Drug Detail:Flo-pred (Prednisolone [ pred-nis-oh-lone ])
Drug Class: Glucocorticoids
Highlights of Prescribing Information
Flo-Pred (prednisolone acetate) Suspension for Oral use
Initial U.S. Approval: 1955
Indications and Usage for Flo-Pred
Flo-Pred is a corticosteroid indicated
- as an anti-inflammatory or immunosuppressive agent for certain allergic, dermatologic, gastrointestinal, hematologic, ophthalmologic, nervous system, renal, respiratory, rheumatologic, specific infectious diseases or conditions and organ transplantation (1)
- for the treatment of certain endocrine conditions (1)
- for palliation of certain neoplastic conditions (1)
Flo-Pred Dosage and Administration
Individualize dosing based on disease severity and patient response (2):
- Initial Dose: 5 mg to 60 mg of prednisolone (as 5.6 mg to 67 mg of prednisolone acetate)
- Maintenance Dose: Use lowest dosage that will maintain an adequate clinical response.
- Discontinuation: Withdraw gradually if discontinuing long-term or high-dose therapy
- Take with food to avoid gastrointestinal (GI) irritation.
Dosage Forms and Strengths
Oral Suspension:
- 15 mg per 5 mL (as 16.7 mg/5 mL of prednisolone acetate) (3)
- Dispense only in original containers (16)
Contraindications
- Hypersensitivity to prednisolone or any component of this product. (4)
Warnings and Precautions
- Hypothalamic-pituitary-adrenal (HPA) axis suppression, Cushing's syndrome and hyperglycemia: Monitor patients for these conditions with chronic use. Taper doses gradually for withdrawal after chronic use. (5.1)
- Infections: Increased susceptibility to new infection and increased risk of exacerbation, dissemination, or reactivation of latent infection. Signs and symptoms of infection may be masked (5.2)
- Elevated blood pressure, salt and water retention and hypokalemia: Monitor blood pressure and sodium, potassium serum levels (5.3)
- GI perforation: increased risk in patients with certain GI disorders. Signs and symptoms may be masked (5.4)
- Behavioral and mood disturbances: May Include euphoria, insomnia, mood swings, personality changes, severe depression, and psychosis. Existing conditions may be aggravated. (5.5)
- Decreases in bone density: Monitor bone density in patients receiving long-term corticosteroid therapy. (5.6)
- Ophthalmic effects: May include cataracts, infections and glaucoma. Monitor intraocular pressure if corticosteroid therapy is continued for more than 6 weeks.(5.7)
- Live or live attenuated vaccines: Do not administer to patients receiving immunosuppressive doses of corticosteroids. (5.8)
- Negative effects on growth and development: Monitor pediatric patients on long-term corticosteroid therapy. (5.9)
- Use in pregnancy: Fetal harm can occur with first trimester use. Apprise women of potential harm to the fetus. (5.10)
Adverse Reactions/Side Effects
Common adverse reactions for corticosteroids include fluid retention, alteration in glucose tolerance, elevation in blood pressure, behavioral and mood changes, increased appetite and weight gain. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Taro Pharmaceuticals U.S.A., Inc. at 1-888-827-6872 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
- Anticoagulant Agents: May enhance or diminish anticoagulant effects. Monitor coagulation indices. (7)
- Antidiabetic Agents: May increase blood glucose concentrations. Dose adjustments of antidiabetic agents may be required. (7)
- CYP 3A4 inducers and inhibitors: May, respectively, increase or decrease clearance of corticosteroids, necessitating dose adjustment.(7 )
- Cyclosporine: Increase in activity of both, cyclosporine and corticosteroid when administered concurrently. Convulsions have been reported with concurrent use. (7)
- NSAIDs including aspirin and salicylates: Increased risk of gastrointestinal side effects. (7)
See 17 for PATIENT COUNSELING INFORMATION.
