Drug Detail:Prolia (Denosumab (prolia) [ den-oh-sue-mab ])
Drug Class: Miscellaneous bone resorption inhibitors
Highlights of Prescribing Information
Prolia® (denosumab)
Injection, for subcutaneous use
Initial U.S. Approval: 2010
Recent Major Changes
| 01/2023 |
| 05/2022 |
Indications and Usage for Prolia
Prolia is a RANK ligand (RANKL) inhibitor indicated for:
- Treatment of postmenopausal women with osteoporosis at high risk for fracture (1.1)
- Treatment to increase bone mass in men with osteoporosis at high risk for fracture (1.2)
- Treatment of glucocorticoid-induced osteoporosis in men and women at high risk for fracture (1.3)
- Treatment to increase bone mass in men at high risk for fracture receiving androgen deprivation therapy for nonmetastatic prostate cancer (1.4)
- Treatment to increase bone mass in women at high risk for fracture receiving adjuvant aromatase inhibitor therapy for breast cancer (1.5)
Prolia Dosage and Administration
- Pregnancy must be ruled out prior to administration of Prolia. (2.1)
- Prolia should be administered by a healthcare professional. (2.2)
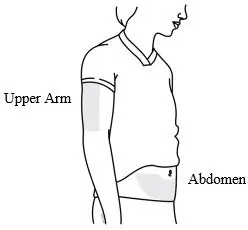
- Administer 60 mg every 6 months as a subcutaneous injection in the upper arm, upper thigh, or abdomen. (2.2)
- Instruct patients to take calcium 1000 mg daily and at least 400 IU vitamin D daily. (2.2)
Dosage Forms and Strengths
- Injection: Single-dose prefilled syringe containing 60 mg in a 1 mL solution (3)
Contraindications
- Hypocalcemia (4, 5.3)
- Pregnancy (4, 8.1)
- Known hypersensitivity to Prolia (4, 5.2)
Warnings and Precautions
- Same Active Ingredient: Patients receiving Prolia should not receive XGEVA®. (5.1)
- Hypersensitivity including anaphylactic reactions may occur. Discontinue permanently if a clinically significant reaction occurs. (5.2)
- Hypocalcemia: Must be corrected before initiating Prolia. May worsen, especially in patients with renal impairment. Adequately supplement patients with calcium and vitamin D. (5.3)
- Osteonecrosis of the jaw: Has been reported with Prolia. Monitor for symptoms. (5.4)
- Atypical femoral fractures: Have been reported. Evaluate patients with thigh or groin pain to rule out a femoral fracture. (5.5)
- Multiple vertebral fractures have been reported following Prolia discontinuation. Patients should be transitioned to another antiresorptive agent if Prolia is discontinued. (5.6)
- Serious infections including skin infections: May occur, including those leading to hospitalization. Advise patients to seek prompt medical attention if they develop signs or symptoms of infection, including cellulitis. (5.7)
- Dermatologic reactions: Dermatitis, rashes, and eczema have been reported. Consider discontinuing Prolia if severe symptoms develop. (5.8)
- Severe bone, joint, muscle pain may occur. Discontinue use if severe symptoms develop. (5.9)
- Suppression of bone turnover: Significant suppression has been demonstrated. Monitor for consequences of bone over-suppression. (5.10)
Adverse Reactions/Side Effects
- Postmenopausal osteoporosis: Most common adverse reactions (> 5% and more common than placebo) were: back pain, pain in extremity, hypercholesterolemia, musculoskeletal pain, and cystitis. Pancreatitis has been reported in clinical trials. (6.1)
- Male osteoporosis: Most common adverse reactions (> 5% and more common than placebo) were: back pain, arthralgia, and nasopharyngitis. (6.1)
- Glucocorticoid-induced osteoporosis: Most common adverse reactions (> 3% and more common than active-control group) were: back pain, hypertension, bronchitis, and headache. (6.1)
- Bone loss due to hormone ablation for cancer: Most common adverse reactions (≥ 10% and more common than placebo) were: arthralgia and back pain. Pain in extremity and musculoskeletal pain have also been reported in clinical trials. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Amgen Inc. at 1-800-77-AMGEN (1-800-772-6436) or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Use In Specific Populations
- Pregnant women and females of reproductive potential: Prolia may cause fetal harm when administered to pregnant women. Advise females of reproductive potential to use effective contraception during therapy, and for at least 5 months after the last dose of Prolia. (8.1, 8.3)
- Pediatric patients: Prolia is not approved for use in pediatric patients. (8.4)
- Renal impairment: No dose adjustment is necessary in patients with renal impairment. Patients with creatinine clearance < 30 mL/min or receiving dialysis are at risk for hypocalcemia. Supplement with calcium and vitamin D, and consider monitoring serum calcium. (8.6)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 1/2023
Full Prescribing Information
1. Indications and Usage for Prolia
1.1 Treatment of Postmenopausal Women with Osteoporosis at High Risk for Fracture
Prolia is indicated for the treatment of postmenopausal women with osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, or multiple risk factors for fracture; or patients who have failed or are intolerant to other available osteoporosis therapy. In postmenopausal women with osteoporosis, Prolia reduces the incidence of vertebral, nonvertebral, and hip fractures [see Clinical Studies (14.1)].
1.2 Treatment to Increase Bone Mass in Men with Osteoporosis
Prolia is indicated for treatment to increase bone mass in men with osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, or multiple risk factors for fracture; or patients who have failed or are intolerant to other available osteoporosis therapy [see Clinical Studies (14.2)].
