Drug Detail:Alecensa (Alectinib)
Drug Class: Multikinase inhibitors
Highlights of Prescribing Information
ALECENSA® (alectinib) capsules, for oral use
Initial U.S. Approval: 2015
Recent Major Changes
| Dosage and Administration (2.1) | 1/2021 |
| Warnings and Precautions (5.6) | 9/2021 |
Indications and Usage for Alecensa
ALECENSA is a kinase inhibitor indicated for the treatment of patients with anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) as detected by an FDA-approved test. (1)
Alecensa Dosage and Administration
600 mg orally twice daily. Administer ALECENSA with food. (2.2)
Dosage Forms and Strengths
Capsules: 150 mg (3)
Contraindications
None. (4)
Warnings and Precautions
- Hepatotoxicity: Monitor liver laboratory tests every 2 weeks during the first 3 months of treatment, then once a month and as clinically indicated, with more frequent testing in patients who develop transaminase and bilirubin elevations. In case of severe ALT, AST, or bilirubin elevations, withhold, then reduce dose, or permanently discontinue ALECENSA. (2.3, 5.1)
- Interstitial Lung Disease (ILD)/Pneumonitis: Immediately withhold ALECENSA in patients diagnosed with ILD/pneumonitis and permanently discontinue if no other potential causes of ILD/pneumonitis have been identified. (2.3, 5.2)
- Renal Impairment: Withhold ALECENSA for severe renal impairment, then resume ALECENSA at reduced dose upon recovery or permanently discontinue (2.3, 5.3).
- Bradycardia: Monitor heart rate and blood pressure regularly. If symptomatic, withhold ALECENSA then reduce dose, or permanently discontinue. (2.3, 5.4)
- Severe Myalgia and Creatine Phosphokinase (CPK) Elevation: Assess CPK every 2 weeks during the first month of treatment and in patients reporting unexplained muscle pain, tenderness, or weakness. In case of severe CPK elevations, withhold, then resume or reduce dose. (2.3, 5.5)
- Hemolytic Anemia: If hemolytic anemia is suspected, withhold ALECENSA. If hemolytic anemia is confirmed, consider resuming at a reduced dose upon resolution or permanently discontinue. (5.6)
- Embryo-Fetal Toxicity: ALECENSA can cause fetal harm. Advise females of reproductive potential of the potential risk to a fetus and to use effective contraception. (5.7, 8.1, 8.3)
Adverse Reactions/Side Effects
The most common adverse reactions (incidence ≥20%) were fatigue, constipation, edema, myalgia, and anemia. (6)
To report SUSPECTED ADVERSE REACTIONS, contact Genentech at 1-888-835-2555 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Use In Specific Populations
Lactation: Do not breastfeed. (8.2)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 9/2021
Full Prescribing Information
1. Indications and Usage for Alecensa
ALECENSA is indicated for the treatment of patients with anaplastic lymphoma kinase (ALK)-positive metastatic non-small cell lung cancer (NSCLC) as detected by an FDA-approved test.
2. Alecensa Dosage and Administration
2.1 Patient Selection
Select patients for the treatment of metastatic NSCLC with ALECENSA based on the presence of ALK positivity in tumor tissue or plasma specimens [see Indications and Usage (1) and Clinical Studies (14)]. If ALK rearrangements are not detected in a plasma specimen, test tumor tissue if feasible.
Information on FDA-approved tests for the detection of ALK rearrangements in NSCLC is available at http://www.fda.gov/CompanionDiagnostics.
2.2 Dosing and Administration
The recommended dose of ALECENSA is 600 mg orally twice daily [see Clinical Pharmacology (12.3)]. Administer ALECENSA until disease progression or unacceptable toxicity.
The recommended dose of ALECENSA in patients with severe hepatic impairment (Child-Pugh C) is 450 mg orally twice daily [see Use in Specific Populations (8.7) and Clinical Pharmacology (12.3)].
ALECENSA should be taken with food. Do not open or dissolve the contents of the capsule. If a dose of ALECENSA is missed or vomiting occurs after taking a dose of ALECENSA, take the next dose at the scheduled time.
2.3 Dose Modifications for Adverse Reactions
The dose reduction schedule for ALECENSA is provided in Table 1.
| Dose reduction schedule | Dose level |
|---|---|
| Starting dose | 600 mg taken orally twice daily |
| First dose reduction | 450 mg taken orally twice daily |
| Second dose reduction | 300 mg taken orally twice daily |
Discontinue if patients are unable to tolerate the 300 mg twice daily dose.