Revised: 1/2019
Full Prescribing Information
1. Indications and Usage for Flo-Pred
Flo-Pred (prednisolone acetate oral suspension) is indicated in the treatment of the following diseases or conditions:
1.1 Allergic Conditions
Control of severe or incapacitating allergic conditions intractable to adequate trials of conventional treatment in adults and pediatric populations with:
- Atopic dermatitis
- Drug hypersensitivity reactions
- Seasonal or perennial allergic rhinitis
- Serum sickness
1.2 Dermatologic Diseases
- Bullous dermatitis herpetiformis
- Contact dermatitis
- Exfoliative erythroderma
- Mycosis fungoides
- Pemphigus
- Severe erythema multiforme (Stevens-Johnson syndrome)
1.3 Endocrine Conditions
- Congenital adrenal hyperplasia
- Hypercalcemia of malignancy
- Nonsuppurative thyroiditis
- Primary or secondary adrenocortical insufficiency: hydrocortisone or cortisone is the first choice: synthetic analogs may be used in conjunction with mineralocorticoids where applicable
1.5 Hematologic Diseases
- Acquired (autoimmune) hemolytic anemia
- Diamond-Blackfan anemia
- Idiopathic thrombocytopenic purpura in adults
- Pure red cell aplasia
- Secondary thrombocytopenia in adults
1.7 Nervous System Conditions
- Acute exacerbations of multiple sclerosis
- Cerebral edema associated with primary or metastatic brain tumor, craniotomy or head injury
1.8 Ophthalmic Conditions
- Sympathetic ophthalmia
- Uveitis and ocular inflammatory conditions unresponsive to topical steroids
1.10 Pulmonary Diseases
- Acute exacerbations of chronic obstructive pulmonary disease (COPD)
- Allergic bronchopulmonary aspergillosis
- Aspiration pneumonitis
- Asthma
- Fulminating or disseminated pulmonary tuberculosis when used concurrently with appropriate chemotherapy
- Hypersensitivity pneumonitis
- Idiopathic bronchiolitis obliterans with organizing pneumonia
- Idiopathic eosinophilic pneumonias
- Idiopathic pulmonary fibrosis
- Pneumocystis carinii pneumonia (PCP) associated with hypoxemia occurring in an HIV(+) individual who is also under treatment with appropriate anti-PCP antibiotics.
- Symptomatic sarcoidosis
1.11 Renal Conditions
- To induce a diuresis or remission of proteinuria in nephrotic syndrome, without uremia, of the idiopathic type or that due to lupus erythematosus
1.12 Rheumatologic Conditions
As adjunctive therapy for short-term administration (to tide the patient over an acute episode or exacerbation) in:
- Acute gouty arthritis
During an exacerbation or as maintenance therapy in selected cases of:
- Ankylosing spondylitis
- Dermatomyositis/polymyositis
- Polymyalgia rheumatica
- Psoriatic arthritis
- Relapsing polychondritis
- Rheumatoid arthritis, including juvenile rheumatoid arthritis (selected cases may require low dose maintenance therapy)
- Sjogren's syndrome
- Systemic lupus erythematosus
- Vasculitis
2. Flo-Pred Dosage and Administration
2.1 Recommended Dosing
Dosage of Flo-Pred should be individualized according to the severity of the disease and the response of the patient. For pediatric patients, the recommended dosage should be governed by the same considerations rather than strict adherence to the ratio indicated by age or body weight.
The initial dosage of Flo-Pred may vary from 5 mg to 60 mg per day depending on the specific disease entity being treated. In situations of less severity lower doses will generally suffice while in selected patients higher initial doses may be required. The initial dosage should be maintained or adjusted until a satisfactory response is noted. If after a reasonable period there is a lack of satisfactory clinical response, Flo-Pred should be discontinued and the patient transferred to other appropriate therapy. It should be emphasized that dosage requirements are variable and must be individualized on the basis of the disease under treatment and the response of the patient.
After a favorable response is noted, the proper maintenance dosage should be determined by decreasing the initial drug dosage in small decrements at appropriate time intervals until the lowest dosage which will maintain an adequate clinical response is reached. It should be kept in mind that constant monitoring is needed in regard to drug dosage. Included in the situations which may make dosage adjustments necessary are changes in clinical status secondary to remissions or exacerbations in the disease process, the patient's individual drug responsiveness, and the effect of patient exposure to stressful situations not directly related to the disease entity under treatment. In this latter situation it may be necessary to increase the dosage of Flo-Pred for a period of time consistent with the patient's condition. If a period of spontaneous remission occurs in a chronic condition, treatment should be discontinued. If after long-term therapy the drug is to be stopped, it is recommended that it be withdrawn gradually rather than abruptly.
2.2 Recommended Monitoring
Blood pressure, body weight, routine laboratory studies, including two-hour postprandial blood glucose and serum potassium, and a chest X-ray should be obtained at regular intervals during prolonged therapy. Upper GI X-rays are desirable in patients with known or suspected peptic ulcer disease.