1.3 Treatment of Glucocorticoid-Induced Osteoporosis
Prolia is indicated for the treatment of glucocorticoid-induced osteoporosis in men and women at high risk of fracture who are either initiating or continuing systemic glucocorticoids in a daily dosage equivalent to 7.5 mg or greater of prednisone and expected to remain on glucocorticoids for at least 6 months. High risk of fracture is defined as a history of osteoporotic fracture, multiple risk factors for fracture, or patients who have failed or are intolerant to other available osteoporosis therapy [see Clinical Studies (14.3)].
1.4 Treatment of Bone Loss in Men Receiving Androgen Deprivation Therapy for Prostate Cancer
Prolia is indicated as a treatment to increase bone mass in men at high risk for fracture receiving androgen deprivation therapy for nonmetastatic prostate cancer. In these patients Prolia also reduced the incidence of vertebral fractures [see Clinical Studies (14.4)].
2. Prolia Dosage and Administration
2.1 Information Essential to Safe Dosing or Administration
Pregnancy must be ruled out prior to administration of Prolia. Perform pregnancy testing in all females of reproductive potential prior to administration of Prolia. Based on findings in animals, Prolia can cause fetal harm when administered to pregnant women [see Use in Specific Populations (8.1, 8.3)].
2.3 Preparation and Administration
Visually inspect Prolia for particulate matter and discoloration prior to administration whenever solution and container permit. Prolia is a clear, colorless to pale yellow solution that may contain trace amounts of translucent to white proteinaceous particles. Do not use if the solution is discolored or cloudy or if the solution contains many particles or foreign particulate matter.
Prior to administration, Prolia may be removed from the refrigerator and brought to room temperature (up to 25°C/77°F) by standing in the original container. This generally takes 15 to 30 minutes. Do not warm Prolia in any other way [see How Supplied/Storage and Handling (16)].


3. Dosage Forms and Strengths
- Injection: 1 mL of a 60 mg/mL denosumab solution in a single-dose prefilled syringe.
4. Contraindications
Prolia is contraindicated in:
- Hypocalcemia: Pre-existing hypocalcemia must be corrected prior to initiating therapy with Prolia [see Warnings and Precautions (5.3)].
- Pregnancy: Prolia may cause fetal harm when administered to a pregnant woman. In women of reproductive potential, pregnancy testing should be performed prior to initiating treatment with Prolia [see Use in Specific Populations (8.1)].
- Hypersensitivity: Prolia is contraindicated in patients with a history of systemic hypersensitivity to any component of the product. Reactions have included anaphylaxis, facial swelling, and urticaria [see Warnings and Precautions (5.2), Adverse Reactions (6.2)].
5. Warnings and Precautions
5.1 Drug Products with Same Active Ingredient
Prolia contains the same active ingredient (denosumab) found in Xgeva. Patients receiving Prolia should not receive Xgeva.
5.2 Hypersensitivity
Clinically significant hypersensitivity including anaphylaxis has been reported with Prolia. Symptoms have included hypotension, dyspnea, throat tightness, facial and upper airway edema, pruritus, and urticaria. If an anaphylactic or other clinically significant allergic reaction occurs, initiate appropriate therapy and discontinue further use of Prolia [see Contraindications (4), Adverse Reactions (6.2)].
5.3 Hypocalcemia and Mineral Metabolism
Hypocalcemia may be exacerbated by the use of Prolia. Pre-existing hypocalcemia must be corrected prior to initiating therapy with Prolia. In patients predisposed to hypocalcemia and disturbances of mineral metabolism (e.g. history of hypoparathyroidism, thyroid surgery, parathyroid surgery, malabsorption syndromes, excision of small intestine, severe renal impairment [creatinine clearance < 30 mL/min] or receiving dialysis, treatment with other calcium-lowering drugs), clinical monitoring of calcium and mineral levels (phosphorus and magnesium) is highly recommended within 14 days of Prolia injection. In some postmarketing cases, hypocalcemia persisted for weeks or months and required frequent monitoring and intravenous and/or oral calcium replacement, with or without vitamin D.
Hypocalcemia following Prolia administration is a significant risk in patients with severe renal impairment (creatinine clearance < 30 mL/min) or receiving dialysis. These patients may also develop marked elevations of serum parathyroid hormone (PTH). Concomitant use of calcimimetic drugs may worsen hypocalcemia risk and serum calcium should be closely monitored. Instruct all patients with severe renal impairment, including those receiving dialysis, about the symptoms of hypocalcemia and the importance of maintaining calcium levels with adequate calcium and vitamin D supplementation.
Adequately supplement all patients with calcium and vitamin D [see Dosage and Administration (2.1), Contraindications (4), Adverse Reactions (6.1) and Patient Counseling Information (17)].
5.4 Osteonecrosis of the Jaw
Osteonecrosis of the jaw (ONJ), which can occur spontaneously, is generally associated with tooth extraction and/or local infection with delayed healing. ONJ has been reported in patients receiving denosumab [see Adverse Reactions (6.1)]. A routine oral exam should be performed by the prescriber prior to initiation of Prolia treatment. A dental examination with appropriate preventive dentistry is recommended prior to treatment with Prolia in patients with risk factors for ONJ such as invasive dental procedures (e.g. tooth extraction, dental implants, oral surgery), diagnosis of cancer, concomitant therapies (e.g. chemotherapy, corticosteroids, angiogenesis inhibitors), poor oral hygiene, and comorbid disorders (e.g. periodontal and/or other pre-existing dental disease, anemia, coagulopathy, infection, ill-fitting dentures). Good oral hygiene practices should be maintained during treatment with Prolia. Concomitant administration of drugs associated with ONJ may increase the risk of developing ONJ. The risk of ONJ may increase with duration of exposure to Prolia.
