Drug Detail:Neupogen (Filgrastim [ fil-gras-tim ])
Drug Class: Colony stimulating factors
Highlights of Prescribing Information
NEUPOGEN® (filgrastim) injection, for subcutaneous or intravenous use
Initial U.S. Approval: 1991
Recent Major Changes
Warnings and Precautions: Glomerulonephritis (5.5) 07/2015
Indications and Usage for Neupogen
NEUPOGEN is a leukocyte growth factor indicated to
- Decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever (1.1)
- Reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML) (1.2)
- Reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g.‚ febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation (BMT) (1.3)
- Mobilize autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis (1.4)
- Reduce the incidence and duration of sequelae of severe neutropenia (e.g.‚ fever‚ infections‚ oropharyngeal ulcers) in symptomatic patients with congenital neutropenia‚ cyclic neutropenia‚ or idiopathic neutropenia (1.5)
- Increase survival in patients acutely exposed to myelosuppressive doses of radiation (Hematopoietic Syndrome of Acute Radiation Syndrome) (1.6)
Neupogen Dosage and Administration
- Patients with cancer receiving myelosuppressive chemotherapy or induction and/or consolidation chemotherapy for AML
○ Recommended starting dose is 5 mcg/kg/day subcutaneous injection, short intravenous infusion (15 to 30 minutes), or continuous intravenous infusion. See Full Prescribing Information for recommended dosage adjustments and timing of administration (2.1)
- Patients with cancer undergoing bone marrow transplantation
○ 10 mcg/kg/day given as an intravenous infusion no longer than 24 hours. See Full Prescribing Information for recommended dosage adjustments and timing of administration (2.2)
- Patients undergoing autologous peripheral blood progenitor cell collection and therapy
○ 10 mcg/kg/day subcutaneous injection (2.3)
○ Administer for at least 4 days before first leukapheresis procedure and continue until last leukapheresis (2.3)
- Patients with congenital neutropenia
○ Recommended starting dose is 6 mcg/kg subcutaneous injection twice daily (2.4)
- Patients with cyclic or idiopathic neutropenia
○ Recommended starting dose is 5 mcg/kg subcutaneous injection daily (2.4)
- Patients acutely exposed to myelosuppressive doses of radiation
○ 10 mcg/kg/day subcutaneous injection (2.5)
Dosage Forms and Strengths
Vial
- Injection: 300 mcg/mL in a single-dose vial (3)
- Injection: 480 mcg/1.6 mL in a single-dose vial (3)
Prefilled Syringe
- Injection: 300 mcg/0.5 mL in a single-dose prefilled syringe (3)
- Injection: 480 mcg/0.8 mL in a single-dose prefilled syringe (3)
Contraindications
- Patients with a history of serious allergic reactions to human granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim. (4)
Warnings and Precautions
- Fatal splenic rupture: Evaluate patients who report left upper abdominal or shoulder pain for an enlarged spleen or splenic rupture. (5.1)
- Acute respiratory distress syndrome (ARDS): Evaluate patients who develop fever and lung infiltrates or respiratory distress for ARDS. Discontinue NEUPOGEN in patients with ARDS. (5.2)
- Serious allergic reactions, including anaphylaxis: Permanently discontinue NEUPOGEN in patients with serious allergic reactions. (5.3)
- Fatal sickle cell crises: Have occurred. (5.4)
- Glomerulonephritis: Evaluate and consider dose-reduction or interruption of NEUPOGEN if causality is likely. (5.5)
Adverse Reactions/Side Effects
Most common adverse reactions in patients:
- With nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs (≥ 5% difference in incidence compared to placebo) are pyrexia, pain, rash, cough, and dyspnea. (6.1)
- With AML (≥ 2% difference in incidence) are pain, epistaxis and rash. (6.1)
- With nonmyeloid malignancies undergoing myeloablative chemotherapy followed by BMT (≥ 5% difference in incidence) is rash. (6.1)
- Undergoing peripheral blood progenitor cell mobilization and collection (≥ 5% incidence) are bone pain, pyrexia and headache. (6.1)
- With severe chronic neutropenia (SCN) (≥ 5% difference in incidence) are pain, anemia, epistaxis, diarrhea, hypoesthesia and alopecia. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Amgen Medical Information at 1-800-77-AMGEN (1-800-772-6436) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Use In Specific Populations
- NEUPOGEN should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. (8.1)
- It is not known whether NEUPOGEN is excreted in human milk. (8.3)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 6/2016
Full Prescribing Information
1. Indications and Usage for Neupogen
1.1 Patients with Cancer Receiving Myelosuppressive Chemotherapy
NEUPOGEN is indicated to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs associated with a significant incidence of severe neutropenia with fever [see Clinical Studies (14.1)].
1.2 Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
NEUPOGEN is indicated for reducing the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML) [see Clinical Studies (14.2)].
1.3 Patients with Cancer Undergoing Bone Marrow Transplantation
NEUPOGEN is indicated to reduce the duration of neutropenia and neutropenia-related clinical sequelae‚ e.g.‚ febrile neutropenia, in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by bone marrow transplantation [see Clinical Studies (14.3)].
1.4 Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
NEUPOGEN is indicated for the mobilization of autologous hematopoietic progenitor cells into the peripheral blood for collection by leukapheresis [see Clinical Studies (14.4)].
1.5 Patients with Severe Chronic Neutropenia
NEUPOGEN is indicated for chronic administration to reduce the incidence and duration of sequelae of neutropenia (e.g.‚ fever‚ infections‚ oropharyngeal ulcers) in symptomatic patients with congenital neutropenia‚ cyclic neutropenia‚ or idiopathic neutropenia [see Clinical Studies (14.5)].
2. Neupogen Dosage and Administration
2.1 Dosage in Patients with Cancer Receiving Myelosuppressive Chemotherapy or Induction and/or Consolidation Chemotherapy for AML
The recommended starting dosage of NEUPOGEN is 5 mcg/kg/day‚ administered as a single daily injection by subcutaneous injection‚ by short intravenous infusion (15 to 30 minutes)‚ or by continuous intravenous infusion. Obtain a complete blood count (CBC) and platelet count before instituting NEUPOGEN therapy and monitor twice weekly during therapy. Consider dose escalation in increments of 5 mcg/kg for each chemotherapy cycle‚ according to the duration and severity of the absolute neutrophil count (ANC) nadir. Recommend stopping NEUPOGEN if the ANC increases beyond 10‚000/mm3 [see Warnings and Precautions (5.10)].
Administer NEUPOGEN at least 24 hours after cytotoxic chemotherapy. Do not administer NEUPOGEN within the 24-hour period prior to chemotherapy [see Warnings and Precautions (5.13)]. A transient increase in neutrophil count is typically seen 1 to 2 days after initiation of NEUPOGEN therapy. Therefore, to ensure a sustained therapeutic response‚ administer NEUPOGEN daily for up to 2 weeks or until the ANC has reached 10‚000/mm3 following the expected chemotherapy-induced neutrophil nadir. The duration of NEUPOGEN therapy needed to attenuate chemotherapy-induced neutropenia may be dependent on the myelosuppressive potential of the chemotherapy regimen employed.
2.2 Dosage in Patients with Cancer Undergoing Bone Marrow Transplantation
The recommended dosage of NEUPOGEN following bone marrow transplantation (BMT) is 10 mcg/kg/day given as an intravenous infusion no longer than 24 hours. Administer the first dose of NEUPOGEN at least 24 hours after cytotoxic chemotherapy and at least 24 hours after bone marrow infusion. Monitor CBCs and platelet counts frequently following marrow transplantation.