2.3 Corticosteroid Comparison Chart
For the purpose of comparison, the following is the equivalent milligram dosage of the various glucocorticoids:
| Bethamethasone, 0.75 mg | Paramethasone, 2 mg |
| Cortisone, 25 mg | Prednisolone, 5 mg |
| Dexamethasone, 0.75 mg | Prednisone, 5 mg |
| Hydrocortisone, 20 mg | Triamcinolone, 4 mg |
| Methylprednisolone, 4 mg |
These dose relationships apply only to oral or intravenous administration of these compounds. When these substances or their derivatives are injected intramuscularly or into joint spaces, their relative properties may be greatly altered.
3. Dosage Forms and Strengths
Oral Suspension:
- 15 mg prednisolone (as 16.7 mg of prednisolone acetate) per 5 mL
4. Contraindications
Flo-Pred is contraindicated in patients who are hypersensitive to corticosteroids such as prednisolone, or any components of this product. Rare instances of anaphylactoid reactions have occurred in patients receiving corticosteroid therapy.
5. Warnings and Precautions
5.1 Alterations in Endocrine Function
Hypothalamic-pituitary-adrenal (HPA) axis suppression, Cushing's syndrome, and hyperglycemia. Monitor patients for these conditions with chronic use.
Corticosteroids can produce reversible HPA axis suppression with the potential for glucocorticosteroid insufficiency after withdrawal of treatment. Drug induced secondary adrenocortical insufficiency may be minimized by gradual reduction of dosage. This type of relative insufficiency may persist for months after discontinuation of therapy; therefore, in any situation of stress occurring during that period, hormone therapy should be reinstituted.
Since mineralocorticoid secretion may be impaired, salt and/or a mineralocorticoid should be administered concurrently. Mineralocorticoid supplementation is of particular importance in infancy.
Metabolic clearance of corticosteroids is decreased in hypothyroid patients and increased in hyperthyroid patients. Changes in thyroid status of the patient may necessitate adjustment in dosage.
5.2 Increased Risks Related to Infections
Corticosteroids may increase the risks related to infections with any pathogen, including viral, bacterial, fungal, protozoan, or helminthic infections. The degree to which the dose, route and duration of corticosteroid administration correlates with the specific risks of infection is not well characterized, however, with increasing doses of corticosteroids, the rate of occurrence of infectious complications increases.
Corticosteroids may mask some signs of infection and may reduce resistance to new infections.
Corticosteroids may exacerbate infections and increase risk of disseminated infection.
The use of Flo-Pred in active tuberculosis should be restricted to those cases of fulminating or disseminated tuberculosis in which the corticosteroid is used for the management of the disease in conjunction with an appropriate antituberculous regimen.
Chickenpox and measles can have a more serious or even fatal course in non-immune children or adults on corticosteroids. In children or adults who have not had these diseases, particular care should be taken to avoid exposure. If a patient is exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If patient is exposed to measles, prophylaxis with pooled intramuscular immunoglobulin (IG) may be indicated. If chickenpox develops, treatment with antiviral agents may be considered.
Corticosteroids should be used with great care in patients with known or suspected Strongyloides (threadworm) infestation. In such patients, corticosteroid-induced immunosuppression may lead to Strongyloides hyperinfection and dissemination with widespread larval migration, often accompanied by severe enterocolitis and potentially fatal gram-negative septicemia.
Corticosteroids may exacerbate systemic fungal infections and therefore should not be used in the presence of such infections unless they are needed to control drug reactions.
Corticosteroids may increase risk of reactivation or exacerbation of latent infection.
If corticosteroids are indicated in patients with latent tuberculosis or tuberculin reactivity, close observation is necessary as reactivation of the disease may occur. During prolonged corticosteroid therapy, these patients should receive chemoprophylaxis.
Corticosteroids may activate latent amebiasis. Therefore, it is recommended that latent or active amebiasis be ruled out before initiating corticosteroid therapy in any patient who has spent time in the tropics or in any patient with unexplained diarrhea.
Corticosteroids should not be used in cerebral malaria.
5.3 Alterations in Cardiovascular/Renal Function
Corticosteroids can cause elevation of blood pressure, salt and water retention, and increased excretion of potassium and calcium. These effects are less likely to occur with the synthetic derivatives except when used in large doses. Dietary salt restriction and potassium supplementation may be necessary. These agents should be used with caution in patients with hypertension, congestive heart failure, or renal insufficiency.
Literature reports suggest an association between use of corticosteroids and left ventricular free wall rupture after a recent myocardial infarction; therefore, therapy with corticosteroids should be used with caution in these patients.