Recommendations for dose modifications of ALECENSA in case of adverse reactions are provided in Table 2.
| Criteria* | ALECENSA Dose Modification |
|---|---|
|
|
| ALT or AST elevation of greater than 5 times upper limit of normal (ULN) with total bilirubin less than or equal to 2 times ULN | Temporarily withhold until recovery to baseline or to less than or equal to 3 times ULN, then resume at reduced dose as per Table 1. |
| ALT or AST elevation greater than 3 times ULN with total bilirubin elevation greater than 2 times ULN in the absence of cholestasis or hemolysis | Permanently discontinue ALECENSA. |
| Total bilirubin elevation of greater than 3 times ULN | Temporarily withhold until recovery to baseline or to less than or equal to 1.5 times ULN, then resume at reduced dose as per Table 1. |
| Any grade treatment-related interstitial lung disease (ILD)/pneumonitis | Permanently discontinue ALECENSA. |
| Grade 3 renal impairment | Temporarily withhold until serum creatinine recovers to less than or equal to 1.5 times ULN, then resume at reduced dose. |
| Grade 4 renal impairment | Permanently discontinue ALECENSA. |
| Symptomatic bradycardia | Withhold ALECENSA until recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above. If contributing concomitant medication is identified and discontinued, or its dose is adjusted, resume ALECENSA at previous dose upon recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above. If no contributing concomitant medication is identified, or if contributing concomitant medications are not discontinued or dose modified, resume ALECENSA at reduced dose (see Table 1) upon recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above. |
| Bradycardia† (life-threatening consequences, urgent intervention indicated) | Permanently discontinue ALECENSA if no contributing concomitant medication is identified. If contributing concomitant medication is identified and discontinued, or its dose is adjusted, resume ALECENSA at reduced dose (see Table 1) upon recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above, with frequent monitoring as clinically indicated. Permanently discontinue ALECENSA in case of recurrence. |
| CPK elevation greater than 5 times ULN | Temporarily withhold until recovery to baseline or to less than or equal to 2.5 times ULN, then resume at same dose. |
| CPK elevation greater than 10 times ULN or second occurrence of CPK elevation of greater than 5 times ULN | Temporarily withhold until recovery to baseline or to less than or equal to 2.5 times ULN, then resume at reduced dose as per Table 1. |
| Hemolytic Anemia | Withhold ALECENSA if hemolytic anemia is suspected. Upon resolution, resume at reduced dose or permanently discontinue. |
3. Dosage Forms and Strengths
150 mg hard capsules, white, with "ALE" printed in black ink on the cap and "150 mg" printed in black ink on the body.
5. Warnings and Precautions
5.1 Hepatotoxicity
Elevations of AST greater than 5 times the upper limit of normal (ULN) occurred in 4.6% of patients, and elevations of ALT greater than 5 times the ULN occurred in 5.3% of the 405 patients in Studies NP28761, NP28673 and ALEX who received ALECENSA at a dose of 600 mg BID. Elevations of bilirubin greater than 3 times the ULN occurred in 3.7% of patients. The majority (69% of the patients with hepatic transaminase elevations and 68% of the patients with bilirubin elevations) of these events occurred during the first 3 months of treatment. Six patients discontinued ALECENSA for Grades 3–4 AST and/or ALT elevations, and 4 patients discontinued ALECENSA for Grade 3 bilirubin elevations. Concurrent elevations in ALT or AST greater than or equal to 3 times the ULN and total bilirubin greater than or equal to 2 times the ULN, with normal alkaline phosphatase, occurred in less than 1% of patients treated with ALECENSA across clinical trials. Three patients with Grades 3–4 AST/ALT elevations had drug-induced liver injury (documented by liver biopsy in two cases).
Monitor liver function tests including ALT, AST, and total bilirubin every 2 weeks during the first 3 months of treatment, then once a month and as clinically indicated, with more frequent testing in patients who develop transaminase and bilirubin elevations. Based on the severity of the adverse drug reaction, withhold ALECENSA and resume at a reduced dose or permanently discontinue ALECENSA as described in Table 2 [see Dosage and Administration (2.3)].
5.2 Interstitial Lung Disease (ILD)/Pneumonitis
ILD/pneumonitis occurred in three (0.7%) patients treated with ALECENSA in Studies NP28761, NP28673 and ALEX. One (0.2%) of these events was severe (Grade 3).
Promptly investigate for ILD/pneumonitis in any patient who presents with worsening of respiratory symptoms indicative of ILD/pneumonitis (e.g., dyspnea, cough, and fever). Immediately withhold ALECENSA treatment in patients diagnosed with ILD/pneumonitis and permanently discontinue ALECENSA if no other potential causes of ILD/pneumonitis have been identified [see Dosage and Administration (2.3) and Adverse Reactions (6)].
5.3 Renal Impairment
Renal impairment occurred in 8% of patients in Studies NP28761, NP28673, and ALEX. The incidence of Grade ≥ 3 renal impairment was 1.7%, of which 0.5% were fatal events. Dose modifications for renal impairment were required in 3.2% of patients. Median time to Grade ≥ 3 renal impairment was 3.7 months (range 0.5 to 14.7 months).