During the period of neutrophil recovery‚ titrate the daily dosage of NEUPOGEN against the neutrophil response (see Table 1).
| Absolute Neutrophil Count | NEUPOGEN Dosage Adjustment |
| When ANC greater than 1000/mm3 for 3 consecutive days | Reduce to 5 mcg/kg/daya |
| Then, if ANC remains greater than 1000/mm3
for 3 more consecutive days | Discontinue NEUPOGEN |
| Then, if ANC decreases to less than 1000/mm3 | Resume at 5 mcg/kg/day |
a If ANC decreases to less than 1000/mm3 at any time during the 5 mcg/kg/day administration‚ increase NEUPOGEN to 10 mcg/kg/day‚ and then follow the above steps.
2.3 Dosage in Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
The recommended dosage of NEUPOGEN for the mobilization of autologous peripheral blood progenitor cells (PBPC) is 10 mcg/kg/day given by subcutaneous injection. Administer NEUPOGEN for at least 4 days before the first leukapheresis procedure and continue until the last leukapheresis. Although the optimal duration of NEUPOGEN administration and leukapheresis schedule have not been established‚ administration of NEUPOGEN for 6 to 7 days with leukaphereses on days 5‚ 6‚ and 7 was found to be safe and effective [see Clinical Studies (14.4)]. Monitor neutrophil counts after 4 days of NEUPOGEN‚ and discontinue NEUPOGEN if the white blood cell (WBC) count rises to greater than 100‚000/mm3.
2.4 Dosage in Patients with Severe Chronic Neutropenia
Prior to starting NEUPOGEN in patients with suspected chronic neutropenia, confirm the diagnosis of severe chronic neutropenia (SCN) by evaluating serial CBCs with differential and platelet counts‚ and evaluating bone marrow morphology and karyotype. The use of NEUPOGEN prior to confirmation of a correct diagnosis of SCN may impair diagnostic efforts and may thus impair or delay evaluation and treatment of an underlying condition‚ other than SCN‚ causing the neutropenia.
The recommended starting dosage in patients with Congenital Neutropenia is 6 mcg/kg as a twice daily subcutaneous injection and the recommended starting dosage in patients with Idiopathic or Cyclic Neutropenia is 5 mcg/kg as a single daily subcutaneous injection.
Dosage Adjustments in Patients with Severe Chronic Neutropenia
Chronic daily administration is required to maintain clinical benefit. Individualize the dosage based on the patient’s clinical course as well as ANC. In the SCN postmarketing surveillance study, the reported median daily doses of NEUPOGEN were: 6 mcg/kg (congenital neutropenia), 2.1 mcg/kg (cyclic neutropenia), and 1.2 mcg/kg (idiopathic neutropenia). In rare instances, patients with congenital neutropenia have required doses of NEUPOGEN greater than or equal to 100 mcg/kg/day.
Monitor CBCs for Dosage Adjustments
During the initial 4 weeks of NEUPOGEN therapy and during the 2 weeks following any dosage adjustment‚ monitor CBCs with differential and platelet counts. Once a patient is clinically stable‚ monitor CBCs with differential and platelet counts monthly during the first year of treatment. Thereafter, if the patient is clinically stable, less frequent routine monitoring is recommended.
2.5 Dosage in Patients Acutely Exposed to Myelosuppressive Doses of Radiation (Hematopoietic Syndrome of Acute Radiation Syndrome)
The recommended dose of NEUPOGEN is 10 mcg/kg as a single daily subcutaneous injection for patients exposed to myelosuppressive doses of radiation. Administer NEUPOGEN as soon as possible after suspected or confirmed exposure to radiation doses greater than 2 gray (Gy).
Estimate a patient’s absorbed radiation dose (i.e., level of radiation exposure) based on information from public health authorities, biodosimetry if available, or clinical findings such as time to onset of vomiting or lymphocyte depletion kinetics.
Obtain a baseline CBC and then serial CBCs approximately every third day until the ANC remains greater than 1,000/mm3 for 3 consecutive CBCs. Do not delay administration of NEUPOGEN if a CBC is not readily available.
Continue administration of NEUPOGEN until the ANC remains greater than 1,000/mm3 for 3 consecutive CBCs or exceeds 10,000/mm3 after a radiation-induced nadir.
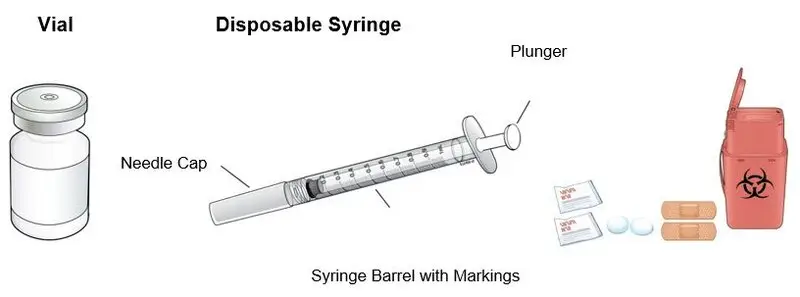
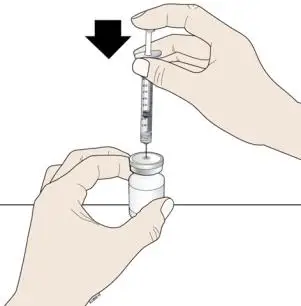
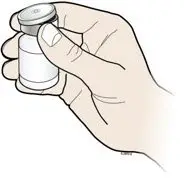
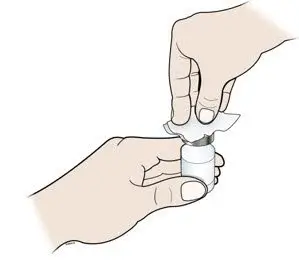
2.6 Important Administration Instructions
NEUPOGEN is supplied in single-dose vials (for subcutaneous use or intravenous infusion) and single-dose prefilled syringes (for subcutaneous use) [see Dosage Forms and Strengths (3)]. Prior to use‚ remove the vial or prefilled syringe from the refrigerator and allow NEUPOGEN to reach room temperature for a minimum of 30 minutes and a maximum of 24 hours. Discard any vial or prefilled syringe left at room temperature for greater than 24 hours. Visually inspect NEUPOGEN for particulate matter and discoloration prior to administration (the solution is clear and colorless). Do not administer NEUPOGEN if particulates or discoloration are observed.
Discard unused portion of NEUPOGEN in vials or prefilled syringes; do not re-enter the vial. Do not save unused drug for later administration.
