ 3 (%) |
All Grades (%) |
Grade ≥ 3 (%) |
|
|
||||||
|
69 |
22‡ |
65 |
14‡ |
46 |
13‡ |
|
39 |
2.8 |
35 |
0 |
17 |
1.2 |
|
24 |
8 |
18 |
4.5 |
7 |
1.8 |
|
15 |
1.7 |
15 |
2.8 |
5 |
0.6 |
|
||||||
|
53 |
37 |
23 |
13 |
78 |
50 |
|
52 |
12 |
53 |
10 |
54 |
14 |
|
51 |
12 |
32 |
3.4 |
61 |
16 |
|
12 |
11 |
16 |
15 |
0.6 |
0.6 |
|
||||||
|
40 |
1.1 |
39 |
1.1 |
12 |
0 |
|
20 |
0 |
12 |
0 |
7 |
0 |
|
||||||
|
39 |
4.5 |
35 |
0.6 |
21 |
1.8 |
|
20 |
0 |
22 |
0 |
31 |
0 |
|
||||||
|
37 |
2.2 |
32 |
1.1 |
16 |
2.4 |
|
22 |
1.1 |
16 |
0.6 |
4.7 |
1.2 |
|
||||||
|
34 |
2.2 |
23 |
1.1 |
24 |
1.2 |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
20 |
1.7 |
20 |
1.7 |
6 |
0 |
Other clinically relevant adverse reactions (all grades incidence < 15%) in recipients of CALQUENCE (CALQUENCE in combination with obinutuzumab and monotherapy) included:
- •
- Neoplasms: second primary malignancy (10%), non-melanoma skin cancer (5%)
- •
- Cardiac disorders: atrial fibrillation or flutter (3.6%), hypertension (5%)
- •
- Infection: herpesvirus infection (6%)
| Laboratory Abnormality*† | CALQUENCE plus Obinutuzumab
N=178 | CALQUENCE Monotherapy
N=179 | Obinutuzumab plus Chlorambucil
N=169 |
|||
|---|---|---|---|---|---|---|
| All
Grades (%) | Grade ≥ 3 (%) | All
Grades (%) | Grade ≥ 3 (%) | All
Grades (%) | Grade ≥ 3 (%) | |
|
||||||
|
Uric acid increase |
29 |
29 |
22 |
22 |
37 |
37 |
|
ALT increase |
30 |
7 |
20 |
1.1 |
36 |
6 |
|
AST increase |
38 |
5 |
17 |
0.6 |
60 |
8 |
|
Bilirubin increase |
13 |
0.6 |
15 |
0.6 |
11 |
0.6 |
Increases in creatinine 1.5 to 3 times the upper limit of normal occurred in 3.9% and 2.8% of patients in the CALQUENCE combination arm and monotherapy arm, respectively.
ASCEND
The safety of CALQUENCE in patients with relapsed or refractory CLL was evaluated in a randomized, open-label study (ASCEND) [see Clinical Studies (14.2)]. The trial enrolled patients with relapsed or refractory CLL after at least one prior therapy and required hepatic transaminases ≤ 2 times upper limit of normal (ULN), total bilirubin ≤ 1.5 times ULN, and an estimated creatinine clearance ≥ 30 mL/min. The trial excluded patients having an absolute neutrophil count < 500/µL, platelet count < 30,000/µL, prothrombin time or activated partial thromboplastin time > 2 times ULN, significant cardiovascular disease, or a requirement for strong CYP3A inhibitors or inducers. Patients were allowed to receive antithrombotic agents other than warfarin or equivalent vitamin K antagonist.
In ASCEND, 154 patients received CALQUENCE (100 mg approximately every 12 hours until disease progression or unacceptable toxicity), 118 received idelalisib (150 mg approximately every 12 hours until disease progression or unacceptable toxicity) with up to 8 infusions of a rituximab product, and 35 received up to 6 cycles of bendamustine and a rituximab product. The median age overall was 68 years (range: 32-90); 67% were male; 92% were white; and 88% had an ECOG performance status of 0 or 1.
In the CALQUENCE arm, serious adverse reactions occurred in 29% of patients. Serious adverse reactions in > 5% of patients who received CALQUENCE included lower respiratory tract infection (6%). Fatal adverse reactions within 30 days of the last dose of CALQUENCE occurred in 2.6% of patients, including from second primary malignancies and infection.
In recipients of CALQUENCE, permanent discontinuation due to an adverse reaction occurred in 10% of patients, most frequently due to second primary malignancies followed by infection. Adverse reactions led to dosage interruptions of CALQUENCE in 34% of patients, most often due to respiratory tract infections followed by neutropenia, and dose reduction in 3.9% of patients.
