Drug Detail:Sucraid (Sacrosidase [ sak-roe-si-dase ])
Drug Class: Digestive enzymes
Sucraid Description
Sucraid® (sacrosidase) Oral Solution is an enzyme replacement therapy for the treatment of genetically determined sucrase deficiency, which is part of congenital sucrase-isomaltase deficiency (CSID).
Sucraid - Clinical Pharmacology
Congenital sucrase-isomaltase deficiency (CSID) is a chronic, autosomal recessive, inherited, phenotypically heterogeneous disease with very variable enzyme activity. CSID is usually characterized by a complete or almost complete lack of endogenous sucrase activity, a very marked reduction in isomaltase activity, a moderate decrease in maltase activity, and normal lactase levels.
Sucrase is naturally produced in the brush border of the small intestine, primarily the distal duodenum and jejunum. Sucrase hydrolyzes the disaccharide sucrose into its component monosaccharides, glucose and fructose. Isomaltase breaks down disaccharides from starch into simple sugars. Sucraid does not contain isomaltase.
In the absence of endogenous human sucrase, as in CSID, sucrose is not metabolized. Unhydrolyzed sucrose and starch are not absorbed from the intestine and their presence in the intestinal lumen may lead to osmotic retention of water. This may result in loose stools.
Unabsorbed sucrose in the colon is fermented by bacterial flora to produce increased amounts of hydrogen, methane, and water. As a consequence, excessive gas, bloating, abdominal cramps, nausea, and vomiting may occur.
Chronic malabsorption of disaccharides may result in malnutrition. Undiagnosed/untreated CSID patients often fail to thrive and fall behind in their expected growth and development curves. Previously, the treatment of CSID has required the continual use of a strict sucrose-free diet.
CSID is often difficult to diagnose. Approximately 4% to 10% of pediatric patients with chronic diarrhea of unknown origin have CSID. Measurement of expired breath hydrogen under controlled conditions following a sucrose challenge (a measurement of excess hydrogen excreted in exhalation) in CSID patients has shown levels as great as 6 times that in normal subjects.
A generally accepted clinical definition of CSID is a condition characterized by the following: stool pH <6, an increase in breath hydrogen of > 10 ppm when challenged with sucrose after fasting and a negative lactose breath test. However, because of the difficulties in diagnosing CSID, it may be warranted to conduct a short therapeutic trial (e.g., one week) to assess response in patients suspected of having CSID.
Clinical Studies
A two-phase (dose response preceded by a breath hydrogen phase) double-blind, multi-site, crossover trial was conducted in 28 patients (aged 4 months to 11.5 years) with confirmed CSID. During the dose response phase, the patients were challenged with an ordinary sucrose-containing diet while receiving each of four doses of sacrosidase: full strength (9000 I.U./mL) and three dilutions (1:10 [900 I.U./mL], 1:100 [90 I.U./mL], and 1:1000 [9 I.U./mL]) in random order for a period of 10 days. Patients who weighed no more than 15 kg received 1 mL per meal; those weighing more than 15 kg received 2 mL per meal. The dose did not vary with age or sucrose intake. A dose-response relationship was shown between the two higher and the two lower doses. The two higher doses of sacrosidase were associated with significantly fewer total stools and higher proportions of patients having lower total symptom scores, the primary efficacy end-points. In addition, higher doses of sacrosidase were associated with a significantly greater number of hard and formed stools as well as with fewer watery and soft stools, the secondary efficacy end-points.
Analysis of the overall symptomatic response as a function of age indicated that in CSID patients up to 3 years of age, 86% became asymptomatic. In patients over 3 years of age, 77% became asymptomatic. Thus, the therapeutic response did not differ significantly according to age.
A second study of similar design and execution as the first used 4 different dilutions of sacrosidase: 1:100 (90 I.U./mL), 1:1000 (9 I.U./mL), 1:10,000 (0.9 I.U./mL), and 1:100,000 (0.09 I.U./mL). There were inconsistent results with regards to the primary efficacy parameters.
In both trials, however, patients showed a marked decrease in breath hydrogen output when they received sacrosidase in comparison to placebo.
Indications and Usage for Sucraid
Sucraid® (sacrosidase) Oral Solution is indicated as oral replacement therapy of the genetically determined sucrase deficiency, which is part of congenital sucrase-isomaltase deficiency (CSID).
Contraindications
Patients known to be hypersensitive to yeast, yeast products, glycerin (glycerol), or papain.
Warnings
Severe wheezing, 90 minutes after a second dose of sacrosidase, necessitated admission into the ICU for a 4-year-old boy. The wheezing was probably caused by sacrosidase. He had asthma and was being treated with steroids. A skin test for sacrosidase was positive.