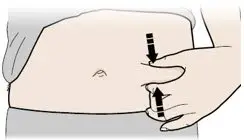
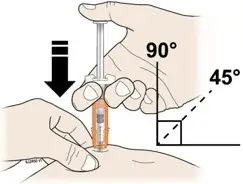
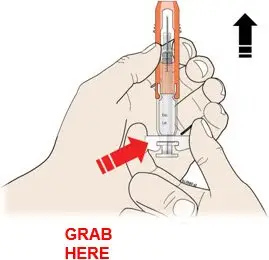
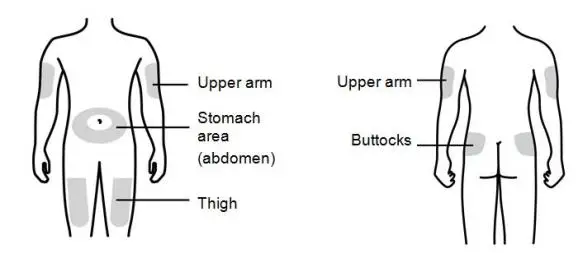
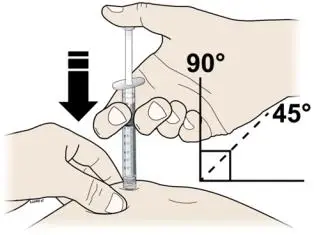
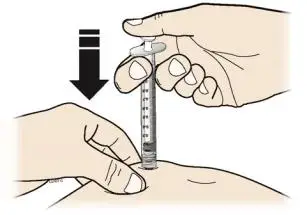
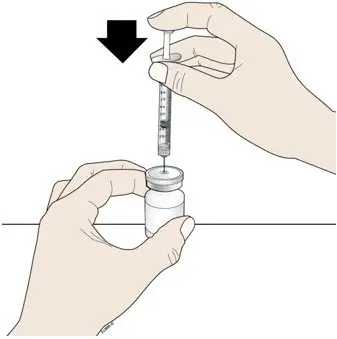
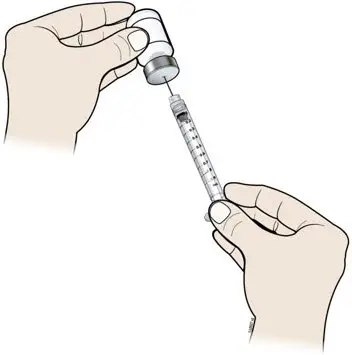
Subcutaneous Injection
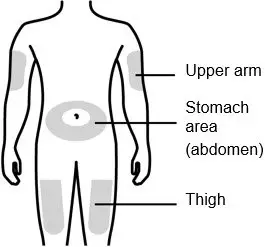
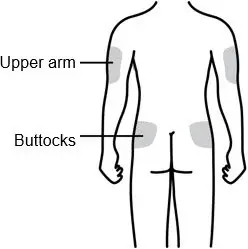
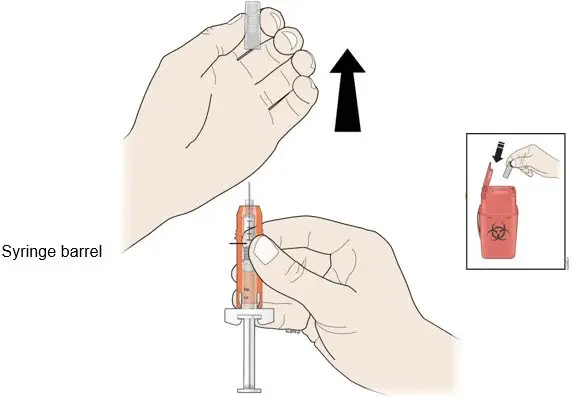
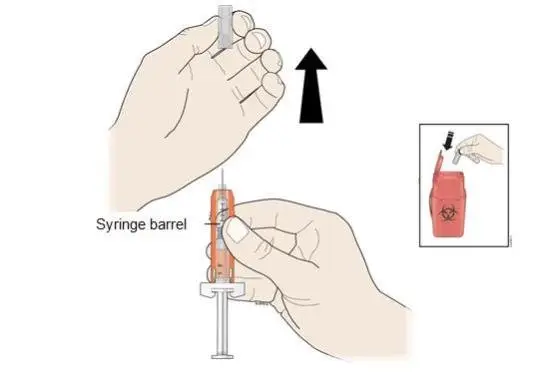
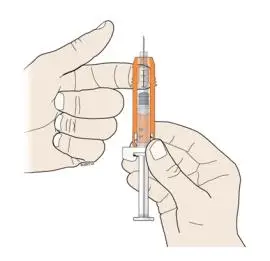
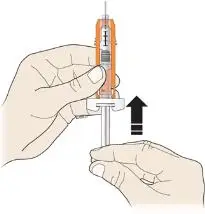
Inject NEUPOGEN subcutaneously in the outer area of upper arms, abdomen, thighs, or upper outer areas of the buttock. If patients or caregivers are to administer NEUPOGEN, instruct them in appropriate injection technique and ask them to follow the subcutaneous injection procedures in the Instructions for Use for the vial or prefilled syringe [see Patient Counseling Information (17)].
Training by the healthcare provider should aim to demonstrate to those patients and caregivers how to measure the dose of NEUPOGEN, and the focus should be on ensuring that a patient or caregiver can successfully perform all of the steps in the Instructions for Use for the vial or prefilled syringe. If a patient or caregiver is not able to demonstrate that they can measure the dose and administer the product successfully, you should consider whether the patient is an appropriate candidate for self-administration of NEUPOGEN or whether the patient would benefit from a different NEUPOGEN presentation. If a patient or caregiver experiences difficulty measuring the required dose, especially if it is other than the entire contents of the NEUPOGEN prefilled syringe, use of the NEUPOGEN vial may be considered.
If the patient or caregiver misses a dose of NEUPOGEN, instruct them to contact their healthcare provider.
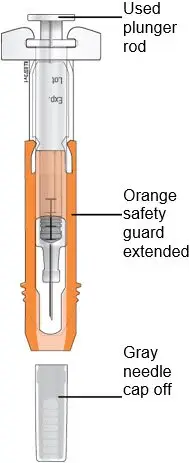
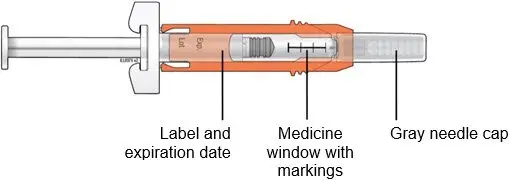
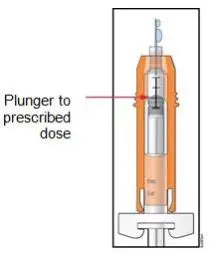
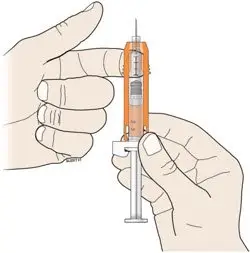
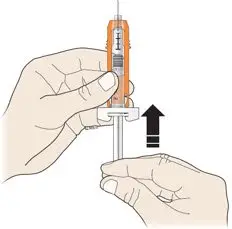
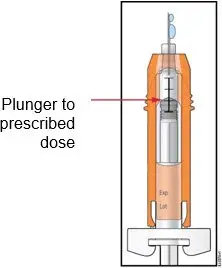
Administration Instructions for the Prefilled Syringe
Persons with latex allergies should not administer the NEUPOGEN prefilled syringe, because the needle cap contains dry natural rubber (derived from latex).
Administration Instructions for Dilution (Vial Only)
If required for intravenous administration‚ NEUPOGEN (vial only) may be diluted in 5% Dextrose Injection, USP from a concentration of 300 mcg/mL to 5 mcg/mL (do not dilute to a final concentration less than 5 mcg/mL). NEUPOGEN diluted to concentrations from 5 mcg/mL to 15 mcg/mL should be protected from adsorption to plastic materials by the addition of Albumin (Human) to a final concentration of 2 mg/mL. When diluted in 5% Dextrose Injection, USP or 5% Dextrose plus Albumin (Human)‚ NEUPOGEN is compatible with glass bottles‚ polyvinyl chloride (PVC) and polyolefin intravenous bags‚ and polypropylene syringes. Do not dilute with saline at any time because the product may precipitate.
Diluted NEUPOGEN solution can be stored at room temperature for up to 24 hours. This 24 hour time period includes the time during room temperature storage of the infusion solution and the duration of the infusion.
3. Dosage Forms and Strengths
Vial:
- Injection: 300 mcg/mL in a single-dose vial
- Injection: 480 mcg/1.6 mL in a single-dose vial
Prefilled Syringe:
- Injection: 300 mcg/0.5 mL in a single-dose prefilled syringe
- Injection: 480 mcg/0.8 mL in a single-dose prefilled syringe
4. Contraindications
NEUPOGEN is contraindicated in patients with a history of serious allergic reactions to human granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim [see Warnings and Precautions (5.3)].
5. Warnings and Precautions
5.1 Splenic Rupture
Splenic rupture, including fatal cases, has been reported following the administration of NEUPOGEN. Evaluate patients who report left upper abdominal or shoulder pain for an enlarged spleen or splenic rupture.
5.2 Acute Respiratory Distress Syndrome
Acute respiratory distress syndrome (ARDS) has been reported in patients receiving NEUPOGEN. Evaluate patients who develop fever and lung infiltrates or respiratory distress for ARDS. Discontinue NEUPOGEN in patients with ARDS.
