Drug Detail:Nexplanon (Etonogestrel (implant) [ e-toe-noe-jes-trel ])
Drug Class: Contraceptives Progestins
Highlights of Prescribing Information
NEXPLANON® (etonogestrel implant)
Radiopaque
Subdermal Use Only
Initial U.S. Approval: 2001
Recent Major Changes
| Warnings and Precautions, Complications of Insertion and Removal (5.1) | 9/2020 |
| Warnings and Precautions, Broken or Bent Implant (5.16) | 10/2020 |
Indications and Usage for Nexplanon
NEXPLANON is a progestin indicated for use by women to prevent pregnancy. (1)
Nexplanon Dosage and Administration
Insert one NEXPLANON subdermally just under the skin at the inner side of the non-dominant upper arm. NEXPLANON must be removed no later than by the end of the third year. (2)
Dosage Forms and Strengths
NEXPLANON consists of a single, radiopaque, rod-shaped implant, containing 68 mg etonogestrel, pre-loaded in the needle of a disposable applicator. (3)
Contraindications
- Known or suspected pregnancy. (4)
- Current or past history of thrombosis or thromboembolic disorders. (4, 5.4)
- Liver tumors, benign or malignant, or active liver disease. (4, 5.7)
- Undiagnosed abnormal genital bleeding. (4, 5.2)
- Known or suspected breast cancer, personal history of breast cancer, or other progestin-sensitive cancer, now or in the past. (4, 5.6)
- Allergic reaction to any of the components of NEXPLANON. (4, 6)
Warnings and Precautions
- Insertion and removal complications: Pain, paresthesias, bleeding, hematoma, scarring, infection, or migration to vasculature, including pulmonary vessels, may occur. Symptoms associated with implants in pulmonary vessels include chest pain, dyspnea, cough, or hemoptysis. Surgical interventions may be necessary to remove implants. (5.1)
- Menstrual bleeding pattern: Counsel women regarding changes in bleeding frequency, intensity, or duration. (5.2)
- Ectopic pregnancies: Be alert to the possibility of an ectopic pregnancy in women using NEXPLANON who become pregnant or complain of lower abdominal pain. (5.3)
- Thrombotic and other vascular events: The NEXPLANON implant should be removed in the event of a thrombosis. (5.4)
- Liver disease: Remove the NEXPLANON implant if jaundice occurs. (5.7)
- Elevated blood pressure: The NEXPLANON implant should be removed if blood pressure rises significantly and becomes uncontrolled. (5.9)
- Carbohydrate and lipid metabolic effects: Monitor prediabetic and diabetic women using NEXPLANON. (5.11)
Adverse Reactions/Side Effects
Most common (≥10%) adverse reactions reported in clinical trials were change in menstrual bleeding pattern, headache, vaginitis, weight increase, acne, breast pain, abdominal pain, and pharyngitis. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Organon USA LLC, a subsidiary of Organon & Co., at 1-844-674-3200 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Interactions
Drugs or herbal products that induce certain enzymes, such as CYP3A4, may decrease the effectiveness of progestin hormonal contraceptives or increase breakthrough bleeding. (7.1)
Use In Specific Populations
- Pregnancy: Discontinue if maintaining a pregnancy. (8.1)
- Overweight women: NEXPLANON may become less effective in overweight women over time, especially in the presence of other factors that decrease etonogestrel concentrations, such as concomitant use of hepatic enzyme inducers. (8.7)
See 17 for PATIENT COUNSELING INFORMATION and FDA-approved patient labeling.
Revised: 7/2021
Full Prescribing Information
1. Indications and Usage for Nexplanon
NEXPLANON® is indicated for use by women to prevent pregnancy.
2. Nexplanon Dosage and Administration
The efficacy of NEXPLANON does not depend on daily, weekly or monthly administration.
All healthcare professionals should receive instruction and training prior to performing insertion and/or removal of NEXPLANON.
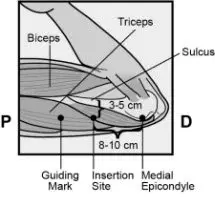
A single NEXPLANON implant is inserted subdermally just under the skin at the inner side of the non-dominant upper arm. The insertion site is overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles. This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus (see Figures 2a, 2b and 2c). An implant inserted more deeply than subdermally (deep insertion) may not be palpable and the localization and/or removal can be difficult or impossible [see Dosage and Administration (2.3) and Warnings and Precautions (5.1)].