5.4 Use in Patients with Gastrointestinal Disorders
There is an increased risk of gastrointestinal perforation in patients with certain GI disorders. Signs of GI perforation, such as peritoneal irritation, may be masked in patients receiving corticosteroids.
Corticosteroids should be used with caution if there is a probability of impending perforation, abscess or other pyogenic infections; diverticulitis; fresh intestinal anastomoses; and active or latent peptic ulcer.
5.5 Behavioral and Mood Disturbances
Corticosteroid use may be associated with central nervous system effects ranging from euphoria, insomnia, mood swings, personality changes, and severe depression, to frank psychotic manifestations. Also, existing emotional instability or psychotic tendencies may be aggravated by corticosteroids.
5.6 Decrease in Bone Density
Corticosteroids decrease bone formation and increase bone resorption both through their effect on calcium regulation (i.e., decreasing absorption and increasing excretion) and inhibition of osteoblast function. This, together with a decrease in the protein matrix of the bone secondary to an increase in protein catabolism, and reduced sex hormone production, may lead to inhibition of bone growth in children and adolescents and the development of osteoporosis at any age. Special consideration should be given to patients at increased risk of osteoporosis (i.e., postmenopausal women) before initiating corticosteroid therapy and bone density should be monitored in patients on long-term corticosteroid therapy.
5.7 Ophthalmic Effects
Prolonged use of corticosteroids may produce posterior subcapsular cataracts, glaucoma with possible damage to the optic nerves, and may enhance the establishment of secondary ocular infections due to fungi or viruses.
The use of oral corticosteroids is not recommended in the treatment of optic neuritis and may lead to an increase in the risk of new episodes.
Intraocular pressure may become elevated in some individuals. If steroid therapy is continued for more than 6 weeks, intraocular pressure should be monitored.
Patients with Ocular Herpes Simplex
Corticosteroids should be used cautiously in patients with ocular herpes simplex because of possible corneal perforation. Corticosteroids should not be used in active ocular herpes simplex.
5.8 Vaccination
Administration of live or live attenuated vaccines is contraindicated in patients receiving immunosuppressive doses of corticosteroids. Killed or inactivated vaccines may be administered, however, the response to such vaccines can not be predicted. Immunization procedures may be undertaken in patients who are receiving corticosteroids as replacement therapy, e.g., for Addison's disease.
While on corticosteroid therapy, patients should not be vaccinated against smallpox. Other immunization procedures should not be undertaken in patients who are on corticosteroids, especially on high dose, because of possible hazards of neurological complications and a lack of antibody response.
5.9 Effect on Growth and Development
Long-term use of corticosteroids can have negative effects on growth and development in children.
Growth and development of pediatric patients on prolonged corticosteroid therapy should be carefully monitored.
5.10 Use in Pregnancy
Prednisolone can cause fetal harm when administered to a pregnant woman. Human and animal studies suggest that use of corticosteroids during the first trimester of pregnancy is associated with an increased risk of orofacial clefts, intrauterine growth restriction and decreased birth weight. If this drug is used during pregnancy, or if the patient becomes pregnant while using this drug, the patient should be apprised of the potential hazard to the fetus. [see Use in Specific Populations(8.1)].
5.11 Neuromuscular Effects
Although controlled clinical trials have shown corticosteroids to be effective in speeding the resolution of acute exacerbations of multiple sclerosis, they do not show that they affect the ultimate outcome or natural history of the disease. The studies do show that relatively high doses of corticosteroids are necessary to demonstrate a significant effect. [see Dosage and Administration (2)].
An acute myopathy has been observed with the use of high doses of corticosteroids, most often occurring in patients with disorders of neuromuscular transmission (e.g., myasthenia gravis), or in patients receiving concomitant therapy with neuromuscular blocking drugs (e.g., pancuronium). This acute myopathy is generalized, may involve ocular and respiratory muscles, and may result in quadriparesis. Elevation of creatine kinase may occur. Clinical improvement or recovery after stopping corticosteroids may require weeks to years.
6. Adverse Reactions/Side Effects
Common adverse reactions for corticosteroids include fluid retention, alteration in glucose tolerance, elevation in blood pressure, behavioral and mood changes, increased appetite and weight gain.