5.3 Serious Allergic Reactions
Serious allergic reactions, including anaphylaxis, have been reported in patients receiving NEUPOGEN. The majority of reported events occurred upon initial exposure. Provide symptomatic treatment for allergic reactions. Allergic reactions, including anaphylaxis, in patients receiving NEUPOGEN can recur within days after the discontinuation of initial anti-allergic treatment. Permanently discontinue NEUPOGEN in patients with serious allergic reactions. NEUPOGEN is contraindicated in patients with a history of serious allergic reactions to human granulocyte colony-stimulating factors such as filgrastim or pegfilgrastim.
5.4 Sickle Cell Disorders
Sickle cell crisis, in some cases fatal, has been reported with the use of NEUPOGEN in patients with sickle cell trait or sickle cell disease.
5.5 Glomerulonephritis
Glomerulonephritis has occurred in patients receiving NEUPOGEN. The diagnoses were based upon azotemia, hematuria (microscopic and macroscopic), proteinuria, and renal biopsy. Generally, events of glomerulonephritis resolved after dose reduction or discontinuation of NEUPOGEN. If glomerulonephritis is suspected, evaluate for cause. If causality is likely, consider dose-reduction or interruption of NEUPOGEN.
5.6 Alveolar Hemorrhage and Hemoptysis
Alveolar hemorrhage manifesting as pulmonary infiltrates and hemoptysis requiring hospitalization have been reported in NEUPOGEN-treated healthy donors undergoing peripheral blood progenitor cell (PBPC) collection mobilization. Hemoptysis resolved with discontinuation of NEUPOGEN. The use of NEUPOGEN for PBPC mobilization in healthy donors is not an approved indication.
5.7 Capillary Leak Syndrome
Capillary leak syndrome (CLS) has been reported after G-CSF administration, including NEUPOGEN, and is characterized by hypotension, hypoalbuminemia, edema and hemoconcentration. Episodes vary in frequency, severity and may be life-threatening if treatment is delayed. Patients who develop symptoms of capillary leak syndrome should be closely monitored and receive standard symptomatic treatment, which may include a need for intensive care.
5.8 Patients with Severe Chronic Neutropenia
Confirm the diagnosis of SCN before initiating NEUPOGEN therapy.
Myelodysplastic syndrome (MDS) and acute myelogenous leukemia (AML) have been reported to occur in the natural history of congenital neutropenia without cytokine therapy. Cytogenetic abnormalities, transformation to MDS, and AML have also been observed in patients treated with NEUPOGEN for SCN. Based on available data including a postmarketing surveillance study, the risk of developing MDS and AML appears to be confined to the subset of patients with congenital neutropenia. Abnormal cytogenetics and MDS have been associated with the eventual development of myeloid leukemia. The effect of NEUPOGEN on the development of abnormal cytogenetics and the effect of continued NEUPOGEN administration in patients with abnormal cytogenetics or MDS are unknown. If a patient with SCN develops abnormal cytogenetics or myelodysplasia‚ the risks and benefits of continuing NEUPOGEN should be carefully considered.
5.9 Thrombocytopenia
Thrombocytopenia has been reported in patients receiving NEUPOGEN. Monitor platelet counts.
5.10 Leukocytosis
Patients with Cancer Receiving Myelosuppressive Chemotherapy
White blood cell counts of 100‚000/mm3 or greater were observed in approximately 2% of patients receiving NEUPOGEN at dosages above 5 mcg/kg/day. In patients with cancer receiving NEUPOGEN as an adjunct to myelosuppressive chemotherapy‚ to avoid the potential risks of excessive leukocytosis‚ it is recommended that NEUPOGEN therapy be discontinued if the ANC surpasses 10‚000/mm3 after the chemotherapy-induced ANC nadir has occurred. Monitor CBCs at least twice weekly during therapy. Dosages of NEUPOGEN that increase the ANC beyond 10‚000/mm3 may not result in any additional clinical benefit. In patients with cancer receiving myelosuppressive chemotherapy‚ discontinuation of NEUPOGEN therapy usually resulted in a 50% decrease in circulating neutrophils within 1 to 2 days‚ with a return to pretreatment levels in 1 to 7 days.
Peripheral Blood Progenitor Cell Collection and Therapy
During the period of administration of NEUPOGEN for PBPC mobilization in patients with cancer, discontinue NEUPOGEN if the leukocyte count rises to > 100,000/mm3.
5.11 Cutaneous Vasculitis
Cutaneous vasculitis has been reported in patients treated with NEUPOGEN. In most cases‚ the severity of cutaneous vasculitis was moderate or severe. Most of the reports involved patients with SCN receiving long-term NEUPOGEN therapy. Hold NEUPOGEN therapy in patients with cutaneous vasculitis. NEUPOGEN may be started at a reduced dose when the symptoms resolve and the ANC has decreased.
5.13 Simultaneous Use with Chemotherapy and Radiation Therapy Not Recommended
The safety and efficacy of NEUPOGEN given simultaneously with cytotoxic chemotherapy have not been established. Because of the potential sensitivity of rapidly dividing myeloid cells to cytotoxic chemotherapy‚ do not use NEUPOGEN in the period 24 hours before through 24 hours after the administration of cytotoxic chemotherapy [see Dosage and Administration (2.2)].
The safety and efficacy of NEUPOGEN have not been evaluated in patients receiving concurrent radiation therapy. Avoid the simultaneous use of NEUPOGEN with chemotherapy and radiation therapy.
6. Adverse Reactions/Side Effects
The following serious adverse reactions are discussed in greater detail in other sections of the labeling:
- Splenic Rupture [see Warnings and Precautions (5.1)]
- Acute Respiratory Distress Syndrome [see Warnings and Precautions (5.2)]
- Serious Allergic Reactions [see Warnings and Precautions (5.3)]
- Sickle Cell Disorders [see Warnings and Precautions (5.4)]
- Glomerulonephritis [see Warnings and Precautions (5.5)]
- Alveolar Hemorrhage and Hemoptysis [see Warnings and Precautions (5.6)]
- Capillary Leak Syndrome [see Warnings and Precautions (5.7)]
- Thrombocytopenia [see Warnings and Precautions (5.9)]
- Leukocytosis [see Warnings and Precautions (5.10)]
- Cutaneous Vasculitis [see Warnings and Precautions (5.11)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared with rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Adverse Reactions in Patients with Cancer Receiving Myelosuppressive Chemotherapy
The following adverse reaction data in Table 2 are from three randomized, placebo-controlled studies in patients with:
- small cell lung cancer receiving standard dose chemotherapy with cyclophosphamide‚ doxorubicin‚ and etoposide (Study 1)
- small cell lung cancer receiving ifosfamide, doxorubicin‚ and etoposide (Study 2), and
- non-Hodgkin’s lymphoma (NHL) receiving doxorubicin, cyclophosphamide, vindesine, bleomycin, methylprednisolone, and methotrexate (“ACVBP”) or mitoxantrone, ifosfamide, mitoguazone, teniposide, methotrexate, folinic acid, methylprednisolone, and methotrexate (“VIM3”) (Study 3).
A total of 451 patients were randomized to receive subcutaneous NEUPOGEN 230 mcg/m2 (Study 1), 240 mcg/m2 (Study 2) or 4 or 5 mcg/kg/day (Study 3) (n = 294) or placebo (n = 157). The patients in these studies were median age 61 (range 29 to 78) years and 64% were male. The ethnicity was 95% Caucasian, 4% African American, and 1% Asian.
| System Organ Class Preferred Term | NEUPOGEN (N = 294) | Placebo (N = 157) |
| Blood and lymphatic system disorders | ||
| Thrombocytopenia | 38% | 29% |
| Gastrointestinal disorders | ||
| Nausea | 43% | 32% |
| General disorders and administration site conditions | ||
| Pyrexia | 48% | 29% |
| Chest pain | 13% | 6% |
| Pain | 12% | 6% |
| Fatigue | 20% | 10% |
| Musculoskeletal and connective tissue disorders | ||
| Back pain | 15% | 8% |
| Arthralgia | 9% | 2% |
| Bone pain | 11% | 6% |
| Pain in extremity* | 7% | 3% |
| Nervous system disorders | ||
| Dizziness | 14% | 3% |
| Respiratory, thoracic and mediastinal disorders | ||
| Cough | 14% | 8% |
| Dyspnea | 13% | 8% |
| Skin and subcutaneous tissue disorders | ||
| Rash | 14% | 5% |
| Investigations | ||
| Blood lactate dehydrogenase increased | 6% | 1% |
| Blood alkaline phosphatase increased | 6% | 1% |
* Percent difference (NEUPOGEN – Placebo) was 4%.