Selected adverse reactions are described in Table 7 and non-hematologic laboratory abnormalities are described in Table 8. These tables reflect exposure to CALQUENCE with median duration of 15.7 months with 94% of patients on treatment for greater than 6 months and 86% of patients on treatment for greater than 12 months. The median duration of exposure to idelalisib was 11.5 months with 72% of patients on treatment for greater than 6 months and 48% of patients on treatment for greater than 12 months. Eighty-three percent of patients completed 6 cycles of bendamustine and rituximab product.
|
||||||
|
Body System Adverse Reaction*
|
CALQUENCE N=154 |
Idelalisib plus Rituximab Product N=118 |
Bendamustine plus Rituximab Product N=35 |
|||
|
All
|
Grade ≥ 3 (%) |
All
|
Grade ≥ 3 (%) |
All
|
Grade ≥ 3 (%) |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
Other clinically relevant adverse reactions (all grades incidence < 15%) in recipients of CALQUENCE included:
- •
- Skin and subcutaneous disorders: bruising (10%), rash (9%)
- •
- Neoplasms: second primary malignancy (12%), non-melanoma skin cancer (6%)
- •
- Musculoskeletal and connective tissue disorders: arthralgia (8%)
- •
- Cardiac disorders: atrial fibrillation or flutter (5%), hypertension (3.2%)
- •
- Infection: herpesvirus infection (4.5%)
| Laboratory Abnormality* | CALQUENCE
N=154 | Idelalisib plus Rituximab Product
N=118 | Bendamustine plus Rituximab Product
N=35 |
|||
|---|---|---|---|---|---|---|
| All
Grades (%) | Grade ≥ 3 (%) | All
Grades (%) | Grade ≥ 3 (%) | All
Grades (%) | Grade ≥ 3 (%) | |
|
||||||
|
Uric acid increase |
15 |
15 |
11 |
11 |
23 |
23 |
|
ALT increase |
15 |
1.9 |
59 |
23 |
26 |
2.9 |
|
AST increase |
13 |
0.6 |
48 |
13 |
31 |
2.9 |
|
Bilirubin increase |
13 |
1.3 |
16 |
1.7 |
26 |
11 |
|
Per NCI CTCAE version 5 |
||||||
7. Drug Interactions
|
Strong CYP3A Inhibitors |
||
|
Clinical Impact |
|
|
|
Prevention or Management |
|
|
|
Moderate CYP3A Inhibitors |
||
|
Clinical Impact |
|
|
|
Prevention or Management |
|
|
|
Strong CYP3A Inducers |
||
|
Clinical Impact |
|
|
|
Prevention or Management |
|
|
|
Gastric Acid Reducing Agents |
||
|
Clinical Impact |
|
|
|
Prevention or Management |
Antacids |
Separate dosing by at least 2 hours [see Recommended Dosage for Drug Interactions (2.3)]. |
|
H2-receptor antagonists |
Take CALQUENCE 2 hours before taking the H2-receptor antagonist [see Recommended Dosage for Drug Interactions (2.3)]. |
|
|
Proton pump inhibitors |
Avoid co-administration. Due to the long-lasting effect of proton pump inhibitors, separation of doses may not eliminate the interaction with CALQUENCE. |
|
8. Use In Specific Populations
8.1 Pregnancy
Risk Summary
Based on findings in animals, CALQUENCE may cause fetal harm and dystocia when administered to a pregnant woman. There are no available data in pregnant women to inform the drug-associated risk. In animal reproduction studies, administration of acalabrutinib to animals during organogenesis resulted in dystocia in rats and reduced fetal growth in rabbits at maternal exposures (AUC) 2 times exposures in patients at the recommended dose of 100 mg approximately every 12 hours (see Data). Advise pregnant women of the potential risk to a fetus.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and 15-20%, respectively.
Data
Animal Data
In a combined fertility and embryo-fetal development study in female rats, acalabrutinib was administered orally at doses up to 200 mg/kg/day starting 14 days prior to mating through gestational day [GD] 17. No effects on embryo-fetal development and survival were observed. The AUC at 200 mg/kg/day in pregnant rats was approximately 9-times the AUC in patients at the recommended dose of 100 mg approximately every 12 hours. The presence of acalabrutinib and its active metabolite were confirmed in fetal rat plasma.
In an embryo-fetal development study in rabbits, pregnant animals were administered acalabrutinib orally at doses up to 200 mg/kg/day during the period of organogenesis (from GD 6-18). Administration of acalabrutinib at doses ≥ 100 mg/kg/day produced maternal toxicity and 100 mg/kg/day resulted in decreased fetal body weights and delayed skeletal ossification. The AUC at 100 mg/kg/day in pregnant rabbits was approximately 2-times the AUC in patients at 100 mg approximately every 12 hours.
In a pre- and postnatal development study in rats, acalabrutinib was administered orally to pregnant animals during organogenesis, parturition and lactation, at doses of 50, 100, and 150 mg/kg/day. Dystocia (prolonged or difficult labor) and mortality of offspring were observed at doses ≥ 100 mg/kg/day. The AUC at 100 mg/kg/day in pregnant rats was approximately 2-times the AUC in patients at 100 mg approximately every 12 hours. Underdeveloped renal papilla was also observed in F1 generation offspring at 150 mg/kg/day with an AUC approximately 5-times the AUC in patients at 100 mg approximately every 12 hours.