Allergic Reactions: Anaphylactoid reaction, anaphylaxis, angioedema
Cardiovascular: Bradycardia, cardiac arrest, cardiac arrhythmias, cardiac enlargement, circulatory collapse, congestive heart failure, fat embolism, hypertension, hypertrophic cardiomyopathy in premature infants, myocardial rupture following recent myocardial infarction, pulmonary edema, syncope, tachycardia, thromboembolism, thrombophlebitis, vasculitis
Dermatologic: Acne, allergic dermatitis, cutaneous and subcutaneous atrophy, dry scalp, edema, facial erythema, hyper or hypo-pigmentation, impaired wound healing, increased sweating, petechiae and ecchymoses, rash, sterile abscess, striae, suppressed reactions to skin tests, thin fragile skin, thinning scalp hair, urticaria
Endocrine: Abnormal fat deposits, decreased carbohydrate tolerance, development of Cushingoid state, hirsutism, manifestations of latent diabetes mellitus and increased requirements for insulin or oral hypoglycemic agents in diabetics, menstrual irregularities, moon facies, secondary adrenocortical and pituitary unresponsiveness (particularly in times of stress, as in trauma, surgery or illness), suppression of growth in children
Fluid and Electrolyte Disturbances: Fluid retention, potassium loss, hypertension, hypokalemic alkalosis, sodium retention
Gastrointestinal: Abdominal distention, elevation in serum liver enzymes levels (usually reversible upon discontinuation), hepatomegaly, hiccups, malaise, nausea, pancreatitis, peptic ulcer with possible perforation and hemorrhage, ulcerative esophagitis
General: Increased appetite and weight gain
Metabolic: Negative nitrogen balance due to protein catabolism
Musculoskeletal: Aseptic necrosis of femoral and humeral heads, charcot-like arthropathy, loss of muscle mass, muscle weakness, osteoporosis, pathologic fracture of long bones, steroid myopathy, tendon rupture, vertebral compression fractures
Neurological: Arachnoiditis, convulsions, depression, emotional instability, euphoria, headache, increased intracranial pressure with papilledema (pseudo-tumor cerebri) usually following discontinuation of treatment, insomnia, meningitis, mood swings, neuritis, neuropathy, paraparesis/paraplegia, paresthesia, personality changes, sensory disturbances, vertigo
Ophthalmic: Exophthalmos, glaucoma, increased intraocular pressure, and posterior subcapsular cataracts
Reproductive: Alteration in motility and number of spermatozoa
7. Drug Interactions
- Aminoglutethimide: Aminoglutethimide may lead to loss of corticosteroid-induced adrenal suppression.
- Amphotericin B: There have been cases reported in which concomitant use of Amphotericin B and hydrocortisone was followed by cardiac enlargement and congestive heart failure (see also Potassium depleting agents).
- Anticholinesterase agents: Concomitant use of anticholinesterase agents and corticosteroids may produce severe weakness in patients with myasthenia gravis. If possible, anticholinesterase agents should be withdrawn at least 24 hours before initiating corticosteroid therapy.
- Anticoagulant agents: Coadministration of corticosteroids and warfarin usually results in inhibition of response to warfarin, although there have been some conflicting reports. Therefore, coagulation indices should be monitored frequently to maintain the desired anticoagulant effect.
- Antidiabetic agents: Because corticosteroids may increase blood glucose concentrations, dosage adjustments of antidiabetic agents may be required.
- Antitubercular drugs: Serum concentrations of isoniazid may be decreased.
- CYP 3A4 inducers (e.g., barbiturates, phenytoin, carbamazepine, and rifampin): Drugs such as barbiturates, phenytoin, ephedrine, and rifampin, which induce hepatic microsomal drug metabolizing enzyme activity may enhance metabolism of prednisolone and require that the dosage of Flo-Pred be increased.
- CYP 3A4 inhibitors (e.g., ketoconazole, macrolide antibiotics): Ketoconazole has been reported to decrease the metabolism of certain corticosteroids by up to 60% leading to an increased risk of corticosteroid side effects.
- Cholestyramine: Cholestyramine may increase the clearance of corticosteroids.
- Cyclosporine: Increased activity of both cyclosporine and corticosteroids may occur when the two are used concurrently. Convulsions have been reported with concurrent use.
- Digitalis: Patients on digitalis glycosides may be at increased risk of arrhythmias due to hypokalemia.
- Estrogens, including oral contraceptives: Estrogens may decrease the hepatic metabolism of certain corticosteroids thereby increasing their effect.