NEXPLANON must be inserted by the expiration date stated on the packaging. NEXPLANON is a long-acting (up to 3 years), reversible, hormonal contraceptive method. The implant must be removed by the end of the third year and may be replaced by a new implant at the time of removal, if continued contraceptive protection is desired.
2.1 Initiating Contraception with NEXPLANON
IMPORTANT: Rule out pregnancy before inserting the implant.
Timing of insertion depends on the woman's recent contraceptive history, as follows:
2.2 Insertion of NEXPLANON
The basis for successful use and subsequent removal of NEXPLANON is a correct and carefully performed subdermal insertion of the single, rod-shaped implant in accordance with the instructions. Both the healthcare professional and the woman should be able to feel the implant under the skin after placement.
All healthcare professionals performing insertions and/or removals of NEXPLANON should receive instructions and training prior to inserting or removing the implant.
Insertion Procedure
To help make sure the implant is inserted just under the skin, the healthcare professionals should be positioned to see the advancement of the needle by viewing the applicator from the side and not from above the arm. From the side view, the insertion site and the movement of the needle just under the skin can be clearly visualized.
For illustrative purposes, Figures depict the left inner arm.
Step 1. Have the woman lie on her back on the examination table with her non-dominant arm flexed at the elbow and externally rotated so that her hand is underneath her head (or as close as possible) (Figure 1).
 |
| Figure 1 |
 Step 2. Identify the insertion site, which is at the inner side of the non-dominant upper arm. The insertion site is overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles (Figures 2a, 2b and 2c). This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus. If it is not possible to insert the implant in this location (e.g., in women with thin arms), it should be inserted as far posterior from the sulcus as possible. [See Warnings and Precautions (5.1).]
Step 2. Identify the insertion site, which is at the inner side of the non-dominant upper arm. The insertion site is overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles (Figures 2a, 2b and 2c). This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus. If it is not possible to insert the implant in this location (e.g., in women with thin arms), it should be inserted as far posterior from the sulcus as possible. [See Warnings and Precautions (5.1).]
Step 3. Make two marks with a surgical marker: first, mark the spot where the etonogestrel implant will be inserted, and second, mark a spot at 5 centimeters (2 inches) proximal (toward the shoulder) to the first mark (Figure 2a and 2b). This second mark (guiding mark) will later serve as a direction guide during insertion.
 |
| Figure 2a P - Proximal (toward the shoulder) D - Distal (toward the elbow) |
 | 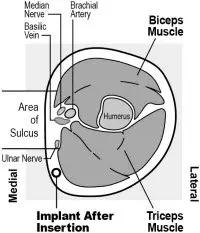 | ||
| Figure 2b | Figure 2c: Cross section of the upper left arm, as viewed from the elbow Medial (inner side of the arm) Lateral (outer side of the arm) |
Step 4. After marking the arm, confirm the site is in the correct location on the inner side of the arm.
Step 5. Clean the skin from the insertion site to the guiding mark with an antiseptic solution.
Step 6. Anesthetize the insertion area (for example, with anesthetic spray or by injecting 2 mL of 1% lidocaine just under the skin along the planned insertion tunnel).
Step 7. Remove the sterile preloaded disposable NEXPLANON applicator carrying the implant from its blister. The applicator should not be used if sterility is in question.
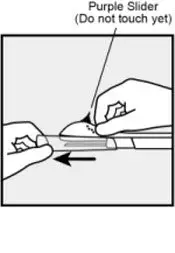
Step 8. Hold the applicator just above the needle at the textured surface area. Remove the transparent protection cap by sliding it horizontally in the direction of the arrow away from the needle (Figure 3). If the cap does not come off easily, the applicator should not be used. You should see the white colored implant by looking into the tip of the needle. Do not touch the purple slider until you have fully inserted the needle subdermally, as doing so will retract the needle and prematurely release the implant from the applicator.
Step 9. If the purple slider is released prematurely, restart the procedure with a new applicator.
 |
| Figure 3 |
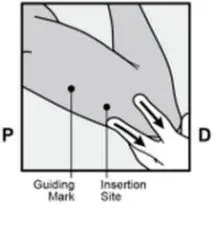
Step 10. With your free hand, stretch the skin around the insertion site towards the elbow (Figure 4).
 |
| Figure 4 |
Step 11. The implant should be inserted subdermally just under the skin [see Warnings and Precautions (5.1)].