Permanently discontinue ALECENSA for Grade 4 renal toxicity. Withhold ALECENSA for Grade 3 renal toxicity until recovery to less than or equal to 1.5 times ULN, then resume at reduced dose [see Dosage and Administration (2.3)].
5.4 Bradycardia
Symptomatic bradycardia can occur with ALECENSA. Cases of bradycardia (8.6%) have been reported in patients treated with ALECENSA in Studies NP28761, NP28673 and ALEX. Eighteen percent of 365 patients treated with ALECENSA for whom serial ECGs were available had heart rates of less than 50 beats per minute (bpm).
Monitor heart rate and blood pressure regularly. Dose modification is not required in cases of asymptomatic bradycardia. In cases of symptomatic bradycardia that is not life-threatening, withhold ALECENSA until recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above and evaluate concomitant medications known to cause bradycardia, as well as anti-hypertensive medications. If attributable to a concomitant medication, resume ALECENSA at a reduced dose (see Table 1) upon recovery to asymptomatic bradycardia or to a heart rate of 60 bpm or above, with frequent monitoring as clinically indicated. Permanently discontinue ALECENSA in case of recurrence. Permanently discontinue ALECENSA in cases of life-threatening bradycardia if no contributing concomitant medication is identified [see Dosage and Administration (2.3)].
5.5 Severe Myalgia and Creatine Phosphokinase (CPK) Elevation
Myalgia or musculoskeletal pain occurred in 26% of patients in Studies NP28761, NP28673 and ALEX. The incidence of Grade 3 myalgia/musculoskeletal pain was 0.7%. Dose modifications for myalgia/musculoskeletal pain were required in 0.5% of patients.
Elevations of CPK occurred in 41% of 347 patients with CPK laboratory data available in Studies NP28761, NP28673 and ALEX. The incidence of Grade 3 elevations of CPK was 4.0%. Median time to Grade 3 CPK elevation was 14 days (interquartile range 13-28 days). Dose modifications for elevation of CPK occurred in 3.2 % of patients.
Advise patients to report any unexplained muscle pain, tenderness, or weakness. Assess CPK levels every 2 weeks for the first month of treatment and as clinically indicated in patients reporting symptoms. Based on the severity of the CPK elevation, withhold ALECENSA, then resume or reduce dose [see Dosage and Administration (2.3)].
5.6 Hemolytic Anemia
Hemolytic anemia has been reported with ALECENSA, including cases associated with a negative direct antiglobulin test (DAT) result. If hemolytic anemia is suspected, withhold ALECENSA and initiate appropriate laboratory testing. If hemolytic anemia is confirmed, consider resuming at a reduced dose upon resolution or permanently discontinue ALECENSA [see Dosage and Administration (2.3)].
5.7 Embryo-Fetal Toxicity
Based on findings from animal studies and its mechanism of action, ALECENSA can cause fetal harm when administered to pregnant women. Administration of alectinib to pregnant rats and rabbits during the period of organogenesis resulted in embryo-fetal toxicity and abortion at maternally toxic doses with exposures approximately 2.7 times those observed in humans with alectinib 600 mg twice daily. Advise pregnant women of the potential risk to a fetus.
Advise females of reproductive potential to use effective contraception during treatment with ALECENSA and for 1 week following the final dose [see Use in Specific Populations (8.1 and 8.3) and Clinical Pharmacology (12.1)].
6. Adverse Reactions/Side Effects
The following adverse reactions are discussed in greater detail in other sections of the label:
- Hepatotoxicity [see Warnings and Precautions (5.1)]
- Interstitial Lung Disease (ILD)/Pneumonitis [see Warnings and Precautions (5.2)]
- Renal Impairment [see Warnings and Precautions (5.3)]
- Bradycardia [see Warnings and Precautions (5.4)]
- Severe Myalgia and Creatine Phosphokinase (CPK) Elevation [see Warnings and Precautions (5.5)]
- Hemolytic Anemia [see Warnings and Precautions (5.6)]
- Embryo-Fetal Toxicity [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Previously Untreated ALK-Positive Metastatic NSCLC
The safety of ALECENSA was evaluated in 152 patients with ALK-positive NSCLC in the ALEX study. The median duration of exposure to ALECENSA was 17.9 months. Patient characteristics of the ALEX study population (n=303) were: median age 56 years, age less than 65 (77%), female (56%), Caucasian (50%), Asian (46%), adenocarcinoma histology (92%), never smoker (63%), and ECOG PS 0 or 1 (93%).