- NSAlDs including aspirin and salicylates: Concomitant use of aspirin or other non-steroidal anti-inflammatory agents and corticosteroids increases the risk of gastrointestinal side effects. Aspirin should be used cautiously in conjunction with corticosteroids in hypoprothrombinemia. The clearance of salicylates may be increased with concurrent use of corticosteroids.
- Potassium depleting agents (e.g., diuretics, Amphotericin B): When corticosteroids are administered concomitantly with potassium-depleting agents, patients should be observed closely for development of hypokalemia.
- Skin tests: Corticosteroids may suppress reactions to skin tests.
- Toxoids and live or inactivated vaccines: Due to inhibition of antibody response, patients on prolonged corticosteroid therapy may exhibit a diminished response to toxoids and live or inactivated vaccines. Corticosteroids may also potentiate the replication of some organisms contained in live attenuated vaccines.
8. Use In Specific Populations
8.3 Nursing Mothers
Prednisolone is secreted in human milk. Reports suggest that prednisolone concentrations in human milk are 5 to 25% of maternal serum levels, and that total infant daily doses are small, about 0.14% of the maternal daily dose. The risk of infant exposure to prednisolone through breast milk should be weighed against the known benefits of breastfeeding for both the mother and baby.
Caution should be exercised when prednisolone is administered to a nursing woman. If prednisolone must be prescribed to a breastfeeding mother, the lowest dose should be prescribed to achieve the desired clinical effect. High doses of corticosteroids for long periods could potentially produce problems in infant growth and development and interfere with endogenous corticosteroid production.
Breastfeeding women using corticosteroids should be encouraged to take their dose immediately after breastfeeding at the time of day when the baby usually has the longest interval between feeds. This will minimize infant exposure to drug.
8.4 Pediatric Use
The efficacy and safety of prednisolone in the pediatric population are based on the well-established course of effect of corticosteroids which is similar in pediatric and adult populations. Published studies provide evidence of efficacy and safety in pediatric patients for the treatment of nephrotic syndrome (>2 years of age), and aggressive lymphomas and leukemias (>1 month of age). However, some of these conclusions and other indications for pediatric use of corticosteroid, e.g., severe asthma and wheezing, are based on adequate and well-controlled trials conducted in adults, on the premises that the course of the diseases and their pathophysiology are considered to be substantially similar in both populations.
The adverse effects of prednisolone in pediatric patients are similar to those in adults [see Adverse Reactions (6)]. Like adults, pediatric patients should be carefully observed with frequent measurements of blood pressure, weight, height, intraocular pressure, and clinical evaluation for the presence of infection, psychosocial disturbances, thromboembolism, peptic ulcers, cataracts, and osteoporosis. Children who are treated with corticosteroids by any route, including systemically administered corticosteroids, may experience a decrease in their growth velocity. This negative impact of corticosteroids on growth has been observed at low systemic doses and in the absence of laboratory evidence of HPA axis suppression (i.e., cosyntropin stimulation and basal cortisol plasma levels).
Growth velocity may therefore be a more sensitive indicator of systemic corticosteroid exposure in children than some commonly used tests of HPA axis function. The linear growth of children treated with corticosteroids by any route should be monitored, and the potential growth effects of prolonged treatment should be weighed against clinical benefits obtained and the availability of other treatment alternatives. In order to minimize the potential growth effects of corticosteroids, children should be titrated to the lowest effective dose.
8.5 Geriatric Use
No overall differences in safety or effectiveness were observed between elderly subjects and younger subjects, and other reported clinical experience with prednisolone has not identified differences in responses between the elderly and younger patients. However, the incidence of corticosteroid-induced side effects may be increased in geriatric patients and are dose-related. Osteoporosis is the most frequently encountered complication, which occurs at a higher incidence rate in corticosteroid-treated geriatric patients as compared to younger populations and in age-matched controls. Losses of bone mineral density appear to be greatest early on in the course of treatment and may recover over time after steroid withdrawal or use of lower doses (i.e., ≤ 5 mg/day). Prednisolone doses of 7.5 mg/day or higher have been associated with an increased relative risk of both vertebral and nonvertebral fractures, even in the presence of higher bone density compared to patients with involution osteoporosis.
Routine screening of geriatric patients, including regular assessments of bone mineral density and institution of fracture prevention strategies, along with regular review of prednisolone indication should be undertaken to minimize complications and keep the prednisolone dose at the lowest acceptable level. Co-administration of certain bisphosphonates have been shown to retard the rate of bone loss in corticosteroid-treated males and postmenopausal females, and these agents are recommended in the prevention and treatment of corticosteroid-induced osteoporosis.