8.2 Lactation
Risk Summary
No data are available regarding the presence of acalabrutinib or its active metabolite in human milk, its effects on the breastfed child, or on milk production. Acalabrutinib and its active metabolite were present in the milk of lactating rats. Due to the potential for adverse reactions in a breastfed child from CALQUENCE, advise lactating women not to breastfeed while taking CALQUENCE and for at least 2 weeks after the final dose.
8.3 Females and Males of Reproductive Potential
Pregnancy
Pregnancy testing is recommended for females of reproductive potential prior to initiating CALQUENCE therapy.
Contraception
Females
CALQUENCE may cause embryo-fetal harm and dystocia when administered to pregnant women [see Use in Specific Populations (8.1)]. Advise female patients of reproductive potential to use effective contraception during treatment with CALQUENCE and for at least 1 week following the last dose of CALQUENCE. If this drug is used during pregnancy, or if the patient becomes pregnant while taking this drug, the patient should be informed of the potential hazard to a fetus.
8.4 Pediatric Use
The safety and efficacy of CALQUENCE in pediatric patients have not been established.
8.5 Geriatric Use
Of the 929 patients with CLL or MCL in clinical trials of CALQUENCE, 68% were 65 years of age or older, and 24% were 75 years of age or older. Among patients 65 years of age or older, 59% had Grade 3 or higher adverse reactions and 39% had serious adverse reactions. Among patients younger than age 65, 45% had Grade 3 or higher adverse reactions and 25% had serious adverse reactions. No clinically relevant differences in efficacy were observed between patients ≥ 65 years and younger.
11. Calquence Description
CALQUENCE (acalabrutinib) is an inhibitor of Bruton tyrosine kinase (BTK). The molecular formula for acalabrutinib is C26H23N7O2, and the molecular weight is 465.51. The chemical name is 4-{8-amino-3-[(2S)-1-(but-2-ynoyl)pyrrolidin-2-yl]imidazo[1,5-a]pyrazin-1-yl)}-N-(pyridine-2-yl)benzamide.
The chemical structure of acalabrutinib is shown below:
Acalabrutinib is a white to yellow powder with pH-dependent solubility. It is freely soluble in water at pH values below 3 and practically insoluble at pH values above 6.
CALQUENCE capsules for oral administration contains 100 mg acalabrutinib and the following inactive ingredients: silicified microcrystalline cellulose, partially pregelatinized starch, magnesium stearate, and sodium starch glycolate. The capsule shell contains gelatin, titanium dioxide, yellow iron oxide, FD&C Blue 2 and is imprinted with edible black ink.
12. Calquence - Clinical Pharmacology
12.1 Mechanism of Action
Acalabrutinib is a small-molecule inhibitor of BTK. Acalabrutinib and its active metabolite, ACP-5862, form a covalent bond with a cysteine residue in the BTK active site, leading to inhibition of BTK enzymatic activity. BTK is a signaling molecule of the B cell antigen receptor (BCR) and cytokine receptor pathways. In B cells, BTK signaling results in activation of pathways necessary for B-cell proliferation, trafficking, chemotaxis, and adhesion. In nonclinical studies, acalabrutinib inhibited BTK-mediated activation of downstream signaling proteins CD86 and CD69 and inhibited malignant B-cell proliferation and tumor growth in mouse xenograft models.
12.2 Pharmacodynamics
In patients with B-cell malignancies dosed with 100 mg approximately every 12 hours, median steady state BTK occupancy of ≥ 95% in peripheral blood was maintained over 12 hours, resulting in inactivation of BTK throughout the recommended dosing interval.
Cardiac Electrophysiology
The effect of acalabrutinib on the QTc interval was evaluated in a randomized, double-blind, double-dummy, placebo‑ and positive-controlled, 4-way crossover thorough QTc study in 48 healthy adult subjects. Administration of a single dose of acalabrutinib that is the 4-fold maximum recommended single dose did not prolong the QTc interval to any clinically relevant extent (i.e., ≥ 10 ms).
12.3 Pharmacokinetics
Acalabrutinib exhibits dose-proportionality, and both acalabrutinib and its active metabolite, ACP-5862, exposures increase with dose across a dose range of 75 to 250 mg (0.75 to 2.5 times the approved recommended single dose) in patients with B-cell malignancies. At the recommended dose of 100 mg twice daily, the geometric mean (% coefficient of variation [CV]) daily area under the plasma drug concentration over time curve (AUC24h) and maximum plasma concentration (Cmax) for acalabrutinib were 1843 (38%) ng•h/mL and 563 (29%) ng/mL, respectively, and for ACP-5862 were 3947 (43%) ng•h/mL and 451 (52%) ng/mL, respectively.
Absorption
The geometric mean absolute bioavailability of acalabrutinib was 25%. Median [min, max] time to peak acalabrutinib plasma concentrations (Tmax) was 0.9 [0.5, 1.9] hours, and 1.6 [0.9, 2.7] hour for ACP-5862.
Effect of Food
In healthy subjects, administration of a single 75 mg dose of acalabrutinib (0.75 times the approved recommended single dose) with a high-fat, high-calorie meal (approximately 918 calories, 59 grams carbohydrate, 59 grams fat, and 39 grams protein) did not affect the mean AUC as compared to dosing under fasted conditions. Resulting Cmax decreased by 73% and Tmax was delayed 1-2 hours.