To help make sure the implant is inserted just under the skin, you should position yourself to see the advancement of the needle by viewing the applicator from the side and not from above the arm. From the side view (see Figure 6), you can clearly see the insertion site and the movement of the needle just under the skin.
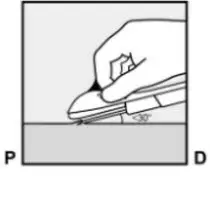
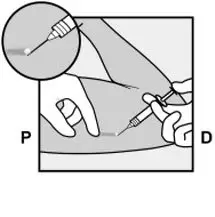
Step 12. Puncture the skin with the tip of the needle slightly angled less than 30° (Figure 5a).
 |
| Figure 5a |
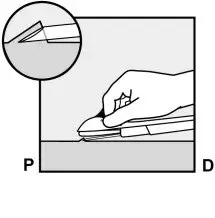
 Step 13. Insert the needle until the bevel (slanted opening of the tip) is just under the skin (and no further) (Figure 5b). If you inserted the needle deeper than the bevel, withdraw the needle until only the bevel is beneath the skin.
Step 13. Insert the needle until the bevel (slanted opening of the tip) is just under the skin (and no further) (Figure 5b). If you inserted the needle deeper than the bevel, withdraw the needle until only the bevel is beneath the skin.
 |
| Figure 5b |
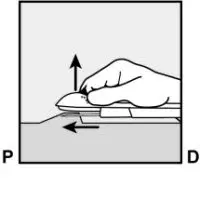
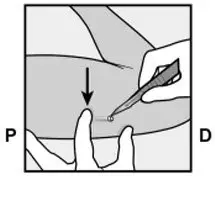
Step 14. Lower the applicator to a nearly horizontal position. To facilitate subdermal placement, lift the skin with the needle while sliding the needle to its full length (Figure 6). You may feel slight resistance but do not exert excessive force. If the needle is not inserted to its full length, the implant will not be inserted properly.
If the needle tip emerges from the skin before needle insertion is complete, the needle should be pulled back and be readjusted to subdermal position before completing the insertion procedure.
 |
| Figure 6 |
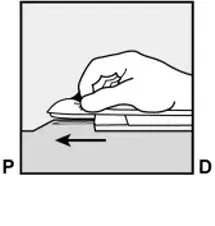
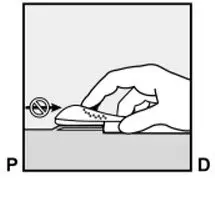
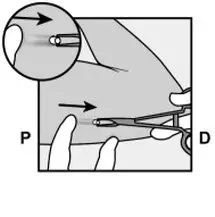
Step 15. Keep the applicator in the same position with the needle inserted to its full length (Figure 7). If needed, you may use your free hand to stabilize the applicator. Unlock the purple slider by pushing it slightly down (Figure 8a). Move the slider fully back until it stops. Do not move the applicator while moving the purple slider (Figure 8b). The implant is now in its final subdermal position, and the needle is locked inside the body of the applicator. The applicator can now be removed (Figure 8c).
 |
| Figure 7 |
 | 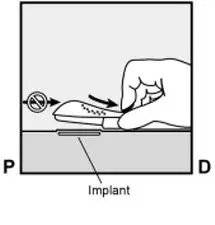 | ||
| Figure 8a | Figure 8b |
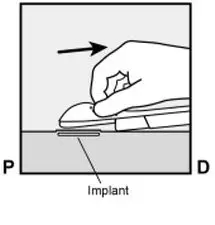 |
| Figure 8c |
If the applicator is not kept in the same position during this procedure or if the purple slider is not moved fully back until it stops, the implant will not be inserted properly and may protrude from the insertion site.
If the implant is protruding from the insertion site, remove the implant and perform a new procedure at the same insertion site using a new applicator. Do not push the protruding implant back into the incision.
Step 16. Apply a small adhesive bandage over the insertion site.
Step 17. Always verify the presence of the implant in the woman's arm immediately after insertion by palpation. By palpating both ends of the implant, you should be able to confirm the presence of the 4 cm rod (Figure 9). See "If the rod is not palpable after insertion" below.