Adverse events with ≥ 5% higher incidence in NEUPOGEN patients compared to placebo and associated with the sequelae of the underlying malignancy or cytotoxic chemotherapy delivered included anemia, constipation, diarrhea, oral pain, vomiting, asthenia, malaise, edema peripheral, hemoglobin decreased, decreased appetite, oropharyngeal pain, and alopecia.
Adverse Reactions in Patients with Acute Myeloid Leukemia
Adverse reaction data below are from a randomized, double-blind, placebo-controlled study in patients with AML (Study 4) who received an induction chemotherapy regimen of intravenous daunorubicin days 1, 2, and 3; cytosine arabinoside days 1 to 7; and etoposide days 1 to 5 and up to 3 additional courses of therapy (induction 2, and consolidation 1, 2) of intravenous daunorubicin, cytosine arabinoside, and etoposide. The safety population included 518 patients randomized to receive either 5 mcg/kg/day NEUPOGEN (n = 257) or placebo (n = 261). The median age was 54 (range 16 to 89) years and 54% were male.
Adverse reactions with ≥ 2% higher incidence in NEUPOGEN patients compared to placebo included epistaxis, back pain, pain in extremity, erythema, and rash maculo-papular.
Adverse events with ≥ 2% higher incidence in NEUPOGEN patients compared to placebo and associated with the sequelae of the underlying malignancy or cytotoxic chemotherapy included diarrhea, constipation, and transfusion reaction.
Adverse Reactions in Patients with Cancer Undergoing Bone Marrow Transplantation
The following adverse reaction data are from one randomized, no treatment-controlled study in patients with acute lymphoblastic leukemia or lymphoblastic lymphoma receiving high-dose chemotherapy (cyclophosphamide or cytarabine, and melphalan) and total body irradiation (Study 5) and one randomized, no treatment controlled study in patients with Hodgkin's disease (HD) and NHL undergoing high-dose chemotherapy and autologous bone marrow transplantation (Study 6). Patients receiving autologous bone marrow transplantation only were included in the analysis. A total of 100 patients received either 30 mcg/kg/day as a 4 hour infusion (Study 5) or 10 mcg/kg/day or 30 mcg/kg/day as a 24 hour infusion (Study 6) NEUPOGEN (n = 72), no treatment control or placebo (n = 28). The median age was 30 (range 15 to 57) years, 57% were male.
Adverse reactions with ≥ 5% higher incidence in NEUPOGEN patients compared to patients receiving no NEUPOGEN included rash and hypersensitivity.
Adverse reactions in patients receiving intensive chemotherapy followed by autologous BMT with ≥ 5% higher incidence in NEUPOGEN patients compared to patients receiving no NEUPOGEN included thrombocytopenia, anemia, hypertension, sepsis, bronchitis, and insomnia.
Adverse Reactions in Patients with Cancer Undergoing Autologous Peripheral Blood Progenitor Cell Collection
The adverse reaction data in Table 3 are from a series of 7 trials in patients with cancer undergoing mobilization of autologous peripheral blood progenitor cells for collection by leukapheresis. Patients (n = 166) in all these trials underwent a similar mobilization/collection regimen: NEUPOGEN was administered for 6 to 8 days‚ in most cases the apheresis procedure occurred on days 5‚ 6, and 7. The dosage of NEUPOGEN ranged between 5 to 30 mcg/kg/day and was administered subcutaneously by injection or continuous infusion. The median age was 39 (range 15 to 67) years, and 48% were male.
| System Organ Class Preferred Term | Mobilization Phase (N = 166) |
| Musculoskeletal and connective tissue disorders | |
| Bone pain | 30% |
| General disorders and administration site conditions | |
| Pyrexia | 16% |
| Investigations | |
| Blood alkaline phosphatase increased | 11% |
| Nervous system disorders | |
| Headache | 10% |
Adverse Reactions in Patients with Severe Chronic Neutropenia
The following adverse reaction data were identified in a randomized, controlled study in patients with SCN receiving NEUPOGEN (Study 7). 123 patients were randomized to a 4 month observation period followed by subcutaneous NEUPOGEN treatment or immediate subcutaneous NEUPOGEN treatment. The median age was 12 years (range 7 months to 76 years) and 46% were male. The dosage of NEUPOGEN was determined by the category of neutropenia. Initial dosage of NEUPOGEN:
- Idiopathic neutropenia: 3.6 mcg/kg/day
- Cyclic neutropenia: 6 mcg/kg/day
- Congenital neutropenia: 6 mcg/kg/day divided 2 times per day
The dosage was increased incrementally to 12 mcg/kg/day divided 2 times per day if there was no response.
Adverse reactions with ≥ 5% higher incidence in NEUPOGEN patients compared to patients receiving no NEUPOGEN included arthralgia, bone pain, back pain, muscle spasms, musculoskeletal pain, pain in extremity, splenomegaly, anemia, upper respiratory tract infection, and urinary tract infection (upper respiratory tract infection and urinary tract infection were higher in the NEUPOGEN arm, total infection related events were lower in NEUPOGEN treated patients), epistaxis, chest pain, diarrhea, hypoesthesia, and alopecia.
8. Use In Specific Populations
8.1 Pregnancy
Pregnancy Category C
There are no adequate and well-controlled studies in pregnant women. The potential risk to the fetus is unknown. Reports in the scientific literature have described transplacental passage of NEUPOGEN in pregnant women when administered ≤ 30 hours prior to preterm delivery (≤ 30 weeks gestation). NEUPOGEN should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Effects of filgrastim on prenatal development have been studied in rats and rabbits. No malformations were observed in either species. Filgrastim has been shown to have adverse effects in pregnant rabbits at doses 2 to 10 times higher than the human doses. In pregnant rabbits showing signs of maternal toxicity, reduced embryo-fetal survival (at 20 and 80 mcg/kg/day) and increased abortions (at 80 mcg/kg/day) were observed. In pregnant rats, no maternal or fetal effects were observed at doses up to 575 mcg/kg/day.
Offspring of rats administered filgrastim during the peri-natal and lactation periods exhibited a delay in external differentiation and growth retardation (≥ 20 mcg/kg/day) and slightly reduced survival rate (100 mcg/kg/day).
8.3 Nursing Mothers
It is not known whether NEUPOGEN is excreted in human milk. Because many drugs are excreted in human milk‚ caution should be exercised if NEUPOGEN is administered to women who are breastfeeding.
8.4 Pediatric Use
In patients with cancer receiving myelosuppressive chemotherapy‚ 15 pediatric patients median age 2.6 (range 1.2 to 9.4) years with neuroblastoma were treated with myelosuppressive chemotherapy (cyclophosphamide‚ cisplatin‚ doxorubicin‚ and etoposide) followed by subcutaneous NEUPOGEN at doses of 5, 10, or 15 mcg/kg/day for 10 days (n = 5/dose) (Study 8). The pharmacokinetics of NEUPOGEN in pediatric patients after chemotherapy are similar to those in adults receiving the same weight-normalized doses, suggesting no age-related differences in the pharmacokinetics of NEUPOGEN. In this population‚ NEUPOGEN was well tolerated. There was one report of palpable splenomegaly and one report of hepatosplenomegaly associated with NEUPOGEN therapy; however‚ the only consistently reported adverse event was musculoskeletal pain‚ which is no different from the experience in the adult population.