Other serious events have not been linked to Sucraid.
Precautions
Care should be taken to administer initial doses of Sucraid near (within a few minutes of travel) a facility where acute hypersensitivity reactions can be adequately treated. Alternatively, the patient may be tested for hypersensitivity to Sucraid through skin abrasion testing. Should symptoms of hypersensitivity appear, discontinue medication and initiate symptomatic and supportive therapy.
Skin testing as a rechallenge has been used to verify hypersensitivity in one asthmatic child who displayed wheezing after oral sacrosidase.
GENERAL
Although Sucraid provides replacement therapy for the deficient sucrase, it does not provide specific replacement therapy for the deficient isomaltase. Therefore, restricting starch in the diet may still be necessary to reduce symptoms as much as possible. The need for dietary starch restriction for patients using Sucraid should be evaluated in each patient.
It may sometimes be clinically inappropriate, difficult, or inconvenient to perform a small bowel biopsy or breath hydrogen test to make a definitive diagnosis of CSID. If the diagnosis is in doubt, it may be warranted to conduct a short therapeutic trial (e.g., one week) with Sucraid to assess response in a patient suspected of sucrase deficiency.
The effects of Sucraid have not been evaluated in patients with secondary (acquired) disaccharidase deficiencies.
Adverse Reactions/Side Effects
Adverse experiences with Sucraid in clinical trials were generally minor and were frequently associated with the underlying disease.
In clinical studies of up to 54 months duration, physicians treated a total of 52 patients with Sucraid. The adverse experiences and respective number of patients reporting each event (in parenthesis) were as follows: abdominal pain (4), vomiting (3), nausea (2), diarrhea (2), constipation (2), insomnia (1), headache (1), nervousness (1), and dehydration (1).
Note: diarrhea and abdominal pain can be a part of the clinical presentation of the genetically determined sucrase deficiency, which is part of congenital sucrase-isomaltase deficiency (CSID).
One asthmatic child experienced a serious hypersensitivity reaction (wheezing) probably related to sacrosidase (seeWarnings). The event resulted in withdrawal of the patient from the trial but resolved with no sequelae.
Sucraid Dosage and Administration
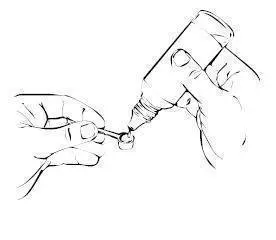
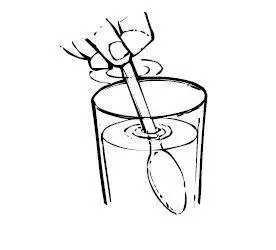
The recommended dosage is 1 or 2 mL (8,500 to 17,000 I.U.) or 1 or 2 full measuring scoops (each full measuring scoop equals 1 mL; 28 drops from the Sucraid container tip equals 1 mL) taken orally with each meal or snack diluted with 2 to 4 ounces (60 to 120 mL) of water, milk, or infant formula. The beverage or infant formula should be served cold or at room temperature. The beverage or infant formula should not be warmed or heated before or after addition of Sucraid because heating is likely to decrease potency. Sucraid should not be reconstituted or consumed with fruit juice since its acidity may reduce the enzyme activity.
It is recommended that approximately half of the dosage be taken at the beginning of the meal or snack and the remainder be taken during the meal or snack.
The recommended dosage is as follows:
1 mL (8,500 I.U.) (one full measuring scoop or 28 drops) per meal or snack for patients up to 15 kg in body weight.
2 mL (17,000 I.U.) (two full measuring scoops or 56 drops) per meal or snack for patients over 15 kg in body weight.
Dosage may be measured with the 1 mL measuring scoop (provided) or by drop count method (1 mL equals 28 drops from the Sucraid container tip).
How is Sucraid supplied
Sucraid® (sacrosidase) Oral Solution is available in 118 mL (4 fluid ounces) translucent plastic bottles, packaged two bottles per box. Each mL of solution contains 8,500 International Units (I.U.) of sacrosidase. A 1 mL measuring scoop is provided with each bottle. A full measuring scoop is 1 mL.
Store in a refrigerator at 2°- 8°C (36°- 46°F). Discard four weeks after first opening due to the potential for bacterial growth. Protect from heat and light.
Rx only.
Distributed by:
QOL Medical, LLC
Vero Beach, FL 32963
To order, or for any questions, call 1-866-469-3773
www.sucraid.net
NDC# 67871-111-04
| SUCRAID
sacrosidase solution |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - QOL Medical, LLC (140026258) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| Lyophilization Services of New England, Inc. (LSNE) | 028180765 | manufacture(67871-111) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| QOL MEDICAL | 104085889 | api manufacture(67871-111) , analysis(67871-111) | |