For patients requiring invasive dental procedures, clinical judgment of the treating physician and/or oral surgeon should guide the management plan of each patient based on individual benefit-risk assessment.
Patients who are suspected of having or who develop ONJ while on Prolia should receive care by a dentist or an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition. Discontinuation of Prolia therapy should be considered based on individual benefit-risk assessment.
5.5 Atypical Subtrochanteric and Diaphyseal Femoral Fractures
Atypical low energy or low trauma fractures of the shaft have been reported in patients receiving Prolia [see Adverse Reactions (6.1)]. These fractures can occur anywhere in the femoral shaft from just below the lesser trochanter to above the supracondylar flare and are transverse or short oblique in orientation without evidence of comminution. Causality has not been established as these fractures also occur in osteoporotic patients who have not been treated with antiresorptive agents.
Atypical femoral fractures most commonly occur with minimal or no trauma to the affected area. They may be bilateral, and many patients report prodromal pain in the affected area, usually presenting as dull, aching thigh pain, weeks to months before a complete fracture occurs. A number of reports note that patients were also receiving treatment with glucocorticoids (e.g. prednisone) at the time of fracture.
During Prolia treatment, patients should be advised to report new or unusual thigh, hip, or groin pain. Any patient who presents with thigh or groin pain should be suspected of having an atypical fracture and should be evaluated to rule out an incomplete femur fracture. Patient presenting with an atypical femur fracture should also be assessed for symptoms and signs of fracture in the contralateral limb. Interruption of Prolia therapy should be considered, pending a benefit-risk assessment, on an individual basis.
5.6 Multiple Vertebral Fractures (MVF) Following Discontinuation of Prolia Treatment
Following discontinuation of Prolia treatment, fracture risk increases, including the risk of multiple vertebral fractures. Treatment with Prolia results in significant suppression of bone turnover and cessation of Prolia treatment results in increased bone turnover above pretreatment values 9 months after the last dose of Prolia. Bone turnover then returns to pretreatment values 24 months after the last dose of Prolia. In addition, bone mineral density (BMD) returns to pretreatment values within 18 months after the last injection [see Clinical Pharmacology (12.2), Clinical Studies (14.1)].
New vertebral fractures occurred as early as 7 months (on average 19 months) after the last dose of Prolia. Prior vertebral fracture was a predictor of multiple vertebral fractures after Prolia discontinuation. Evaluate an individual's benefit-risk before initiating treatment with Prolia.
If Prolia treatment is discontinued, patients should be transitioned to an alternative antiresorptive therapy [see Adverse Reactions (6.1)].
5.7 Serious Infections
In a clinical trial of over 7800 women with postmenopausal osteoporosis, serious infections leading to hospitalization were reported more frequently in the Prolia group than in the placebo group [see Adverse Reactions (6.1)]. Serious skin infections, as well as infections of the abdomen, urinary tract, and ear, were more frequent in patients treated with Prolia. Endocarditis was also reported more frequently in Prolia-treated patients. The incidence of opportunistic infections was similar between placebo and Prolia groups, and the overall incidence of infections was similar between the treatment groups. Advise patients to seek prompt medical attention if they develop signs or symptoms of severe infection, including cellulitis.
Patients on concomitant immunosuppressant agents or with impaired immune systems may be at increased risk for serious infections. Consider the benefit-risk profile in such patients before treating with Prolia. In patients who develop serious infections while on Prolia, prescribers should assess the need for continued Prolia therapy.
5.8 Dermatologic Adverse Reactions
In a large clinical trial of over 7800 women with postmenopausal osteoporosis, epidermal and dermal adverse events such as dermatitis, eczema, and rashes occurred at a significantly higher rate in the Prolia group compared to the placebo group. Most of these events were not specific to the injection site [see Adverse Reactions (6.1)]. Consider discontinuing Prolia if severe symptoms develop.
5.9 Musculoskeletal Pain
In postmarketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking Prolia [see Adverse Reactions (6.2)]. The time to onset of symptoms varied from one day to several months after starting Prolia. Consider discontinuing use if severe symptoms develop [see Patient Counseling Information (17)].
5.10 Suppression of Bone Turnover
In clinical trials in women with postmenopausal osteoporosis, treatment with Prolia resulted in significant suppression of bone remodeling as evidenced by markers of bone turnover and bone histomorphometry [see Clinical Pharmacology (12.2), Clinical Studies (14.1)]. The significance of these findings and the effect of long-term treatment with Prolia are unknown. The long-term consequences of the degree of suppression of bone remodeling observed with Prolia may contribute to adverse outcomes such as osteonecrosis of the jaw, atypical fractures, and delayed fracture healing. Monitor patients for these consequences.
5.11 Hypercalcemia in Pediatric Patients with Osteogenesis Imperfecta
Prolia is not approved for use in pediatric patients. Hypercalcemia has been reported in pediatric patients with osteogenesis imperfecta treated with denosumab products, including Prolia. Some cases required hospitalization [see Pediatric Use (8.4)].
6. Adverse Reactions/Side Effects
The following serious adverse reactions are discussed below and also elsewhere in the labeling:
- Hypocalcemia [see Warnings and Precautions (5.3)]
- Serious Infections [see Warnings and Precautions (5.7)]
- Dermatologic Adverse Reactions [see Warnings and Precautions (5.8)]
- Osteonecrosis of the Jaw [see Warnings and Precautions (5.4)]
- Atypical Subtrochanteric and Diaphyseal Femoral Fractures [see Warnings and Precautions (5.5)]
- Multiple Vertebral Fractures (MVF) Following Discontinuation of Prolia Treatment [see Warnings and Precautions (5.6)]
The most common adverse reactions reported with Prolia in patients with postmenopausal osteoporosis are back pain, pain in extremity, musculoskeletal pain, hypercholesterolemia, and cystitis.