Distribution
Reversible binding to human plasma protein was 97.5% for acalabrutinib and 98.6% for ACP-5862. The in vitro mean blood-to-plasma ratio was 0.8 for acalabrutinib and 0.7 for ACP-5862. The geometric mean (% CV) steady-state volume of distribution (Vss) was approximately 101 (52%) L for acalabrutinib and 67 (32%) L for ACP-5862.
Elimination
The geometric mean (% CV) terminal elimination half-life (t1/2) was 1 (59%) hour for acalabrutinib and 3.5 (24%) hours for ACP-5862. The geometric mean (%CV) apparent oral clearance (CL/F) was 71 (35%) L/hr for acalabrutinib and 13 (42%) L/hr for ACP-5862.
Metabolism
Acalabrutinib is predominantly metabolized by CYP3A enzymes, and to a minor extent, by glutathione conjugation and amide hydrolysis, based on in vitro studies. ACP-5862 was identified as the major active metabolite in plasma with a geometric mean exposure (AUC) that was approximately 2- to 3-fold higher than the exposure of acalabrutinib. ACP-5862 is approximately 50% less potent than acalabrutinib with regard to BTK inhibition.
Excretion
Following administration of a single 100 mg radiolabeled acalabrutinib dose in healthy subjects, 84% of the dose was recovered in the feces and 12% of the dose was recovered in the urine, with less than 2% of the dose excreted as unchanged acalabrutinib in urine and feces.
Specific Populations
Age, Race, and Body Weight
Age (32 to 90 years), sex, race (Caucasian, African American), and body weight (40 to 149 kg) did not have clinically meaningful effects on the PK of acalabrutinib and its active metabolite, ACP-5862.
Renal Impairment
No clinically relevant PK difference was observed in patients with mild or moderate renal impairment (eGFR ≥ 30 mL/min/1.73m2, as estimated by MDRD (modification of diet in renal disease equation)). Acalabrutinib PK has not been evaluated in patients with severe renal impairment (eGFR < 29 mL/min/1.73m2, MDRD) or renal impairment requiring dialysis.
Hepatic Impairment
The AUC of acalabrutinib increased 1.9-fold in subjects with mild hepatic impairment (Child-Pugh class A), 1.5-fold in subjects with moderate hepatic impairment (Child-Pugh class B) and 5.3-fold in subjects with severe hepatic impairment (Child-Pugh class C) compared to subjects with normal liver function. No clinically relevant PK difference in ACP-5862 was observed in subjects with severe hepatic impairment (Child-Pugh Class C) compared to subjects with normal liver function. No clinically relevant PK differences in acalabrutinib and ACP-5862 were observed in patients with mild or moderate hepatic impairment (total bilirubin less and equal to upper limit of normal [ULN] and AST greater than ULN, or total bilirubin greater than ULN and any AST) relative to patients with normal hepatic function (total bilirubin and AST within ULN).
Drug Interaction Studies
Effect of CYP3A Inhibitors on Acalabrutinib
Co-administration with a strong CYP3A inhibitor (200 mg itraconazole once daily for 5 days) increased the acalabrutinib Cmax by 3.9-fold and AUC by 5.1-fold in healthy subjects.
Physiologically based pharmacokinetic (PBPK) simulations with acalabrutinib and moderate CYP3A inhibitors (erythromycin, fluconazole, diltiazem) showed that co-administration increased acalabrutinib Cmax and AUC approximately 2- to 3-fold.
Effect of CYP3A Inducers on Acalabrutinib
Co-administration with a strong CYP3A inducer (600 mg rifampin once daily for 9 days) decreased acalabrutinib Cmax by 68% and AUC by 77% in healthy subjects.
Gastric Acid Reducing Agents
Acalabrutinib solubility decreases with increasing pH. Co-administration with an antacid (1 g calcium carbonate) decreased acalabrutinib AUC by 53% in healthy subjects. Co-administration with a proton pump inhibitor (40 mg omeprazole for 5 days) decreased acalabrutinib AUC by 43%.
In Vitro Studies
Metabolic Pathways
Acalabrutinib is a weak inhibitor of CYP3A4/5, CYP2C8 and CYP2C9, but does not inhibit CYP1A2, CYP2B6, CYP2C19, CYP2D6, UGT1A1, and UGT2B7. ACP-5862 is a weak inhibitor of CYP2C8, CYP2C9 and CYP2C19, but does not inhibit CYP1A2, CYP2B6, CYP2D6, CYP3A4/5, UGT1A1, and UGT2B7.
Acalabrutinib is a weak inducer of CYP1A2, CYP2B6 and CYP3A4; ACP-5862 weakly induces CYP3A4.
Based on in vitro data and PBPK modeling, no interaction with CYP substrates is expected at clinically relevant concentrations.
Drug Transporter Systems
Acalabrutinib and its active metabolite, ACP-5862, are substrates of P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP). Acalabrutinib is not a substrate of renal uptake transporters OAT1, OAT3, and OCT2, or hepatic transporters OATP1B1, and OATP1B3. ACP-5862 is not a substrate of OATP1B1 or OATP1B3.