Serious adverse reactions occurred in 28% of patients treated with ALECENSA; serious adverse reactions reported in 2% or more of patients treated with ALECENSA were pneumonia (4.6%), and renal impairment (3.9%). Grade ≥ 3 adverse events were reported for 41% of patients in the ALECENSA arm. Fatal adverse reactions occurred in 3.3% of patients treated with ALECENSA; these were renal impairment (2 patients), sudden death, cardiac arrest, and pneumonia (1 patient each). Permanent discontinuation of ALECENSA for adverse reactions occurred in 11% of patients. Adverse drug reactions that led to discontinuation of ALECENSA in 1% or more of patients were renal impairment (2.0%), hyperbilirubinemia (1.3%), increased ALT (1.3%), and increased AST (1.3%). Dose reductions and drug interruption due to adverse reactions occurred in 16% and 19% of patients, respectively, in the ALECENSA arm. The most frequent adverse reactions that led to dose modifications in the ALECENSA arm were hyperbilirubinemia (6%), increased AST (5%), increased ALT (4.6%), and pneumonia (3.3%).
Tables 3 and 4 summarize the common adverse reactions and laboratory abnormalities observed in ALEX.
| Adverse Reaction | ALECENSA N = 152 | Crizotinib N= 151 |
||
|---|---|---|---|---|
| All Grades (%) | Grades 3-4 (%) | All Grades (%) | Grades 3-4 (%) | |
| NCI CTCAE= National Cancer Institute Common Terminology Criteria for Adverse Events; MedDRA = Medical Dictionary for Regulatory Activities; SOC = System Organ Class. | ||||
|
||||
| Gastrointestinal | ||||
| Constipation | 34 | 0 | 33 | 0 |
| Nausea | 14 | 0.7 | 48 | 3.3 |
| Diarrhea | 12 | 0 | 45 | 2.0 |
| Vomiting | 7 | 0 | 38 | 3.3 |
| General | ||||
| Fatigue* | 26 | 1.3 | 23 | 0.7 |
| Edema† | 22 | 0.7 | 34 | 0.7 |
| Musculoskeletal | ||||
| Myalgia‡ | 23 | 0 | 4.0 | 0 |
| Skin | ||||
| Rash§ | 15 | 0.7 | 13 | 0 |
| Nervous system | ||||
| Dysgeusia¶ | 3.3 | 0.7 | 19 | 0 |
| Eye | ||||
| Vision disorders# | 4.6 | 0 | 23 | 0 |
| Cardiac | ||||
| BradycardiaÞ | 11 | 0 | 15 | 0 |
| Renal | ||||
| Renal impairmentß | 12 | 3.9à | 0 | 0 |
The following additional clinically significant adverse drug reactions were observed in patients treated with ALECENSA: weight gain (9.9%), photosensitivity reaction (5.3%), stomatitis (3.3%), interstitial lung disease (1.3%), and drug-induced liver injury (1.3%).
| Parameter | ALECENSA N= 152 | Crizotinib N=151 |
||
|---|---|---|---|---|
| All Grades (%) | Grades 3–4 (%) | All Grades (%) | Grades 3–4 (%) | |
| Note: Based on National Cancer Institute Common Terminology Criteria for Adverse Events v4.03. Excludes patients with no post-baseline lab assessments. |
||||
|
||||
| Chemistry | ||||
| Hyperbilirubinemia* | 54 | 5 | 4.7 | 0 |
| Increased AST† | 50 | 6 | 56 | 11 |
| Increased alkaline phosphatase‡ | 50 | 0 | 44 | 0 |
| Increased ALT‡ | 40 | 6 | 62 | 16 |
| Increased creatinine‡,§ | 38 | 4.1 | 23 | 0.7 |
| Increased CPK¶ | 37 | 2.8 | 52 | 1.4 |
| Hypocalcemia* | 29 | 0 | 61 | 1.4 |
| Hyperglycemia# | 22 | 2.2 | 19 | 2.3 |
| HyponatremiaÞ | 18 | 6 | 20 | 4.1 |
| Hypokalemia‡ | 17 | 2 | 12 | 0.7 |
| Hypoalbuminemiaß | 14 | 0 | 57 | 3.4 |
| Hyperkalemia‡ | 12 | 1.4 | 16 | 1.4 |
| Hypophosphatemiaà | 9 | 1.4 | 25 | 2.7 |
| Increased gamma glutamyl transferaseè | 7 | 0.7 | 39 | 4.1 |
| Hematology | ||||
| Anemia‡ | 62 | 7 | 36 | 0.7 |
| Lymphopenia* | 14 | 1.4 | 34 | 4.1 |
| Neutropenia‡ | 14 | 0 | 36 | 7 |
ALK-Positive Metastatic NSCLC Previously Treated with Crizotinib
The safety of ALECENSA was evaluated in 253 patients with ALK-positive non-small cell lung cancer (NSCLC) treated with ALECENSA in two clinical trials, Studies NP28761 and NP28673. The median duration of exposure to ALECENSA was 9.3 months. One hundred sixty-nine patients (67%) were exposed to ALECENSA for more than 6 months, and 100 patients (40%) for more than one year. The population characteristics were: median age 53 years, age less than 65 (86%), female (55%), White (74%), Asian (18%), NSCLC adenocarcinoma histology (96%), never or former smoker (98%), ECOG Performance Status (PS) 0 or 1 (91%), and prior chemotherapy treatment (78%).