The most common adverse reactions reported with Prolia in men with osteoporosis are back pain, arthralgia, and nasopharyngitis.
The most common adverse reactions reported with Prolia in patients with glucocorticoid-induced osteoporosis are back pain, hypertension, bronchitis, and headache.
The most common (per patient incidence ≥ 10%) adverse reactions reported with Prolia in patients with bone loss receiving androgen deprivation therapy for prostate cancer or adjuvant aromatase inhibitor therapy for breast cancer are arthralgia and back pain. Pain in extremity and musculoskeletal pain have also been reported in clinical trials.
The most common adverse reactions leading to discontinuation of Prolia in patients with postmenopausal osteoporosis are back pain and constipation.
To report Adverse Reactions with Prolia®, please call Amgen Medical Information at 1-800-772-6436, email [email protected], or report the event at FDA MedWatch.
6.1 Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in clinical practice.
Treatment of Postmenopausal Women with Osteoporosis
The safety of Prolia in the treatment of postmenopausal osteoporosis was assessed in a 3-year, randomized, double-blind, placebo-controlled, multinational study of 7808 postmenopausal women aged 60 to 91 years. A total of 3876 women were exposed to placebo and 3886 women were exposed to Prolia administered subcutaneously once every 6 months as a single 60 mg dose. All women were instructed to take at least 1000 mg of calcium and 400 IU of vitamin D supplementation per day.
The incidence of all-cause mortality was 2.3% (n = 90) in the placebo group and 1.8% (n = 70) in the Prolia group. The incidence of nonfatal serious adverse events was 24.2% in the placebo group and 25.0% in the Prolia group. The percentage of patients who withdrew from the study due to adverse events was 2.1% and 2.4% for the placebo and Prolia groups, respectively.
Adverse reactions reported in ≥ 2% of postmenopausal women with osteoporosis and more frequently in the Prolia-treated women than in the placebo-treated women are shown in the table below.
| SYSTEM ORGAN CLASS Preferred Term | Prolia (N = 3886) n (%) | Placebo (N = 3876) n (%) |
|---|---|---|
| BLOOD AND LYMPHATIC SYSTEM DISORDERS | ||
| Anemia | 129 (3.3) | 107 (2.8) |
| CARDIAC DISORDERS | ||
| Angina pectoris | 101 (2.6) | 87 (2.2) |
| Atrial fibrillation | 79 (2.0) | 77 (2.0) |
| EAR AND LABYRINTH DISORDERS | ||
| Vertigo | 195 (5.0) | 187 (4.8) |
| GASTROINTESTINAL DISORDERS | ||
| Abdominal pain upper | 129 (3.3) | 111 (2.9) |
| Flatulence | 84 (2.2) | 53 (1.4) |
| Gastroesophageal reflux disease | 80 (2.1) | 66 (1.7) |
| GENERAL DISORDERS AND ADMINISTRATION SITE CONDITIONS | ||
| Edema peripheral | 189 (4.9) | 155 (4.0) |
| Asthenia | 90 (2.3) | 73 (1.9) |
| INFECTIONS AND INFESTATIONS | ||
| Cystitis | 228 (5.9) | 225 (5.8) |
| Upper respiratory tract infection | 190 (4.9) | 167 (4.3) |
| Pneumonia | 152 (3.9) | 150 (3.9) |
| Pharyngitis | 91 (2.3) | 78 (2.0) |
| Herpes zoster | 79 (2.0) | 72 (1.9) |
| METABOLISM AND NUTRITION DISORDERS | ||
| Hypercholesterolemia | 280 (7.2) | 236 (6.1) |
| MUSCULOSKELETAL AND CONNECTIVE TISSUE DISORDERS | ||
| Back pain | 1347 (34.7) | 1340 (34.6) |
| Pain in extremity | 453 (11.7) | 430 (11.1) |
| Musculoskeletal pain | 297 (7.6) | 291 (7.5) |
| Bone pain | 142 (3.7) | 117 (3.0) |
| Myalgia | 114 (2.9) | 94 (2.4) |
| Spinal osteoarthritis | 82 (2.1) | 64 (1.7) |
| NERVOUS SYSTEM DISORDERS | ||
| Sciatica | 178 (4.6) | 149 (3.8) |
| PSYCHIATRIC DISORDERS | ||
| Insomnia | 126 (3.2) | 122 (3.1) |
| SKIN AND SUBCUTANEOUS TISSUE DISORDERS | ||
| Rash | 96 (2.5) | 79 (2.0) |
| Pruritus | 87 (2.2) | 82 (2.1) |
Treatment of Glucocorticoid-Induced Osteoporosis
The safety of Prolia in the treatment of glucocorticoid-induced osteoporosis was assessed in the 1-year, primary analysis of a 2-year randomized, multicenter, double-blind, parallel-group, active-controlled study of 795 patients (30% men and 70% women) aged 20 to 94 (mean age of 63 years) treated with greater than or equal to 7.5 mg/day oral prednisone (or equivalent). A total of 384 patients were exposed to 5 mg oral daily bisphosphonate (active-control) and 394 patients were exposed to Prolia administered once every 6 months as a 60 mg subcutaneous dose. All patients were instructed to take at least 1000 mg of calcium and 800 IU of vitamin D supplementation per day.
The incidence of all-cause mortality was 0.5% (n = 2) in the active-control group and 1.5% (n = 6) in the Prolia group. The incidence of serious adverse events was 17% in the active-control group and 16% in the Prolia group. The percentage of patients who withdrew from the study due to adverse events was 3.6% and 3.8% for the active-control and Prolia groups, respectively.