It has been reported that equivalent weight-based doses yield higher total and unbound prednisolone plasma concentrations and reduced renal and non-renal clearance in elderly patients compared to younger populations. Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
10. Overdosage
The effects of accidental ingestion of large quantities of prednisolone over a very short period of time have not been reported, but prolonged use of the drug can produce mental symptoms, moon face, abnormal fat deposits, fluid retention, excessive appetite, weight gain, hypertrichosis, acne, striae, ecchymosis, increased sweating, pigmentation, dry scaly skin, thinning scalp hair, increased blood pressure, tachycardia, thrombophlebitis, decreased resistance to infection, negative nitrogen balance with delayed bone and wound healing, headache, weakness, menstrual disorders, accentuated menopausal symptoms, neuropathy, fractures, osteoporosis, peptic ulcer, decreased glucose tolerance, hypokalemia, and adrenal insufficiency. Hepatomegaly and abdominal distention have been observed in children.
Treatment of acute overdosage is by immediate gastric lavage or emesis followed by supportive and symptomatic therapy. For chronic overdosage in the face of severe disease requiring continuous steroid therapy the dosage of prednisolone may be reduced only temporarily, or alternate day treatment may be introduced.
11. Flo-Pred Description
Flo-Pred (prednisolone acetate oral suspension) contains prednisolone which is the acetate ester of the glucocorticoid prednisolone. Glucocorticoids are adrenocortical steroids, both naturally occurring and synthetic, which are readily absorbed from the gastrointestinal tract.
Prednisolone acetate is a white to off-white in color, odorless, crystalline powder. It is insoluble in water, slightly soluble in acetone, in alcohol and in chloroform.
The chemical name for prednisolone acetate is 11β 17,21-trihydroxypregna-1,4-diene-3,20-dione 21-acetate. Its molecular weight is 402.49. The molecular formula is C23H30O6 and the structural formula is:
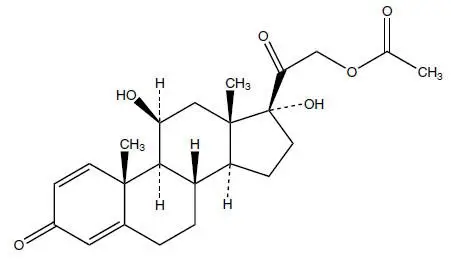
Flo-Pred (prednisolone acetate oral suspension) is a viscous milky white formulation containing 15 mg of prednisolone (as 16.7 mg of prednisolone acetate) in each 5 mL. Flo-Pred is a spill resistant system that delivers semi-solid products for oral administration from a squeezable container. This system comprises of a liquid base and a thickening agent that ensures product homogeneity during storage. Butylparaben, 0.04% is added as a preservative. It also contains carbomer 934P, disodium edetate, glycerin, masking agent, poloxamer 188, propylene glycol, purified water, sodium hydroxide, sorbitol crystalline, sucralose liquid concentrate and cherry flavor.
12. Flo-Pred - Clinical Pharmacology
12.1 Mechanism of Action
Naturally occurring glucocorticoids (hydrocortisone and cortisone), which also have salt-retaining properties, are used as replacement therapy in adrenocortical deficiency states. Their synthetic analogs such as prednisolone are primarily used for their potent anti-inflammatory effects in disorders of many organ systems.
Glucocorticoids such as prednisolone cause profound and varied metabolic effects. In addition, they modify the body's immune responses to diverse stimuli.
Prednisolone is a synthetic adrenocortical steroid drug with predominantly glucocorticoid properties. Some of these properties reproduce the physiological actions of endogenous glucocorticosteroids, but others do not necessarily reflect any of the adrenal hormones' normal functions; they are seen only after administration of large therapeutic doses of the drug. The pharmacological effects of prednisolone which are due to its glucocorticoid properties include: promotion of gluconeogenesis; increased deposition of glycogen in the liver; inhibition of the utilization of glucose; anti-insulin activity; increased catabolism of protein; increased lipolysis; stimulation of fat synthesis and storage; increased glomerular filtration rate and resulting increase in urinary excretion of urate (creatinine excretion remains unchanged); and increased calcium excretion.
Depressed production of eosinophils and lymphocytes occurs, but erythropoiesis and production of polymorphonuclear leukocytes are stimulated. Inflammatory processes (edema, fibrin deposition, capillary dilatation, migration of leukocytes and phagocytosis) and the later stages of wound healing (capillary proliferation, deposition of collagen, cicatrization) are inhibited.