Serious adverse reactions occurred in 19% of patients; the most frequently reported serious adverse reactions were pulmonary embolism (1.2%), dyspnea (1.2%), and hyperbilirubinemia (1.2%). Fatal adverse reactions occurred in 2.8% of patients and included hemorrhage (0.8%), intestinal perforation (0.4%), dyspnea (0.4%), pulmonary embolism (0.4%), and endocarditis (0.4%). Permanent discontinuation of ALECENSA for adverse reactions occurred in 6% of patients. The most frequent adverse reactions that led to permanent discontinuation were hyperbilirubinemia (1.6%), increased ALT levels (1.6%), and increased AST levels (1.2%). Overall, 23% of patients initiating treatment at the recommended dose required at least one dose reduction. The median time to first dose reduction was 48 days. The most frequent adverse reactions that led to dose reductions or interruptions were elevations in bilirubin (6%), CPK (4.3%), ALT (4.0%), AST (2.8%), and vomiting (2.8%).
Tables 5 and 6 summarize the common adverse reactions and laboratory abnormalities observed in Studies NP28761 and NP28673.
| Adverse Reactions | ALECENSA N=253 |
|
|---|---|---|
| All Grades (%) | Grades 3–4 (%)* | |
|
||
| Fatigue† | 41 | 1.2 |
| Constipation | 34 | 0 |
| Edema‡ | 30 | 0.8 |
| Myalgia§ | 29 | 1.2 |
| Cough | 19 | 0 |
| Rash¶ | 18 | 0.4 |
| Nausea | 18 | 0 |
| Headache | 17 | 0.8 |
| Diarrhea | 16 | 1.2 |
| Dyspnea | 16 | 3.6# |
| Back pain | 12 | 0 |
| Vomiting | 12 | 0.4 |
| Increased weight | 11 | 0.4 |
| Vision disorderÞ | 10 | 0 |
An additional clinically significant adverse drug reaction was photosensitivity, which occurred in 9.9% of patients exposed to ALECENSA in Studies NP28761 and NP28673. Patients were advised to avoid sun exposure and to use broad-spectrum sunscreen. The incidence of Grade 2 photosensitivity was 0.4%; the remaining events were Grade 1 in severity.
| Parameter | ALECENSA N=250 | |
|---|---|---|
| All Grades (%) | Grades 3–4 (%)* | |
|
||
| Chemistry | ||
| Increased AST | 51 | 3.6 |
| Increased Alkaline Phosphatase | 47 | 1.2 |
| Increased CPK† | 43 | 4.6 |
| Hyperbilirubinemia | 39 | 2.4 |
| Hyperglycemia‡ | 36 | 2.0 |
| Increased ALT | 34 | 4.8 |
| Hypocalcemia | 32 | 0.4 |
| Hypokalemia | 29 | 4.0 |
| Increased Creatinine§ | 28 | 0 |
| Hypophosphatemia | 21 | 2.8 |
| Hyponatremia | 20 | 2.0 |
| Hematology | ||
| Anemia | 56 | 2.0 |
| Lymphopenia¶ | 22 | 4.6 |
6.2 Postmarketing Experience
The following adverse reactions have been identified during postapproval use of ALECENSA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8. Use In Specific Populations
8.4 Pediatric Use
The safety and effectiveness of ALECENSA in pediatric patients have not been established.
8.5 Geriatric Use
Clinical studies of ALECENSA did not include sufficient number of subjects aged 65 and older to determine whether they respond differently from younger subjects.
8.6 Renal Impairment
No dose adjustment is recommended for patients with mild or moderate renal impairment. The safety of ALECENSA in patients with severe renal impairment (creatinine clearance less than 30 mL/min) or end-stage renal disease has not been studied [see Clinical Pharmacology (12.3)].
8.7 Hepatic Impairment
No dose adjustment is recommended for patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment. Increased exposure of alectinib occurred in patients with severe hepatic impairment (Child-Pugh C). The recommended dose of ALECENSA in patients with severe hepatic impairment (Child-Pugh C) is 450 mg orally twice daily [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)].
10. Overdosage
No experience with overdose is available. There is no specific antidote for overdose with ALECENSA. Alectinib and its major active metabolite M4 are > 99% bound to plasma proteins; therefore, hemodialysis is likely to be ineffective in the treatment of overdose.
11. Alecensa Description
ALECENSA (alectinib) is a kinase inhibitor for oral administration. The molecular formula for alectinib is C30H34N4O2 ∙ HCl. The molecular weight is 482.62 g/mol (free base form) and 519.08 g/mol (hydrochloride salt). Alectinib is described chemically as 9-ethyl-6, 6-dimethyl-8-[4-(morpholin-4-yl)piperidin-1-yl]-11-oxo-6, 11-dihydro-5H-benzo[b]carbazole-3-carbonitrile hydrochloride. The chemical structure of alectinib is shown below:
Alectinib HCl is a white to yellow white powder or powder with lumps with a pKa of 7.05 (base).