Adverse reactions reported in ≥ 2% of patients with glucocorticoid-induced osteoporosis and more frequently with Prolia than in the active-control-treated patients are shown in the table below.
| Preferred Term | Prolia (N = 394) n (%) | Oral Daily Bisphosphonate (Active-Control) (N = 384) n (%) |
|---|---|---|
|
||
| Back pain | 18 (4.6) | 17 (4.4) |
| Hypertension | 15 (3.8) | 13 (3.4) |
| Bronchitis | 15 (3.8) | 11 (2.9) |
| Headache | 14 (3.6) | 7 (1.8) |
| Dyspepsia | 12 (3.0) | 10 (2.6) |
| Urinary tract infection | 12 (3.0) | 8 (2.1) |
| Abdominal pain upper | 12 (3.0) | 7 (1.8) |
| Upper respiratory tract infection | 11 (2.8) | 10 (2.6) |
| Constipation | 11 (2.8) | 6 (1.6) |
| Vomiting | 10 (2.5) | 6 (1.6) |
| Dizziness | 9 (2.3) | 8 (2.1) |
| Fall | 8 (2.0) | 7 (1.8) |
| Polymyalgia rheumatica* | 8 (2.0) | 1 (0.3) |
6.2 Postmarketing Experience
Because postmarketing reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following adverse reactions have been identified during post approval use of Prolia:
- Drug-related hypersensitivity reactions: anaphylaxis, rash, urticaria, facial swelling, and erythema
- Hypocalcemia: severe symptomatic hypocalcemia
- Musculoskeletal pain, including severe cases
- Parathyroid hormone (PTH): Marked elevation in serum PTH in patients with severe renal impairment (creatinine clearance < 30 mL/min) or receiving dialysis
- Multiple vertebral fractures following discontinuation of Prolia
- Cutaneous and mucosal lichenoid drug eruptions (e.g. lichen planus-like reactions)
- Alopecia
- Vasculitis (e.g. ANCA positive vasculitis, leukocytoclastic vasculitis)
- Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome
6.3 Immunogenicity
Denosumab is a human monoclonal antibody. As with all therapeutic proteins, there is potential for immunogenicity. Using an electrochemiluminescent bridging immunoassay, less than 1% (55 out of 8113) of patients treated with Prolia for up to 5 years tested positive for binding antibodies (including pre-existing, transient, and developing antibodies). None of the patients tested positive for neutralizing antibodies, as was assessed using a chemiluminescent cell-based in vitro biological assay. No evidence of altered pharmacokinetic profile, toxicity profile, or clinical response was associated with binding antibody development.
The incidence of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of a positive antibody (including neutralizing antibody) test result may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of antibodies to denosumab with the incidence of antibodies to other products may be misleading.
8. Use In Specific Populations
8.3 Females and Males of Reproductive Potential
Based on findings in animals, Prolia can cause fetal harm when administered to a pregnant woman [see Use in Specific Populations (8.1)].
8.4 Pediatric Use
The safety and effectiveness of Prolia in pediatric patients have not been established. Prolia is not approved for use in pediatric patients.
In clinical trials, hypercalcemia has been reported in pediatric patients with osteogenesis imperfecta treated with denosumab products, including Prolia. Some cases required hospitalization and were complicated by acute renal injury [see Warnings and Precautions (5.11)]. Based on results from animal studies, Prolia may negatively affect long-bone growth and dentition in pediatric patients below the age of 4 years.
8.5 Geriatric Use
Of the total number of patients in clinical studies of Prolia, 9943 patients (76%) were ≥ 65 years old, while 3576 (27%) were ≥ 75 years old. Of the patients in the osteoporosis study in men, 133 patients (55%) were ≥ 65 years old, while 39 patients (16%) were ≥ 75 years old. Of the patients in the glucocorticoid-induced osteoporosis study, 355 patients (47%) were ≥ 65 years old, while 132 patients (17%) were ≥ 75 years old. No overall differences in safety or efficacy were observed between these patients and younger patients, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out.
8.6 Renal Impairment
No dose adjustment is necessary in patients with renal impairment.
In clinical studies, patients with severe renal impairment (creatinine clearance < 30 mL/min) or receiving dialysis were at greater risk of developing hypocalcemia. Consider the benefit-risk profile when administering Prolia to patients with severe renal impairment or receiving dialysis. Clinical monitoring of calcium and mineral levels (phosphorus and magnesium) is highly recommended. Adequate intake of calcium and vitamin D is important in patients with severe renal impairment or receiving dialysis [see Warnings and Precautions (5.3), Adverse Reactions (6.1) and Clinical Pharmacology (12.3)].
11. Prolia Description
Prolia (denosumab) is a human IgG2 monoclonal antibody with affinity and specificity for human RANKL (receptor activator of nuclear factor kappa-B ligand). Denosumab has an approximate molecular weight of 147 kDa and is produced in genetically engineered mammalian (Chinese hamster ovary) cells.
Prolia is a sterile, preservative-free, clear, colorless to pale yellow solution.
Each 1 mL single-dose prefilled syringe of Prolia contains 60 mg denosumab (60 mg/mL solution), 4.7% sorbitol, 17 mM acetate, 0.01% polysorbate 20, Water for Injection (USP), and sodium hydroxide to a pH of 5.2.
12. Prolia - Clinical Pharmacology
12.1 Mechanism of Action
Prolia binds to RANKL, a transmembrane or soluble protein essential for the formation, function, and survival of osteoclasts, the cells responsible for bone resorption. Prolia prevents RANKL from activating its receptor, RANK, on the surface of osteoclasts and their precursors. Prevention of the RANKL/RANK interaction inhibits osteoclast formation, function, and survival, thereby decreasing bone resorption and increasing bone mass and strength in both cortical and trabecular bone.