Acalabrutinib and ACP-5862 do not inhibit P-gp, OAT1, OAT3, OCT2, OATP1B1, OATP1B3, and MATE2-K at clinically relevant concentrations.
Acalabrutinib may increase exposure to co-administered BCRP substrates (e.g., methotrexate) by inhibition of intestinal BCRP. ACP-5862 does not inhibit BCRP at clinically relevant concentrations. Acalabrutinib does not inhibit MATE1, while ACP-5862 may increase exposure to co-administered MATE1 substrates (e.g., metformin) by inhibition of MATE1.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies have not been conducted with acalabrutinib.
Acalabrutinib was not mutagenic in an in vitro bacterial reverse mutation (AMES) assay or clastogenic in an in vitro human lymphocyte chromosomal aberration assay or in an in vivo rat bone marrow micronucleus assay.
In a fertility study in rats, there were no effects of acalabrutinib on fertility in male rats at exposures 11‑times, or in female rats at exposures 9‑times the AUC observed in patients at the recommended dose of 100 mg twice daily.
14. Clinical Studies
14.1 Mantle Cell Lymphoma
The efficacy of CALQUENCE was based upon Trial LY-004 titled “An Open-label, Phase 2 Study of ACP-196 in Subjects with Mantle Cell Lymphoma” (NCT02213926). Trial LY-004 enrolled a total of 124 patients with MCL who had received at least one prior therapy.
The median age was 68 (range 42 to 90) years, 80% were male, and 74% were Caucasian. At baseline, 93% of patients had an ECOG performance status of 0 or 1. The median time since diagnosis was 46.3 months and the median number of prior treatments was 2 (range 1 to 5), including 18% with prior stem cell transplant. Patients who received prior treatment with BTK inhibitors were excluded. The most common prior regimens were CHOP-based (52%) and ARA-C (34%). At baseline, 37% of patients had at least one tumor with a longest diameter ≥ 5 cm, 73% had extra nodal involvement including 51% with bone marrow involvement. The simplified MIPI score (which includes age, ECOG score, and baseline lactate dehydrogenase and white cell count) was intermediate in 44% and high in 17% of patients.
CALQUENCE was administered orally at 100 mg approximately every 12 hours until disease progression or unacceptable toxicity. The median dose intensity was 98.5%. The major efficacy outcome of Trial LY-004 was overall response rate and the median follow-up was 15.2 months.
|
||
|
Investigator Assessed N=124 |
Independent Review Committee (IRC) Assessed N=124 |
|
|
Overall Response Rate (ORR)* |
||
|
ORR (%) [95% CI] |
81 [73, 87] |
80 [72, 87] |
|
Complete Response (%) [95% CI] |
40 [31, 49] |
40 [31, 49] |
|
Partial Response (%) [95% CI] |
41 [32, 50] |
40 [32, 50] |
|
Duration of Response (DoR) |
||
|
Median DoR in months [range] |
NE [1+ to 20+] |
NE [0+ to 20+] |
|
CI= Confidence Interval; NE=Not Estimable; + indicates censored observations |
||
The median time to best response was 1.9 months.
Lymphocytosis
Upon initiation of CALQUENCE, a temporary increase in lymphocyte counts (defined as absolute lymphocyte count (ALC) increased ≥ 50% from baseline and a post baseline assessment ≥ 5 x 109) in 31.5% of patients in Trial LY-004. The median time to onset of lymphocytosis was 1.1 weeks and the median duration of lymphocytosis was 6.7 weeks.
14.2 Chronic Lymphocytic Leukemia
The efficacy of CALQUENCE in patients with CLL was demonstrated in two randomized, controlled trials. The indication for CALQUENCE includes patients with SLL because it is the same disease.
ELEVATE-TN
The efficacy of CALQUENCE was evaluated in the ELEVATE-TN trial, a randomized, multicenter, open-label, actively controlled, 3 arm trial of CALQUENCE in combination with obinutuzumab, CALQUENCE monotherapy, and obinutuzumab in combination with chlorambucil in 535 patients with previously untreated chronic lymphocytic leukemia (NCT02475681). Patients 65 years of age or older or between 18 and 65 years of age with a total Cumulative Illness Rating Scale (CIRS) > 6 or creatinine clearance of 30 to 69 mL/min were enrolled. The trial also required hepatic transaminases ≤ 3 times upper limit of normal (ULN) and total bilirubin ≤ 1.5 times ULN, and excluded patients with Richter’s transformation.
Patients were randomized in a 1:1:1 ratio into 3 arms to receive:
- •
- CALQUENCE plus obinutuzumab (CALQUENCE+G): CALQUENCE 100 mg was administered approximately every 12 hours starting on Cycle 1 Day 1 until disease progression or unacceptable toxicity. Obinutuzumab was administered starting on Cycle 2 Day 1 for a maximum of 6 treatment cycles. Obinutuzumab 1000 mg was administered on Days 1 and 2 (100 mg on Day 1 and 900 mg on Day 2), 8 and 15 of Cycle 2 followed by 1000 mg on Day 1 of Cycles 3 up to 7. Each cycle was 28 days.