The safety and effectiveness of NEUPOGEN have been established in pediatric patients with SCN [see Clinical Studies (14.5)]. In a phase 3 study (Study 7) to assess the safety and efficacy of NEUPOGEN in the treatment of SCN, 123 patients with a median age of 12 years (range 7 months to 76 years) were studied. Of the 123 patients, 12 were infants (7 months to 2 years of age), 49 were children (2 to 12 years of age), and 9 were adolescents (12 to 16 years of age). Additional information is available from a SCN postmarketing surveillance study, which includes long-term follow-up of patients in the clinical studies and information from additional patients who entered directly into the postmarketing surveillance study. Of the 731 patients in the surveillance study, 429 were pediatric patients < 18 years of age (range 0.9 to 17) [see Indications and Usage (1.5), Dosage and Administration (2.6), and Clinical Studies (14.5)].
Long-term follow-up data from the postmarketing surveillance study suggest that height and weight are not adversely affected in patients who received up to 5 years of NEUPOGEN treatment. Limited data from patients who were followed in the phase 3 study for 1.5 years did not suggest alterations in sexual maturation or endocrine function.
Pediatric patients with congenital types of neutropenia (Kostmann’s syndrome, congenital agranulocytosis, or Schwachman-Diamond syndrome) have developed cytogenetic abnormalities and have undergone transformation to MDS and AML while receiving chronic NEUPOGEN treatment. The relationship of these events to NEUPOGEN administration is unknown [see Warnings and Precautions (5.8) and Adverse Reactions (6)].
The use of NEUPOGEN to increase survival in pediatric patients acutely exposed to myelosuppressive doses of radiation is based on studies conducted in animals and clinical data supporting the use of NEUPOGEN in other approved indications [see Dosage and Administration (2.1 to 2.4) and Clinical Studies (14.6)].
12. Neupogen - Clinical Pharmacology
12.3 Pharmacokinetics
Filgrastim exhibits nonlinear pharmacokinetics. Clearance is dependent on filgrastim concentration and neutrophil count: G-CSF receptor-mediated clearance is saturated by high concentration of NEUPOGEN and is diminished by neutropenia. In addition, filgrastim is cleared by the kidney.
Subcutaneous administration of 3.45 mcg/kg and 11.5 mcg/kg of filgrastim resulted in maximum serum concentrations of 4 and 49 ng/mL‚ respectively‚ within 2 to 8 hours. After intravenous administration, the volume of distribution averaged 150 mL/kg and the elimination half-life was approximately 3.5 hours in both normal subjects and cancer subjects. Clearance rates of filgrastim were approximately 0.5 to 0.7 mL/minute/kg. Single parenteral doses or daily intravenous doses‚ over a 14-day period‚ resulted in comparable half-lives. The half-lives were similar for intravenous administration (231 minutes‚ following doses of 34.5 mcg/kg) and for subcutaneous administration (210 minutes‚ following NEUPOGEN dosages of 3.45 mcg/kg). Continuous 24-hour intravenous infusions of 20 mcg/kg over an 11 to 20-day period produced steady-state serum concentrations of filgrastim with no evidence of drug accumulation over the time period investigated. The absolute bioavailability of filgrastim after subcutaneous administration is 60% to 70%.
Specific Populations
Patients Acutely Exposed to Myelosuppressive Doses of Radiation
The pharmacokinetics of filgrastim is not available in patients acutely exposed to myelosuppressive doses of radiation. Based on limited pharmacokinetics data in irradiated non-human primates, the area under the time-concentration curve (AUC), reflecting the exposure to filgrastim in non-human primates at 10 mcg/kg dose of NEUPOGEN, appears to be similar to that in humans at 5 mcg/kg. Simulations conducted using the population pharmacokinetic model indicates that the exposures to filgrastim at a NEUPOGEN dose of 10 mcg/kg in patients acutely exposed to myelosuppressive doses of radiation are expected to exceed the exposures at a dose of 10 mcg/kg in irradiated non-human primates.
Pediatric Patients
The pharmacokinetics of filgrastim in pediatric patients after chemotherapy are similar to those in adult patients receiving the same weight-normalized doses, suggesting no age-related differences in the pharmacokinetics of filgrastim [see Use in Specific Populations (8.4)].
Renal Impairment
In a study with healthy volunteers, subjects with moderate renal impairment, and subjects with end-stage renal disease (n = 4 per group), higher serum concentrations were observed in subjects with end-stage renal disease. However, dose adjustment in patients with renal impairment is not necessary.
Hepatic Impairment
Pharmacokinetics and pharmacodynamics of filgrastim are similar between subjects with hepatic impairment and healthy subjects (n = 12/group). The study included 10 subjects with mild hepatic impairment (Child-Pugh Class A) and 2 subjects with moderate hepatic impairment (Child-Pugh Class B). Therefore, filgrastim dose adjustment for patients with hepatic impairment is not necessary.
14. Clinical Studies
14.1 Patients with Cancer Receiving Myelosuppressive Chemotherapy
The safety and efficacy of NEUPOGEN to decrease the incidence of infection‚ as manifested by febrile neutropenia‚ in patients with nonmyeloid malignancies receiving myelosuppressive anti-cancer drugs were established in a randomized‚ double-blind‚ placebo-controlled trial conducted in patients with small cell lung cancer (Study 1).
In Study 1, patients received up to 6 cycles of intravenous chemotherapy including intravenous cyclophosphamide and doxorubicin on day 1; and etoposide on days 1, 2, and 3 of 21 day cycles. Patients were randomized to receive NEUPOGEN (n = 99) at a dose of 230 mcg/m2 (4 to 8 mcg/kg/day) or placebo (n = 111). Study drug was administered subcutaneously daily beginning on day 4, for a maximum of 14 days. A total of 210 patients were evaluable for efficacy and 207 were evaluable for safety. The demographic and disease characteristics were balanced between arms with a median age of 62 (range 31 to 80) years; 64% males; 89% Caucasian; 72% extensive disease and 28% limited disease.
The main efficacy endpoint was the incidence of febrile neutropenia. Febrile neutropenia was defined as an ANC < 1000/mm3 and temperature > 38.2°C. Treatment with NEUPOGEN resulted in a clinically and statistically significant reduction in the incidence of infection‚ as manifested by febrile neutropenia, 40% for NEUPOGEN-treated patients and 76% for placebo-treated patients (p < 0.001). There were also statistically significant reductions in the incidence and overall duration of infection manifested by febrile neutropenia; the incidence, severity and duration of severe neutropenia (ANC < 500/mm3); the incidence and overall duration of hospital admissions; and the number of reported days of antibiotic use.
14.2 Patients with Acute Myeloid Leukemia Receiving Induction or Consolidation Chemotherapy
The safety and efficacy of NEUPOGEN to reduce the time to neutrophil recovery and the duration of fever, following induction or consolidation chemotherapy treatment of patients with acute myeloid leukemia (AML) was established in a randomized, double-blind‚ placebo-controlled‚ multi-center trial in patients with newly diagnosed, de novo AML (Study 4).
In Study 4 the initial induction therapy consisted of intravenous daunorubicin days 1, 2, and 3; cytosine arabinoside days 1 to 7; and etoposide days 1 to 5. Patients were randomized to receive subcutaneous NEUPOGEN (n = 259) at a dose of 5 mcg/kg/day or placebo (n = 262) from 24 hours after the last dose of chemotherapy until neutrophil recovery (ANC ≥ 1000/mm3 for 3 consecutive days or ≥ 10,000/mm3 for 1 day) or for a maximum of 35 days. The demographic and disease characteristics were balanced between arms with a median age of 54 (range 16 to 89) years; 54% males; initial white blood cell count (65% < 25,000/mm3 and 27% > 100,000/mm3); 29% unfavorable cytogenetics.