12.2 Pharmacodynamics
In clinical studies, treatment with 60 mg of Prolia resulted in reduction in the bone resorption marker serum type 1 C-telopeptide (CTX) by approximately 85% by 3 days, with maximal reductions occurring by 1 month. CTX levels were below the limit of assay quantitation (0.049 ng/mL) in 39% to 68% of patients 1 to 3 months after dosing of Prolia. At the end of each dosing interval, CTX reductions were partially attenuated from a maximal reduction of ≥ 87% to ≥ 45% (range: 45% to 80%), as serum denosumab levels diminished, reflecting the reversibility of the effects of Prolia on bone remodeling. These effects were sustained with continued treatment. Upon reinitiation, the degree of inhibition of CTX by Prolia was similar to that observed in patients initiating Prolia treatment.
Consistent with the physiological coupling of bone formation and resorption in skeletal remodeling, subsequent reductions in bone formation markers (i.e. osteocalcin and procollagen type 1 N-terminal peptide [P1NP]) were observed starting 1 month after the first dose of Prolia. After discontinuation of Prolia therapy, markers of bone resorption increased to levels 40% to 60% above pretreatment values but returned to baseline levels within 12 months.
12.3 Pharmacokinetics
In a study conducted in healthy male and female volunteers (n = 73, age range: 18 to 64 years) following a single subcutaneously administered Prolia dose of 60 mg after fasting (at least for 12 hours), the mean maximum denosumab concentration (Cmax) was 6.75 mcg/mL (standard deviation [SD] = 1.89 mcg/mL). The median time to maximum denosumab concentration (Tmax) was 10 days (range: 3 to 21 days). After Cmax, serum denosumab concentrations declined over a period of 4 to 5 months with a mean half-life of 25.4 days (SD = 8.5 days; n = 46). The mean area-under-the-concentration-time curve up to 16 weeks (AUC0-16 weeks) of denosumab was 316 mcg∙day/mL (SD = 101 mcg∙day/mL).
No accumulation or change in denosumab pharmacokinetics with time was observed upon multiple dosing of 60 mg subcutaneously administered once every 6 months.
Prolia pharmacokinetics were not affected by the formation of binding antibodies.
A population pharmacokinetic analysis was performed to evaluate the effects of demographic characteristics. This analysis showed no notable differences in pharmacokinetics with age (in postmenopausal women), race, or body weight (36 to 140 kg).
13. Nonclinical Toxicology
13.2 Animal Toxicology and/or Pharmacology
Denosumab is an inhibitor of osteoclastic bone resorption via inhibition of RANKL.
In ovariectomized monkeys, once-monthly treatment with denosumab suppressed bone turnover and increased BMD and strength of cancellous and cortical bone at doses 50-fold higher than the recommended human dose of 60 mg administered once every 6 months, based on body weight (mg/kg). Bone tissue was normal with no evidence of mineralization defects, accumulation of osteoid, or woven bone.
Because the biological activity of denosumab in animals is specific to nonhuman primates, evaluation of genetically engineered ("knockout") mice or use of other biological inhibitors of the RANK/RANKL pathway, namely OPG-Fc, provided additional information on the pharmacodynamic properties of denosumab. RANK/RANKL knockout mice exhibited absence of lymph node formation, as well as an absence of lactation due to inhibition of mammary gland maturation (lobulo-alveolar gland development during pregnancy). Neonatal RANK/RANKL knockout mice exhibited reduced bone growth and lack of tooth eruption. A corroborative study in 2-week-old rats given the RANKL inhibitor OPG-Fc also showed reduced bone growth, altered growth plates, and impaired tooth eruption. These changes were partially reversible in this model when dosing with the RANKL inhibitors was discontinued.
14. Clinical Studies
14.1 Treatment of Postmenopausal Women with Osteoporosis
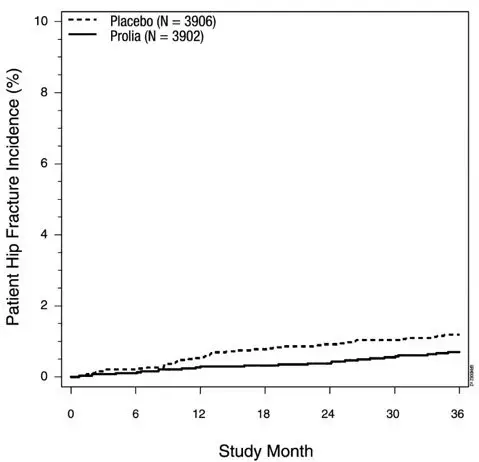
The efficacy and safety of Prolia in the treatment of postmenopausal osteoporosis was demonstrated in a 3-year, randomized, double-blind, placebo-controlled trial. Enrolled women had a baseline BMD T-score between -2.5 and -4.0 at either the lumbar spine or total hip. Women with other diseases (such as rheumatoid arthritis, osteogenesis imperfecta, and Paget's disease) or on therapies that affect bone were excluded from this study. The 7808 enrolled women were aged 60 to 91 years with a mean age of 72 years. Overall, the mean baseline lumbar spine BMD T-score was -2.8, and 23% of women had a vertebral fracture at baseline. Women were randomized to receive subcutaneous injections of either placebo (N = 3906) or Prolia 60 mg (N = 3902) once every 6 months. All women received at least 1000 mg calcium and 400 IU vitamin D supplementation daily.