ALECENSA is supplied as hard capsules containing 150 mg of alectinib (equivalent to 161.33 mg alectinib HCl) and the following inactive ingredients: lactose monohydrate, hydroxypropylcellulose, sodium lauryl sulfate, magnesium stearate, and carboxymethylcellulose calcium. The capsule shell contains hypromellose, carrageenan, potassium chloride, titanium dioxide, corn starch, and carnauba wax. The printing ink contains red iron oxide (E172), yellow iron oxide (E172), FD&C Blue No. 2 aluminum lake (E132), carnauba wax, white shellac, and glyceryl monooleate.
12. Alecensa - Clinical Pharmacology
12.1 Mechanism of Action
Alectinib is a tyrosine kinase inhibitor that targets ALK and RET. In nonclinical studies, alectinib inhibited ALK phosphorylation and ALK-mediated activation of the downstream signaling proteins STAT3 and AKT, and decreased tumor cell viability in multiple cell lines harboring ALK fusions, amplifications, or activating mutations. The major active metabolite of alectinib, M4, showed similar in vitro potency and activity.
Alectinib and M4 demonstrated in vitro and in vivo activity against multiple mutant forms of the ALK enzyme, including some mutations identified in NSCLC tumors in patients who have progressed on crizotinib.
In mouse models implanted with tumors carrying ALK fusions, administration of alectinib resulted in antitumor activity and prolonged survival, including in mouse models implanted intracranially with ALK-driven tumor cell lines.
12.3 Pharmacokinetics
The pharmacokinetics of alectinib and its major active metabolite M4 have been characterized in patients with ALK-positive NSCLC and healthy subjects.
In patients with ALK-positive NSCLC, the geometric mean (coefficient of variation %) steady-state maximal concentration (Cmax,ss) for alectinib was 665 ng/mL (44%) and for M4 was 246 ng/mL (45%) with peak to trough concentration ratio of 1.2. The geometric mean steady-state area under the curve from 0 to 12 hours (AUC0-12h,ss) for alectinib was 7,430 ng*h/mL (46%) and for M4 was 2,810 ng*h/mL (46%). Alectinib exposure is dose proportional across the dose range of 460 mg to 900 mg (i.e., 0.75 to 1.5 times the approved recommended dosage) under fed conditions. Alectinib and M4 reached steady-state concentrations by day 7. The geometric mean accumulation was approximately 6-fold for both alectinib and M4.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenicity studies with alectinib have not been conducted.
Alectinib was not mutagenic in vitro in the bacterial reverse mutation (Ames) assay, but was positive with an increased number of micronuclei in a rat bone marrow micronucleus test. The mechanism of micronucleus induction was abnormal chromosome segregation (aneugenicity) and not a clastogenic effect on chromosomes.
No studies in animals have been performed to evaluate the effect of alectinib on fertility. No adverse effects on male and female reproductive organs were observed in general toxicology studies conducted in rats and monkeys.
14. Clinical Studies
Previously Untreated ALK-Positive Metastatic NSCLC
The efficacy of ALECENSA for the treatment of patients with ALK-positive NSCLC who had not received prior systemic therapy for metastatic disease was established in an open-label, randomized, active-controlled, multicenter study (ALEX: NCT02075840). Patients were required to have an ECOG performance status of 0-2 and ALK-positive NSCLC as identified by the VENTANA ALK (D5F3) CDx assay. Neurologically stable patients with treated or untreated central nervous system (CNS) metastases, including leptomeningeal metastases, were eligible; patients with neurologic signs and symptoms due to CNS metastases were required to have completed whole brain radiation or gamma knife irradiation at least 14 days prior to enrollment and be clinically stable. Patients with a baseline QTc > 470 ms were ineligible.
Patients were randomized 1:1 to receive ALECENSA 600 mg orally twice daily or crizotinib 250 mg orally twice daily. Randomization was stratified by ECOG performance status (0/1 vs. 2), race (Asian vs. non-Asian), and the presence or absence of CNS metastases at baseline. Treatment on both arms was continued until disease progression or unacceptable toxicity. The major efficacy outcome measure was progression-free survival (PFS) as determined by investigator assessment according to RECIST v1.1. Additional efficacy outcome measures were PFS as determined by independent review committee (IRC), time to CNS progression by IRC based on RECIST v1.1, objective response rate (ORR) and duration of response (DOR), and overall survival (OS). Additional exploratory outcome measures were CNS objective response rate (CNS-ORR) and CNS duration of response (CNS-DOR) by IRC in patients with CNS metastases at baseline.