The main efficacy endpoint was median duration of severe neutropenia defined as neutrophil count < 500/mm3. Treatment with NEUPOGEN resulted in a clinically and statistically significant reduction in median number of days of severe neutropenia, NEUPOGEN-treated patients 14 days, placebo-treated patients 19 days (p = 0.0001: difference of 5 days (95% CI: -6.0, -4.0)). There was a reduction in the median duration of intravenous antibiotic use, NEUPOGEN-treated patients: 15 days versus placebo-treated patients: 18.5 days; a reduction in the median duration of hospitalization, NEUPOGEN-treated patients: 20 days versus placebo-treated patients: 25 days.
There were no statistically significant differences between the NEUPOGEN and the placebo groups in complete remission rate (69% - NEUPOGEN, 68% - placebo), median time to progression of all randomized patients (165 days - NEUPOGEN, 186 days - placebo), or median overall survival (380 days - NEUPOGEN, 425 days - placebo).
14.3 Patients with Cancer Undergoing Bone Marrow Transplantation
The safety and efficacy of NEUPOGEN to reduce the duration of neutropenia in patients with nonmyeloid malignancies undergoing myeloablative chemotherapy followed by autologous bone marrow transplantation was evaluated in 2 randomized controlled trials of patients with lymphoma (Study 6 and Study 9). The safety and efficacy of NEUPOGEN to reduce the duration of neutropenia in patients undergoing myeloablative chemotherapy followed by allogeneic bone marrow transplantation was evaluated in a randomized placebo controlled trial (Study 10).
In Study 6 patients with Hodgkin’s disease received a preparative regimen of intravenous cyclophosphamide, etoposide, and BCNU (“CVP”), and patients with non-Hodgkin’s lymphoma received intravenous BCNU, etoposide, cytosine arabinoside and melphalan (“BEAM”). There were 54 patients randomized 1:1:1 to control, NEUPOGEN 10 mcg/kg/day, and NEUPOGEN 30 mcg/kg/day as a 24 hour continuous infusion starting 24 hours after bone marrow infusion for a maximum of 28 days. The median age was 33 (range 17 to 57) years; 56% males; 69% Hodgkin’s disease and 31% non-Hodgkin’s lymphoma.
The main efficacy endpoint was duration of severe neutropenia ANC < 500/mm3. A statistically significant reduction in the median number of days of severe neutropenia (ANC < 500/mm3) occurred in the NEUPOGEN-treated groups versus the control group (23 days in the control group‚ 11 days in the 10 mcg/kg/day group, and 14 days in the 30 mcg/kg/day group [11 days in the combined treatment groups‚ p = 0.004]).
In Study 9, patients with Hodgkin’s disease and non-Hodgkin’s lymphoma received a preparative regimen of intravenous cyclophosphamide, etoposide, and BCNU (“CVP”). There were 43 evaluable patients randomized to continuous subcutaneous infusion NEUPOGEN 10 mcg/kg/day (n = 19), NEUPOGEN 30 mcg/kg/day (n = 10) and no treatment (n = 14) starting the day after marrow infusion for a maximum of 28 days. The median age was 33 (range 17 to 56) years; 67% males; 28% Hodgkin’s disease and 72% non-Hodgkin’s lymphoma.
The main efficacy endpoint was duration of severe neutropenia. There was statistically significant reduction in the median number of days of severe neutropenia (ANC < 500/mm3) in the NEUPOGEN-treated groups versus the control group (21.5 days in the control group versus 10 days in the NEUPOGEN-treated groups, p < 0.001). The number of days of febrile neutropenia was also reduced significantly in this study (13.5 days in the control group versus 5 days in the NEUPOGEN-treated groups‚ p < 0.0001).
In Study 10, 70 patients scheduled to undergo bone marrow transplantation for multiple underlying conditions using multiple preparative regimens were randomized to receive NEUPOGEN 300 mcg/m2/day (n = 33) or placebo (n = 37) days 5 through 28 after marrow infusion. The median age was 18 (range 1 to 45) years, 56% males. The underlying disease was: 67% hematologic malignancy, 24% aplastic anemia, 9% other. A statistically significant reduction in the median number of days of severe neutropenia occurred in the treated group versus the control group (19 days in the control group and 15 days in the treatment group‚ p < 0.001) and time to recovery of ANC to ≥ 500/mm3 (21 days in the control group and 16 days in the treatment group‚ p < 0.001).
14.4 Patients Undergoing Autologous Peripheral Blood Progenitor Cell Collection and Therapy
The safety and efficacy of NEUPOGEN to mobilize autologous peripheral blood progenitor cells for collection by leukapheresis was supported by the experience in uncontrolled trials, and a randomized trial comparing hematopoietic stem cell rescue using NEUPOGEN mobilized autologous peripheral blood progenitor cells to autologous bone marrow (Study 11). Patients in all these trials underwent a similar mobilization/collection regimen: NEUPOGEN was administered for 6 to 7 days‚ in most cases the apheresis procedure occurred on days 5‚ 6, and 7. The dose of NEUPOGEN ranged between 10 to 24 mcg/kg/day and was administered subcutaneously by injection or continuous intravenous infusion.
Engraftment was evaluated in 64 patients who underwent transplantation using NEUPOGEN mobilized autologous hematopoietic progenitor cells in uncontrolled trials. Two of the 64 patients (3%) did not achieve the criteria for engraftment as defined by a platelet count ≥ 20‚000/mm3 by day 28. In clinical trials of NEUPOGEN for the mobilization of hematopoietic progenitor cells‚ NEUPOGEN was administered to patients at doses between 5 to 24 mcg/kg/day after reinfusion of the collected cells until a sustainable ANC (≥ 500/mm3) was reached. The rate of engraftment of these cells in the absence of NEUPOGEN post transplantation has not been studied.
Study 11 was a randomized, unblinded study of patients with Hodgkin’s disease or non-Hodgkin’s lymphoma undergoing myeloablative chemotherapy‚ 27 patients received NEUPOGEN-mobilized autologous hematopoietic progenitor cells and 31 patients received autologous bone marrow. The preparative regimen was intravenous BCNU, etoposide, cytosine arabinoside and melphalan (“BEAM”). Patients received daily NEUPOGEN 24 hours after stem cell infusion at a dose of 5 mcg/kg/day. The median age was 33 (range 1 to 59) years; 64% males; 57% Hodgkin’s disease and 43% non-Hodgkin’s lymphoma. The main efficacy endpoint was number of days of platelet transfusions. Patients randomized to NEUPOGEN-mobilized autologous peripheral blood progenitor cells compared to autologous bone marrow had significantly fewer days of platelet transfusions (median 6 vs 10 days).
14.5 Patients with Severe Chronic Neutropenia
The safety and efficacy of NEUPOGEN to reduce the incidence and duration of sequelae of neutropenia (that is fever‚ infections, oropharyngeal ulcers) in symptomatic adult and pediatric patients with congenital neutropenia‚ cyclic neutropenia‚ or idiopathic neutropenia was established in a randomized controlled trial conducted in patients with severe neutropenia (Study 7).
Patients eligible for Study 7 had a history of severe chronic neutropenia documented with an ANC < 500/mm3 on three occasions during a 6 month period, or in patients with cyclic neutropenia 5 consecutive days of ANC < 500/mm3 per cycle. In addition patients must have experienced a clinically significant infection during the previous 12 months. Patients were randomized to a 4 month observation period followed by NEUPOGEN treatment or immediate NEUPOGEN treatment. The median age was 12 years (range 7 months to 76 years); 46% males; 34% idiopathic, 17% cyclic and 49% congenital neutropenia.
NEUPOGEN was administered subcutaneously. The dose of NEUPOGEN was determined by the category of neutropenia. Initial dose of NEUPOGEN:
- Idiopathic neutropenia: 3.6 mcg/kg/day
- Cyclic neutropenia: 6 mcg/kg/day
- Congenital neutropenia: 6 mcg/kg/day divided 2 times per day
The dose was increased incrementally to 12 mcg/kg/day divided 2 times per day if there was no response.