- •
- CALQUENCE monotherapy: CALQUENCE 100 mg was administered approximately every 12 hours until disease progression or unacceptable toxicity.
- •
- Obinutuzumab plus chlorambucil (GClb): Obinutuzumab and chlorambucil were administered for a maximum of 6 treatment cycles. Obinutuzumab 1000 mg was administered intravenously on Days 1 and 2 (100 mg on Day 1 and 900 mg on Day 2), 8 and 15 of Cycle 1 followed by 1000 mg on Day 1 of Cycles 2 to 6. Chlorambucil 0.5 mg/kg was administered orally on Days 1 and 15 of Cycles 1 to 6. Each cycle was 28 days.
Randomization was stratified by 17p deletion mutation status, ECOG performance status (0 or 1 versus 2), and geographic region. A total of 535 patients were randomized, 179 to CALQUENCE+G, 179 to CALQUENCE monotherapy, and 177 to GClb. The overall median age was 70 years (range: 41 to 91 years), 47% had Rai stage III or IV disease, 14% had 17p deletion or TP53 mutation, 63% of patients had an unmutated IGVH, and 18% had 11q deletion. Baseline demographic and disease characteristics were similar between treatment arms.
Efficacy was based on progression-free survival (PFS) as assessed by an Independent Review Committee (IRC). The median duration of follow-up was 28.3 months (range: 0.0 to 40.8 months). Efficacy results are presented in Table 10. The Kaplan-Meier curves for PFS are shown in Figure 1.
|
|||
|
CALQUENCE plus Obinutuzumab N=179 |
CALQUENCE Monotherapy N=179 |
Obinutuzumab plus Chlorambucil N=177 |
|
|
Progression-Free Survival* |
|||
|
Number of events (%) |
14 (8) |
26 (15) |
93 (53) |
|
PD, n (%) |
9 (5) |
20 (11) |
82 (46) |
|
Death events, n (%) |
5 (3) |
6 (3) |
11 (6) |
|
Median (95% CI), months† |
NE |
NE (34, NE) |
22.6 (20, 28) |
|
HR‡(95% CI) |
0.10 (0.06, 0.17) |
0.20 (0.13, 0.30) |
- |
|
p-value§ |
< 0.0001 |
< 0.0001 |
- |
|
Overall Response Rate* (CR + CRi + nPR + PR) |
|||
|
ORR, n (%) |
168 (94) |
153 (86) |
139 (79) |
|
(95% CI) |
(89, 97) |
(80, 90) |
(72, 84) |
|
p-value¶ |
< 0.0001 |
0.0763 |
- |
|
CR, n (%) |
23 (13) |
1 (1) |
8 (5) |
|
CRi, n (%) |
1 (1) |
0 |
0 |
|
nPR, n (%) |
1 (1) |
2 (1) |
3 (2) |
|
PR, n (%) |
143 (80) |
150 (84) |
128 (72) |
|
ITT=intent-to-treat; CI=confidence interval; HR=hazard ratio; NE=not estimable; CR=complete response; CRi=complete response with incomplete blood count recovery; nPR=nodular partial response; PR=partial response. |
|||
Figure 1: Kaplan-Meier Curve of IRC-Assessed PFS in Patients with CLL in ELEVATE-TN
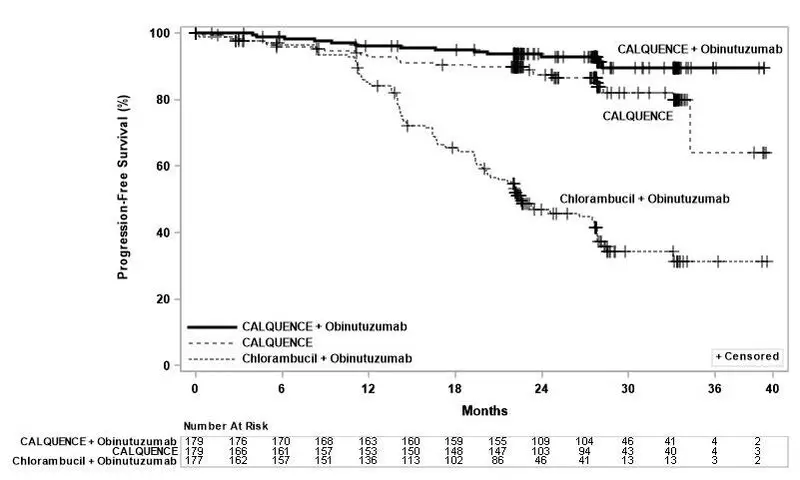
With a median follow-up of 28.3 months, median overall survival was not reached in any arm, with fewer than 10% of patients experiencing an event.
ASCEND
The efficacy of CALQUENCE in patients with relapsed or refractory CLL was based upon a multicenter, randomized, open-label trial (ASCEND; NCT02970318). The trial enrolled 310 patients with relapsed or refractory CLL after at least 1 prior systemic therapy. The trial excluded patients with transformed disease, prolymphocytic leukemia, or previous treatment with venetoclax, a Bruton tyrosine kinase inhibitor, or a phosphoinositide-3 kinase inhibitor.