The primary efficacy variable was the incidence of new morphometric (radiologically-diagnosed) vertebral fractures at 3 years. Vertebral fractures were diagnosed based on lateral spine radiographs (T4-L4) using a semiquantitative scoring method. Secondary efficacy variables included the incidence of hip fracture and nonvertebral fracture, assessed at 3 years.
Effect on Vertebral Fractures
Prolia significantly reduced the incidence of new morphometric vertebral fractures at 1, 2, and 3 years (p < 0.0001), as shown in Table 3. The incidence of new vertebral fractures at year 3 was 7.2% in the placebo-treated women compared to 2.3% for the Prolia-treated women. The absolute risk reduction was 4.8% and relative risk reduction was 68% for new morphometric vertebral fractures at year 3.
| Proportion of Women with Fracture (%)* | Absolute Risk Reduction (%)†
(95% CI) | Relative Risk Reduction (%)†
(95% CI) |
||
|---|---|---|---|---|
| Placebo N = 3691 (%) | Prolia N = 3702 (%) |
|||
|
||||
| 0-1 Year | 2.2 | 0.9 | 1.4 (0.8, 1.9) | 61 (42, 74) |
| 0-2 Years | 5.0 | 1.4 | 3.5 (2.7, 4.3) | 71 (61, 79) |
| 0-3 Years | 7.2 | 2.3 | 4.8 (3.9, 5.8) | 68 (59, 74) |
Prolia was effective in reducing the risk for new morphometric vertebral fractures regardless of age, baseline rate of bone turnover, baseline BMD, baseline history of fracture, or prior use of a drug for osteoporosis.
Effect on Nonvertebral Fractures
Treatment with Prolia resulted in a significant reduction in the incidence of nonvertebral fractures (Table 4).
| Proportion of Women with Fracture (%)* | Absolute Risk Reduction (%) (95% CI) | Relative Risk Reduction (%) (95% CI) |
||
|---|---|---|---|---|
| Placebo N = 3906 (%) | Prolia N = 3902 (%) |
|||
|
||||
| Nonvertebral fracture† | 8.0 | 6.5 | 1.5 (0.3, 2.7) | 20 (5, 33)‡ |
14.2 Treatment to Increase Bone Mass in Men with Osteoporosis
The efficacy and safety of Prolia in the treatment to increase bone mass in men with osteoporosis was demonstrated in a 1-year, randomized, double-blind, placebo-controlled trial. Enrolled men had a baseline BMD T-score between -2.0 and -3.5 at the lumbar spine or femoral neck. Men with a BMD T-score between -1.0 and -3.5 at the lumbar spine or femoral neck were also enrolled if there was a history of prior fragility fracture. Men with other diseases (such as rheumatoid arthritis, osteogenesis imperfecta, and Paget's disease) or on therapies that may affect bone were excluded from this study. The 242 men enrolled in the study ranged in age from 31 to 84 years with a mean age of 65 years. Men were randomized to receive SC injections of either placebo (n = 121) or Prolia 60 mg (n = 121) once every 6 months. All men received at least 1000 mg calcium and at least 800 IU vitamin D supplementation daily.
14.3 Treatment of Glucocorticoid-Induced Osteoporosis
The efficacy and safety of Prolia in the treatment of patients with glucocorticoid-induced osteoporosis was assessed in the 12-month primary analysis of a 2-year, randomized, multicenter, double-blind, parallel-group, active-controlled study (NCT 01575873) of 795 patients (70% women and 30% men) aged 20 to 94 years (mean age of 63 years) treated with greater than or equal to 7.5 mg/day oral prednisone (or equivalent) for < 3 months prior to study enrollment and planning to continue treatment for a total of at least 6 months (glucocorticoid-initiating subpopulation; n = 290) or ≥ 3 months prior to study enrollment and planning to continue treatment for a total of at least 6 months (glucocorticoid-continuing subpopulation, n = 505). Enrolled patients < 50 years of age were required to have a history of osteoporotic fracture. Enrolled patients ≥ 50 years of age who were in the glucocorticoid-continuing subpopulation were required to have a baseline BMD T-score of ≤ -2.0 at the lumbar spine, total hip, or femoral neck; or a BMD T-score ≤ -1.0 at the lumbar spine, total hip, or femoral neck and a history of osteoporotic fracture.
Patients were randomized (1:1) to receive either an oral daily bisphosphonate (active-control, risedronate 5 mg once daily) (n = 397) or Prolia 60 mg subcutaneously once every 6 months (n = 398) for one year. Randomization was stratified by gender within each subpopulation. Patients received at least 1000 mg calcium and 800 IU vitamin D supplementation daily.
14.4 Treatment of Bone Loss in Men with Prostate Cancer
The efficacy and safety of Prolia in the treatment of bone loss in men with nonmetastatic prostate cancer receiving androgen deprivation therapy (ADT) were demonstrated in a 3-year, randomized (1:1), double-blind, placebo-controlled, multinational study. Men less than 70 years of age had either a BMD T-score at the lumbar spine, total hip, or femoral neck between -1.0 and -4.0, or a history of an osteoporotic fracture. The mean baseline lumbar spine BMD T-score was -0.4, and 22% of men had a vertebral fracture at baseline. The 1468 men enrolled ranged in age from 48 to 97 years (median 76 years). Men were randomized to receive subcutaneous injections of either placebo (n = 734) or Prolia 60 mg (n = 734) once every 6 months for a total of 6 doses. Randomization was stratified by age (< 70 years vs. ≥ 70 years) and duration of ADT at trial entry (≤ 6 months vs. > 6 months). Seventy-nine percent of patients received ADT for more than 6 months at study entry. All men received at least 1000 mg calcium and 400 IU vitamin D supplementation daily.