A total of 303 patients were randomized to ALECENSA (n=152) or crizotinib (n=151). The demographic characteristics of the study population were 56% female, median age 56 years (range: 18 to 91 years), 50% White, 46% Asian, 1% Black, and 3% other races. The majority of patients had adenocarcinoma (92%) and never smoked (63%). CNS metastases were present in 40% (n=122) of patients: of these, 43 patients had measurable CNS lesions as determined by an IRC. The ALEX study demonstrated a significant improvement in PFS. The time to cause-specific CNS progression as assessed by IRC was also significantly improved; there was a lower incidence of progression in the CNS as the first site of disease progression, alone or with concurrent systemic progression, in the ALECENSA arm (12%) as compared to the crizotinib arm (45%). Efficacy results from ALEX are summarized in Table 7 and Figure 1.
| ALECENSA N=152 | Crizotinib N=151 |
|
|---|---|---|
| CNS: central nervous system, ORR: overall response rate, IRC: independent review committee, CI: confidence interval, NE: not estimable. | ||
|
||
| Progression-Free Survival | ||
| Number of events (%) | 63 (41%) | 92 (61%) |
| Progressive disease (%) | 51 (34%) | 82 (54%) |
| Death (%) | 12 (8%) | 10 (7%) |
| Median in months (95% CI) | 25.7 (19.9, NE) | 10.4 (7.7, 14.6) |
| Hazard ratio (95% CI) * | 0.53 (0.38, 0.73) | |
| P-value * | < 0.0001 | |
| Overall Response Rate | ||
| Overall response rate, % (95% CI) † | 79% (72, 85) | 72% (64, 79) |
| P-value * | 0.1652 | |
| Complete response, % | 13% | 6% |
| Partial response, % | 66% | 66% |
| Duration of Response | ||
| Number of responders | n=120 | n=109 |
| Response duration ≥6 months | 82% | 57% |
| Response duration ≥12 months | 64% | 36% |
| Response duration ≥18 months | 37% | 14% |
Figure 1: Kaplan-Meier Plot of Progression-Free Survival (IRC) in ALEX
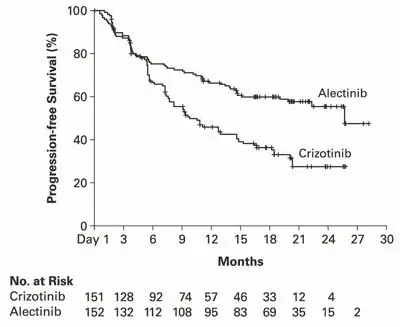
Results for PFS as determined by investigator assessment (HR=0.48 [95% CI: 0.35-0.66], stratified log-rank p<0.0001) were similar to that observed by IRC. At the data cutoff point overall survival data was not mature.
The results of prespecified exploratory analyses of CNS response rate in patients with measurable CNS lesions at baseline are summarized in Table 8.
| ALECENSA | Crizotinib | |
|---|---|---|
| IRC: Independent Review Committee; CI: Confidence Interval; NE: Not Estimable | ||
|
||
| CNS Tumor Response Assessment | N = 21 | N = 22 |
| CNS Objective Response Rate, % (95% CI*) | 81% (58, 95) | 50% (28,72) |
| Complete Response | 38% | 5% |
| Duration of CNS Response | ||
| Number of responders | 17 | 11 |
| CNS response duration ≥ 12 months | 59% | 36% |
ALK-Positive Metastatic NSCLC Previously Treated with Crizotinib
The safety and efficacy of ALECENSA were established in two single-arm, multicenter clinical trials: NP28761 (NCT01588028) and NP28673 (NCT01801111). Patients with locally advanced or metastatic ALK-positive NSCLC, who have progressed on crizotinib, with documented ALK-positive NSCLC based on an FDA-approved test, and ECOG PS of 0-2 were enrolled in both studies. Eligibility criteria permitted enrollment of patients with prior chemotherapy and prior CNS radiotherapy provided that CNS metastases were stable for at least two weeks. All patients received ALECENSA 600 mg orally twice daily. The major efficacy outcome measure in both studies was objective response rate (ORR) according to Response Evaluation Criteria in Solid Tumors (RECIST v1.1) as evaluated per Independent Review Committee (IRC). Additional outcome measures as evaluated by the IRC included duration of response (DOR), CNS ORR, and CNS DOR.
NP28761 was conducted in North America and enrolled 87 patients. Baseline demographic and disease characteristics in NP28761 were median age 54 years old (range 29 to 79, 18% 65 and over), 84% White and 8% Asian, 55% female, 35% ECOG PS 0 and 55% ECOG PS 1, 100% never or former smokers, 99% Stage IV, 94% adenocarcinoma, and 74% prior chemotherapy. The most common sites of extra-thoracic metastasis included 60% CNS (of whom 65% had received CNS radiation), 43% lymph nodes, 36% bone, and 34% liver.