Patients were randomized in a 1:1 ratio to receive either:
- •
- CALQUENCE 100 mg approximately every 12 hours until disease progression or unacceptable toxicity, or
- •
- Investigator’s choice:
- •
- Idelalisib plus a rituximab product (IR): Idelalisib 150 mg orally approximately every 12 hours until disease progression or unacceptable toxicity, in combination with 8 infusions of a rituximab product (375 mg/m2 intravenously on Day 1 of Cycle 1, followed by 500 mg/m2 every 2 weeks for 4 doses and then every 4 weeks for 3 doses), with a 28-day cycle length.
- •
- Bendamustine plus a rituximab product (BR): Bendamustine 70 mg/m2 intravenously (Day 1 and 2 of each 28-day cycle), in combination with a rituximab product (375 mg/m2 intravenously on Day 1 of Cycle 1, then 500 mg/m2 on Day 1 of subsequent cycles), for up to 6 cycles.
Randomization was stratified by 17p deletion mutation status, ECOG performance status (0 or 1 versus 2), and number of prior therapies (1 to 3 versus ≥ 4). Of 310 patients total, 155 were assigned to CALQUENCE monotherapy, 119 to IR, and 36 to BR. The median age overall was 67 years (range: 32 to 90 years), 42% had Rai stage III or IV disease, 28% had 17p deletion or TP53 mutation, 78% of patients had an unmutated IGVH, and 27% had a 11q deletion. The CALQUENCE arm had a median of 1 prior therapy (range 1-8), with 47% having at least 2 prior therapies. The investigator’s choice arm had a median of 2 prior therapies (range 1-10), with 57% having at least 2 prior therapies.
In the CALQUENCE arm, the median treatment duration was 15.7 months, with 94% of patients treated for at least 6 months and 86% of patients treated for at least 1 year. In the investigator’s choice arm, the median treatment duration was 8.4 months, with 59% of patients treated for at least 6 months and 37% treated for at least 1 year.
Efficacy was based on PFS as assessed by an IRC, with a median follow-up of 16.1 months (range 0.03 to 22.4 months). Efficacy results are presented in Table 11. The Kaplan-Meier curve for PFS is shown in Figure 2. There was no statistically significant difference in overall response rates between the two treatment arms.
| CALQUENCE Monotherapy
N=155 | Investigator’s Choice of Idelalisib + Rituximab Product or Bendamustine + Rituximab Product
N=155 |
|
|---|---|---|
|
||
|
Progression-Free Survival* |
||
|
Number of events, n (%) |
27 (17) |
68 (44) |
|
Disease progression, n |
19 |
59 |
|
Death, n |
8 |
9 |
|
Median (95% CI), months† |
NE (NE, NE) |
16.5 (14.0, 17.1) |
|
HR (95% CI)‡ |
0.31 (0.20, 0.49) |
|
|
P-value§ |
< 0.0001 |
|
|
Overall Response Rate (CR + CRi + nPR + PR)*¶ |
||
|
ORR, n (%)¶ |
126 (81) |
117 (75) |
|
(95% CI) |
(74, 87) |
(68, 82) |
|
CR, n (%) |
0 |
2 (1) |
|
CRi, n (%) |
0 |
0 |
|
nPR, n (%) |
0 |
0 |
|
PR, n (%) |
126 (81) |
115 (74) |
|
ITT=intent-to-treat; CI=confidence interval; HR=hazard ratio; NE=not estimable; CR=complete response; CRi=complete response with incomplete blood count recovery; nPR=nodular partial response; PR=partial response |
||
Figure 2: Kaplan-Meier Curve of IRC-Assessed PFS in Patients with CLL in ASCEND
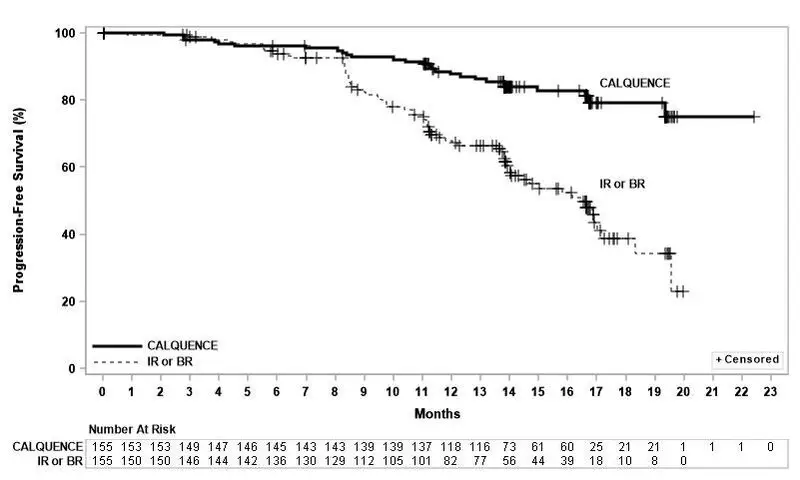
With a median follow up of 16.1 months, median overall survival was not reached in either arm, with fewer than 11% of patients experiencing an event.