Prednisolone can stimulate secretion of various components of gastric juice. Suppression of the production of corticotropin may lead to suppression of endogenous corticosteroids. Prednisolone has slight mineralocorticoid activity, whereby entry of sodium into cells and loss of intracellular potassium is stimulated. This is particularly evident in the kidney, where rapid ion exchange leads to sodium retention and hypertension.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Flo-Pred was not formally evaluated in carcinogenicity studies. Review of the published literature identified carcinogenicity studies of prednisolone at doses which were less than the typical clinical doses. In a 2-year study, male Sprague-Dawley rats administered prednisolone in drinking water at a dose of 368 mcg/kg/day (equivalent to 3.5 mg/day in a 60 kg individual based on a mg/m2 body surface area comparison) developed increased incidences of hepatic adenomas. Lower doses were not studied and therefore a no effect level could not be identified. In an 18-month study, intermittent oral gavage administration of prednisolone did not induce tumors in female Sprague-Dawley rats when given 1, 2, 4.5 or 9 times per month at 3 mg/kg prednisolone (equivalent to 29 mg in a 60 kg individual based on a mg/m2 body surface area comparison).
Flo-Pred was not formally evaluated for genotoxicity. However, in published studies prednisolone was not mutagenic with or without metabolic activation in the Ames bacterial reverse mutation assay using Salmonella typhimurium and Escherichia coli, or in a mammalian cell gene mutation assay using mouse lymphoma L5178Y cells, according to current evaluation standards. In a published chromosomal aberration study in Chinese Hamster Lung (CHL) cells, a slight increase was seen in the incidence of structural chromosomal aberrations with metabolic activation at the highest concentration tested, however, the effect appears to be equivocal. Prednisolone was not genotoxic in an in vivo micronucleaus assay in the mouse though the study design did not meet current criteria.
Flo-Pred was not formally evaluated in fertility studies. However, menstrual irregularities have been described with clinical use [see Adverse Reactions (6)].
16. How is Flo-Pred supplied
Flo-Pred (prednisolone acetate oral suspension) is a cherry flavored milky white viscous liquid containing 16.7 mg of prednisolone acetate (equivalent to 15 mg prednisolone) in each 5 mL of formulation and is supplied as follows:
37 mL (NDC 51672-1338-5) for Professional Samples
52 mL (NDC 51672-1338-3)
65 mL (NDC 51672-1338-6)
17. Patient Counseling Information
Patients should be warned not to discontinue the use of Flo-Pred abruptly or without medical supervision, to advise any medical attendants that they are taking it, and to seek medical advice at once should they develop fever or other signs of infection. Patients should be told to take Flo-Pred exactly as prescribed, follow the instructions on the prescription label, and not stop taking Flo-Pred without first checking with their healthcare providers, as there may be a need for gradual dose reduction.
Patients should discuss with their physician if they have had recent or ongoing infections or if they have recently received a vaccine.
Patients who are on immunosuppressant doses of corticosteroids should be warned to avoid exposure to chickenpox or measles. Patients should also be advised that if they are exposed, medical advice should be sought without delay.
There are a number of medicines that can interact with Flo-Pred. Patients should inform their healthcare provider of all the medicines they are taking, including over-the-counter and prescription medicines (such as phenytoin, diuretics, digitalis or digoxin, rifampin, amphotericin B, cyclosporine, insulin or diabetes medicines, ketoconazole, estrogens including birth control pills and hormone replacement therapy, blood thinners such as warfarin, aspirin or other NSAIDs, barbiturates), dietary supplements, and herbal products. If patients are taking any of these drugs, alternate therapy, dosage adjustment, and/or special testing may be needed during the treatment.
For missed doses, patients should be told to take the missed dose as soon as they remember. If it is almost time for the next dose, the missed dose should be skipped and the medicine taken at the next regularly scheduled time. Patients should not take an extra dose to make up for the missed dose.
Patients should be told to take Flo-Pred with food to avoid GI irritation.
Patients should be advised of common adverse reactions that could occur with Flo-Pred use to include fluid retention, alteration in glucose tolerance, elevation in blood pressure, behavioral and mood changes, increased appetite and weight gain.

| FLO-PRED
prednisolone acetate suspension |
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||
| Labeler - Taro Pharmaceuticals U.S.A., Inc. (145186370) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Taro Pharmaceuticals Inc. | 206263295 | MANUFACTURE(51672-1338) | |