NP28673 was conducted internationally and enrolled 138 patients. Baseline demographic and disease characteristics in NP28673 were median age 52 years old (range 22 to 79, 10% 65 and over), 67% White and 26% Asian, 56% female, 32% ECOG PS 0 and 59% ECOG PS 1, 98% never or former smokers, 99% Stage IV, 96% adenocarcinoma, and 80% prior chemotherapy. The most common sites of extra-thoracic metastasis included 61% CNS (of whom 73% had received CNS radiation), 51% bone, 38% lymph nodes, and 30% liver.
Efficacy results from NP28761 and NP28673 in all treated patients are summarized in Table 9. The median duration of follow-up on Study NP28761 was 4.8 months for both IRC and Investigator assessments and on Study NP28673, 10.9 months for IRC assessment and 7.0 months for Investigator assessment. All responses were partial responses.
| Efficacy Parameter | NP28761 (N=87) | NP28673 (N=138) | ||
|---|---|---|---|---|
| IRC* Assessment | Investigator Assessment | IRC* Assessment | Investigator Assessment | |
|
||||
| Objective Response Rate (95% CI) | 38% (28; 49) | 46% (35; 57) | 44% (36; 53) | 48% (39; 57) |
| Number of Responders | 33 | 40 | 61 | 66 |
| Duration of Response, median in months (95% CI) | 7.5 (4.9, Not Estimable) | NE (4.9, Not Estimable) | 11.2 (9.6, Not Estimable) | 7.8 (7.4, 9.2) |
An assessment of ORR and duration of response for CNS metastases in the subgroup of 51 patients in NP28761 and NP28673 with baseline measurable lesions in the CNS according to RECIST v1.1 are summarized in Table 10. Thirty-five (69%) patients with measurable CNS lesions had received prior brain radiation, including 25 (49%) who completed radiation treatment at least 6 months before starting treatment with ALECENSA. Responses were observed irrespective of prior brain radiation status.
| Efficacy Parameter | N=51 |
|---|---|
| CNS Objective Response Rate (95% CI) | 61% (46, 74) |
| Complete Response | 18% |
| Partial Response | 43% |
| CNS Duration of Response, median in months (95% CI) | 9.1 (5.8, Not Estimable) |
16. How is Alecensa supplied
Hard capsules, white 150 mg capsules with "ALE" printed in black ink on the cap and "150 mg" printed in black ink on the body, available in:
| 240 capsules per bottle: | NDC 50242-130-01 |
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
Inform patients of the following:
| This Patient Information has been approved by the U.S. Food and Drug Administration. | Revised: 09/2021 | ||
| PATIENT INFORMATION
ALECENSA® (a-le-sen-sah) (alectinib) capsules |
|||
| What is the most important information I should know about ALECENSA? ALECENSA may cause serious side effects, including:
|
|||
|
|
||
|
|||
| What is ALECENSA?
ALECENSA is a prescription medicine used to treat people with non-small cell lung cancer (NSCLC):
|
|||
Before you take ALECENSA, tell your healthcare provider about all of your medical conditions, including if you:
|
|||
How should I take ALECENSA?
|
|||
What should I avoid while taking ALECENSA?
|
|||
| What are the possible side effects of ALECENSA? ALECENSA may cause serious side effects, including:
|
|||
|
|
||
| These are not all of the possible side effects of ALECENSA. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. |
|||
How should I store ALECENSA?
|
|||
| General information about the safe and effective use of ALECENSA.
Medicines are sometimes prescribed for purposes other than those listed in a Patient Information leaflet. Do not use ALECENSA for a condition for which it was not prescribed. Do not give ALECENSA to other people, even if they have the same symptoms that you have. It may harm them. You can ask your healthcare provider or pharmacist for information about ALECENSA that is written for health professionals. |
|||
| What are the ingredients in ALECENSA?
Active ingredient: alectinib Inactive ingredients: lactose monohydrate, hydroxypropylcellulose, sodium lauryl sulfate, magnesium stearate and carboxymethylcellulose calcium. Capsule shell contains: hypromellose, carrageenan, potassium chloride, titanium dioxide, corn starch, and carnauba wax. Printing ink contains: red iron oxide (E172), yellow iron oxide (E172), FD&C Blue No. 2 aluminum lake (E132), carnauba wax, white shellac, and glyceryl monooleate. Distributed by: Genentech, Inc., A Member of the Roche Group, 1 DNA Way, South San Francisco, CA 94080-4990 ALECENSA® is a registered trademark of Chugai Pharmaceutical Co., Ltd., Tokyo, Japan ©2021 Genentech, Inc. For more information, go to www.ALECENSA.com or call 1-800-253-2367. |
|||
| ALECENSA
alectinib hydrochloride capsule |
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||
| Labeler - Genentech, Inc. (080129000) |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| F. Hoffmann-La Roche Ltd | 485244961 | ANALYSIS(50242-130) , LABEL(50242-130) , PACK(50242-130) | |
| Establishment | |||
| Name | Address | ID/FEI | Business Operations |
|---|---|---|---|
| F. Hoffmann-La Roche AG | 482242971 | ANALYSIS(50242-130) | |