16. How is Calquence supplied
How Supplied
|
Pack Size |
Contents |
NDC Number |
|
60-count bottle |
Bottle containing 60 capsules 100 mg, hard gelatin capsules with yellow body and blue cap, marked in black ink with ‘ACA 100 mg’ |
0310-0512-60 |
Storage
Store at 20°C-25°C (68°F-77°F); excursions permitted to 15°C-30°C (59°F-86°F) [see USP Controlled Room Temperature].
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Serious and Opportunistic Infections
Inform patients of the possibility of serious infection and to report signs or symptoms suggestive of infection [see Warnings and Precautions (5.1)].
Hemorrhage
Inform patients to report signs or symptoms of bleeding. Inform patients that CALQUENCE may need to be interrupted for major surgeries [see Warnings and Precautions (5.2)].
Cytopenias
Inform patients that they will need periodic blood tests to check blood counts during treatment with CALQUENCE [see Warnings and Precautions (5.3)].
Second Primary Malignancies
Inform patients that other malignancies have been reported in patients who have been treated with CALQUENCE, including skin cancer and other solid tumors. Advise patients to use sun protection [see Warnings and Precautions (5.4)].
Atrial Fibrillation and Flutter
Counsel patients to report any signs of palpitations, dizziness, fainting, chest discomfort, and shortness of breath [see Warnings and Precautions (5.5)].
Pregnancy Complication
CALQUENCE may cause fetal harm and dystocia. Advise women to avoid becoming pregnant during treatment and for at least 1 week after the last dose of CALQUENCE [see Use in Specific Populations (8.3)].
Lactation
Advise females not to breastfeed during treatment with CALQUENCE and for at least 2 weeks after the final dose [see Use in Specific Populations (8.2)].
Dosing Instructions
Instruct patients to take CALQUENCE orally twice daily, about 12 hours apart. CALQUENCE may be taken with or without food. Advise patients that CALQUENCE capsules should be swallowed whole with a glass of water, without being opened, broken, or chewed [see Dosage and Administration (2.1)].
Missed Dose
Advise patients that if they miss a dose of CALQUENCE, they may still take it up to 3 hours after the time they would normally take it. If more than 3 hours have elapsed, they should be instructed to skip that dose and take their next dose of CALQUENCE at the usual time. Warn patients they should not take extra capsules to make up for the dose that they missed [see Dosage and Administration (2.1)].
Drug Interactions
Advise patients to inform their healthcare providers of all concomitant medications, including over-the-counter medications, vitamins and herbal products [see Drug Interactions (7)].
Distributed by:
AstraZeneca Pharmaceuticals LP
Wilmington, DE 19850
CALQUENCE is a registered trademark of the AstraZeneca group of companies.
©AstraZeneca 2019
|
PATIENT INFORMATION CALQUENCE® (KAL-kwens) (acalabrutinib) Capsules |
|
|
What is CALQUENCE? CALQUENCE is a prescription medicine used to treat adults with:
It is not known if CALQUENCE is safe and effective in children. |
|
|
Before taking CALQUENCE, tell your healthcare provider about all of your medical conditions, including if you:
Tell your healthcare provider about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Taking CALQUENCE with certain other medications may affect how CALQUENCE works and can cause side effects. Especially tell your healthcare provider if you take a blood thinner medicine. |
|
|
How should I take CALQUENCE?
|
|
|
What are the possible side effects of CALQUENCE? CALQUENCE may cause serious side effects, including:
|
|
|
|
|
|
|
|
|
The most common side effects of CALQUENCE include: |
|
|
|
|
These are not all of the possible side effects of CALQUENCE. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|
|
How should I store CALQUENCE?
|
|
|
General information about the safe and effective use of CALQUENCE. Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use CALQUENCE for a condition for which it was not prescribed. Do not give CALQUENCE to other people, even if they have the same symptoms you have. It may harm them. You can ask your healthcare provider or pharmacist for more information about CALQUENCE that is written for health professionals. |
|
|
What are the ingredients in CALQUENCE? Active ingredient: acalabrutinib Inactive ingredients: silicified microcrystalline cellulose, pregelatinized starch, magnesium stearate, and sodium starch glycolate. Capsule shell contains: gelatin, titanium dioxide, yellow iron oxide, FD&C Blue 2, and black ink. |
|
|
Distributed by: AstraZeneca Pharmaceuticals LP, Wilmington, DE 19850 CALQUENCE is a registered trademark of the AstraZeneca group of companies. ©AstraZeneca XXXX For more information, go to www.CALQUENCE.com or call 1-800-236-9933. |
|
This Patient Information has been approved by the U.S. Food and Drug Administration. Revised: 11/2019
| CALQUENCE
acalabrutinib capsule, gelatin coated |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
| Labeler - AstraZeneca Pharmaceuticals LP (054743190) |
| Registrant - AstraZeneca PLC (230790719) |