The main efficacy endpoint was response to NEUPOGEN treatment. ANC response from baseline (< 500/mm3) was defined as follows:
- Complete response: median ANC > 1500/mm3
- Partial response: median ANC ≥ 500/mm3 and ≤ 1500/mm3 with a minimum increase of 100%
- No response: median ANC < 500/mm3
There were 112 of 123 patients who demonstrated a complete or partial response to NEUPOGEN treatment.
Additional efficacy endpoints included a comparison between patients randomized to 4 months of observation and patients receiving NEUPOGEN of the following parameters:
- incidence of infection
- incidence of fever
- duration of fever
- incidence, duration, and severity of oropharyngeal ulcers
- number of days of antibiotic use
The incidence for each of these 5 clinical parameters was lower in the NEUPOGEN arm compared to the control arm for cohorts in each of the 3 major diagnostic categories. An analysis of variance showed no significant interaction between treatment and diagnosis‚ suggesting that efficacy did not differ substantially in the different diseases. Although NEUPOGEN substantially reduced neutropenia in all patient groups‚ in patients with cyclic neutropenia‚ cycling persisted but the period of neutropenia was shortened to 1 day.
14.6 Patients Acutely Exposed to Myelosuppressive Doses of Radiation (Hematopoietic Syndrome of Acute Radiation Syndrome)
Efficacy studies of NEUPOGEN could not be conducted in humans with acute radiation syndrome for ethical and feasibility reasons. Approval of this indication was based on efficacy studies conducted in animals and data supporting the use of NEUPOGEN for other approved indications [see Dosage and Administration (2.1 to 2.4)].
Because of the uncertainty associated with extrapolating animal efficacy data to humans, the selection of human dose for NEUPOGEN is aimed at providing exposures to filgrastim that exceed those observed in animal efficacy studies. The 10 mcg/kg daily dose is selected for humans exposed to myelosuppressive doses of radiation because the exposure associated with such a dose is expected to exceed the exposure associated with a 10 mcg/kg dose in non-human primates [see Pharmacokinetics (12.3)]. The safety of NEUPOGEN at a daily dose of 10 mcg/kg has been assessed on the basis of clinical experience in approved indications.
The efficacy of NEUPOGEN was studied in a randomized, blinded, placebo-controlled study in a non-human primate model of radiation injury. The planned sample size was 62 animals, but the study was stopped at the interim analysis with 46 animals because efficacy was established. Rhesus macaques were randomized to a control (n = 22) or treated (n = 24) group. Animals were exposed to total body irradiation of 7.4 ± 0.15 Gy delivered at 0.8 ± 0.03 Gy/min, representing a dose that would be lethal in 50% of animals by 60 days of follow-up (LD50/60). Starting on day 1 after irradiation, animals received daily subcutaneous injections of placebo (5% dextrose in water) or filgrastim (10 mcg/kg/day). Blinded treatment was stopped when one of the following criteria was met: ANC ≥ 1,000/mm3 for 3 consecutive days, or ANC ≥ 10,000/mm3 for more than 2 consecutive days within study day 1 to 5, or ANC ≥ 10,000/mm3 any time after study day 5. Animals received medical management consisting of intravenous fluids, antibiotics, blood transfusions, and other support as required.
Filgrastim significantly (at 0.023 level of significance) reduced 60-day mortality in the irradiated non-human primates: 21% mortality (5/24) in the filgrastim group compared to 59% mortality (13/22) in the control group.
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use). Review the steps for direct patient administration with patients and caregivers. Training by the healthcare provider should aim to ensure that patients and caregivers can successfully perform all of the steps in the Instructions for Use of NEUPOGEN vial and prefilled syringe, including showing the patient or caregiver how to measure the required dose, particularly if a patient is on a dose other than the entire prefilled syringe. If a patient or caregiver is not able to demonstrate that they can measure the dose and administer the product successfully, you should consider whether the patient is an appropriate candidate for self-administration of NEUPOGEN or whether the patient would benefit from a different NEUPOGEN presentation.
Advise patients of the following risks and potential risks with NEUPOGEN:
- Rupture or enlargement of the spleen may occur. Symptoms include left upper quadrant abdominal pain or left shoulder pain. Advise patients to report pain in these areas to their physician immediately [see Warnings and Precautions (5.1)].
- Dyspnea, with or without fever, progressing to Acute Respiratory Distress Syndrome, may occur. Advise patients to report dyspnea to their physician immediately [see Warnings and Precautions (5.2)].
- Serious allergic reactions may occur, which may be signaled by rash‚ facial edema‚ wheezing‚ dyspnea‚ hypotension‚ or tachycardia. Advise patients to seek immediate medical attention if signs or symptoms of hypersensitivity reaction occur [see Warnings and Precautions (5.3)].
- In patients with sickle cell disease, sickle cell crisis and death have occurred. Discuss potential risks and benefits for patients with sickle cell disease prior to the administration of human granulocyte colony-stimulating factors [see Warnings and Precautions (5.4)].
- Glomerulonephritis may occur. Symptoms include swelling of the face or ankles, dark colored urine or blood in the urine, or a decrease in urine production. Advise patients to report signs or symptoms of glomerulonephritis to their physician immediately [see Warnings and Precautions (5.5)].
- Cutaneous vasculitis may occur, which may be signaled by purpura or erythema. Advise patients to report signs or symptoms of vasculitis to their physician immediately [see Warnings and Precautions (5.11)].
- Advise females of reproductive potential that NEUPOGEN should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus [see Use in Specific Populations (8.1)].
- Advise patients acutely exposed to myelosuppressive doses of radiation (Hematopoietic Syndrome of Acute Radiation Syndrome) that efficacy studies of NEUPOGEN for this indication could not be conducted in humans for ethical and feasibility reasons and that, therefore, approval of this use was based on efficacy studies conducted in animals [see Clinical Studies (14.6)].
Instruct patients who self-administer NEUPOGEN using the prefilled syringe or single-dose vial of the:
- Importance of following the applicable Instructions for Use.
- Dangers of reusing needles, syringes, or unused portions of single-dose vials.
- Importance of following local requirements for proper disposal of used syringes, needles, and unused vials.
- Importance of informing the healthcare provider if difficulty occurs when measuring or administering partial contents of the NEUPOGEN prefilled syringe. If difficulty occurs, use of the NEUPOGEN vial may be considered.
- Difference in product concentration of the NEUPOGEN prefilled syringe in comparison to the NEUPOGEN vial. When switching patients from the NEUPOGEN prefilled syringe to the NEUPOGEN vial, or vice versa, ensure that patients understand the correct volume to be administered since the concentration of NEUPOGEN differs between the prefilled syringe and the vial.
NEUPOGEN® (filgrastim)
Manufactured by:
Amgen Inc.
One Amgen Center Drive
Thousand Oaks, California 91320-1799
U.S. License Number 1080
Patent: http://pat.amgen.com/neupogen/
© 1991-2016 Amgen Inc. All rights reserved.
www.NEUPOGEN.com
1-800-77-AMGEN (1-800-772-6436)
1xxxxxx
v30












| NEUPOGEN
filgrastim injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| NEUPOGEN
filgrastim injection, solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| NEUPOGEN
filgrastim injection, solution |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
| NEUPOGEN
filgrastim injection, solution |
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
|
|||||||||||||||||||||||||
| Labeler - Amgen Inc (039976196) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Amgen Manufacturing Ltd | 785800020 | ANALYSIS(55513-530, 55513-546, 55513-924, 55513-209) , LABEL(55513-530, 55513-546, 55513-924, 55513-209) , MANUFACTURE(55513-530, 55513-546, 55513-924, 55513-209) , PACK(55513-530, 55513-546, 55513-924, 55513-209) | |