Effect on Vertebral Fractures
Prolia significantly reduced the incidence of new vertebral fractures at 3 years (p = 0.0125), as shown in Table 5.
| Proportion of Men with Fracture (%)* | Absolute Risk Reduction (%)†
(95% CI) | Relative Risk Reduction (%)†
(95% CI) |
||
|---|---|---|---|---|
| Placebo N = 673 (%) | Prolia N = 679 (%) |
|||
|
||||
| 0-1 Year | 1.9 | 0.3 | 1.6 (0.5, 2.8) | 85 (33, 97) |
| 0-2 Years | 3.3 | 1.0 | 2.2 (0.7, 3.8) | 69 (27, 86) |
| 0-3 Years | 3.9 | 1.5 | 2.4 (0.7, 4.1) | 62 (22, 81) |
14.5 Treatment of Bone Loss in Women with Breast Cancer
The efficacy and safety of Prolia in the treatment of bone loss in women receiving adjuvant aromatase inhibitor (AI) therapy for breast cancer was assessed in a 2-year, randomized (1:1), double-blind, placebo-controlled, multinational study. Women had baseline BMD T-scores between -1.0 to -2.5 at the lumbar spine, total hip, or femoral neck, and had not experienced fracture after age 25. The mean baseline lumbar spine BMD T-score was -1.1, and 2.0% of women had a vertebral fracture at baseline. The 252 women enrolled ranged in age from 35 to 84 years (median 59 years). Women were randomized to receive subcutaneous injections of either placebo (n = 125) or Prolia 60 mg (n = 127) once every 6 months for a total of 4 doses. Randomization was stratified by duration of adjuvant AI therapy at trial entry (≤ 6 months vs. > 6 months). Sixty-two percent of patients received adjuvant AI therapy for more than 6 months at study entry. All women received at least 1000 mg calcium and 400 IU vitamin D supplementation daily.
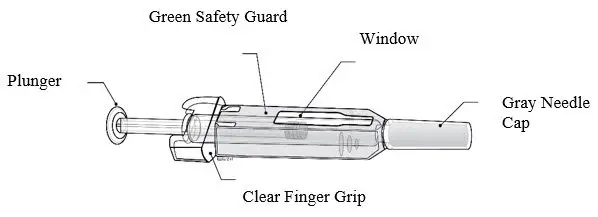
16. How is Prolia supplied
Prolia is supplied in a single-dose prefilled syringe with a safety guard. The prefilled syringe is not made with natural rubber latex.
| 60 mg/1 mL in a single-dose prefilled syringe | 1 per carton | NDC 55513-710-01 |
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
| This Medication Guide has been approved by the U.S. Food and Drug Administration. | Revised: 05/2022 | ||
| Medication Guide Prolia® (PRÓ-lee-a) (denosumab) Injection, for subcutaneous use |
|||
|
What is the most important information I should know about Prolia? |
|||
| If you receive Prolia, you should not receive XGEVA®. Prolia contains the same medicine as Xgeva (denosumab). | |||
| Prolia can cause serious side effects including: | |||
|
|||
|
|
||
|
|||
|
|
||
|
|||
| What is Prolia? | |||
| Prolia is a prescription medicine used to: | |||
|
|||
| It is not known if Prolia is safe and effective in children. Prolia is not approved for use in children. | |||
Do not take Prolia if you:
|
|||
| Before taking Prolia, tell your doctor about all of your medical conditions, including if you: | |||
|
|||
| Tell your doctor about all the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. Know the medicines you take. Keep a list of medicines with you to show to your doctor or pharmacist when you get a new medicine. |
|||
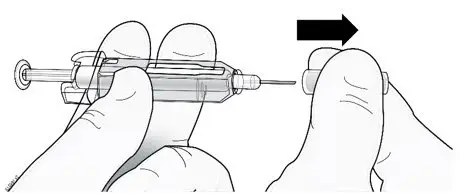
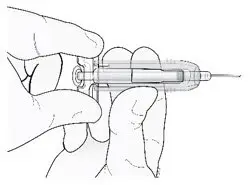
| How will I receive Prolia? | |||
|
|||
| What are the possible side effects of Prolia? | |||
| Prolia may cause serious side effects. | |||
|
|||
| The most common side effects of Prolia in women who are being treated for osteoporosis after menopause are: | |||
|
|
||
| The most common side effects of Prolia in men with osteoporosis are: | |||
|
|
||
| The most common side effects of Prolia in patients with glucocorticoid-induced osteoporosis are: | |||
|
|
||
| The most common side effects of Prolia in patients receiving certain treatments for prostate or breast cancer are: | |||
|
|
||
| Tell your doctor if you have any side effect that bothers you or that does not go away. | |||
| These are not all the possible side effects of Prolia. | |||
| Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. | |||
| How should I store Prolia if I need to pick it up from a pharmacy? | |||
|
|||
| Keep Prolia and all medicines out of the reach of children. | |||
| General information about the safe and effective use of Prolia. | |||
| Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use Prolia for a condition for which it was not prescribed. Do not give Prolia to other people, even if they have the same symptoms that you have. It may harm them. You can ask your doctor or pharmacist for information about Prolia that is written for health professionals. | |||
| What are the ingredients in Prolia? Active ingredient: denosumab Inactive ingredients: sorbitol, acetate, polysorbate 20, Water for Injection (USP), and sodium hydroxide |
|||
| Amgen Inc. One Amgen Center Drive Thousand Oaks, California 91320-1799 1xxxxxx – v16 For more information, go to www.Prolia.com or call Amgen at 1-800-772-6436. |
|||
| PROLIA
denosumab injection |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Amgen Inc (039976196) |