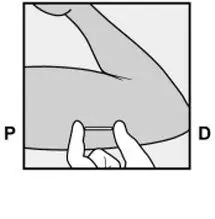 |
| Figure 9 |
Step 18. Request that the woman palpate the implant.
Step 19. Apply a pressure bandage with sterile gauze to minimize bruising. The woman may remove the pressure bandage in 24 hours and the small adhesive bandage over the insertion site after 3 to 5 days.
Step 20. Complete the USER CARD and give it to the woman to keep. Also, complete the PATIENT CHART LABEL and affix it to the woman's medical record.
Step 21. The applicator is for single use only and should be disposed in accordance with the Center for Disease Control and Prevention guidelines for handling of hazardous waste.
If the rod is not palpable after insertion:
If you cannot feel the implant or are in doubt of its presence, the implant may not have been inserted or it may have been inserted deeply:
- Check the applicator. The needle should be fully retracted and only the purple tip of the obturator should be visible.
- Use other methods to confirm the presence of the implant. Given the radiopaque nature of the implant, suitable methods for localization are two-dimensional X-ray and X-ray computerized tomography (CT scan). Ultrasound scanning (USS) with a high-frequency linear array transducer (10 MHz or greater) or magnetic resonance imaging (MRI) may be used. If these methods fail, call the Organon Service Center at 1-844-674-3200 for information on the procedure for measuring etonogestrel blood levels which can be used for verification of the presence of the implant.
Until the presence of the implant has been verified, the woman should be advised to use a non-hormonal contraceptive method, such as condoms.
Deeply-placed implants should be localized and removed as soon as possible to avoid the potential for distant migration [see Warnings and Precautions (5.1)].
2.3 Removal of NEXPLANON
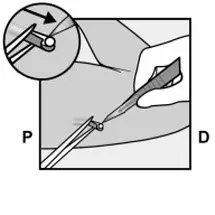
 Removal of the implant should only be performed under aseptic conditions by a healthcare professional who is familiar with the removal technique.
Removal of the implant should only be performed under aseptic conditions by a healthcare professional who is familiar with the removal technique.  Step 2. Locate the implant by palpation. Push down the end of the implant closest to the shoulder (Figure 10) to stabilize it; a bulge should appear indicating the tip of the implant that is closest to the elbow.
Step 2. Locate the implant by palpation. Push down the end of the implant closest to the shoulder (Figure 10) to stabilize it; a bulge should appear indicating the tip of the implant that is closest to the elbow. 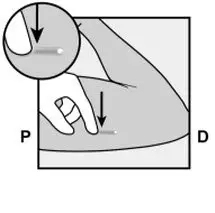
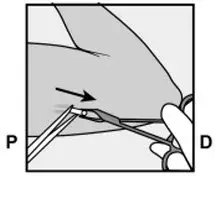
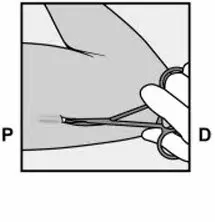
 Step 8. With a second pair of forceps carefully dissect the tissue around the implant and grasp the implant (Figure 18). The implant can then be removed
Step 8. With a second pair of forceps carefully dissect the tissue around the implant and grasp the implant (Figure 18). The implant can then be removed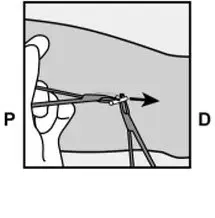
Localization and Removal of a Non-Palpable Implant
There have been reports of migration of the implant; usually this involves minor movement relative to the original position [see Warnings and Precautions (5.1)], but may lead to the implant not being palpable at the location in which it was placed. An implant that has been deeply inserted or has migrated may not be palpable and therefore imaging procedures, as described below, may be required for localization.
A non-palpable implant should always be located prior to attempting removal. Given the radiopaque nature of the implant, suitable methods for localization include two-dimensional X-ray and X-ray computer tomography (CT). Ultrasound scanning (USS) with a high-frequency linear array transducer (10 MHz or greater) or magnetic resonance imaging (MRI) may be used. Once the implant has been localized in the arm, the implant should be removed by a healthcare professional experienced in removing deeply placed implants and familiar with the anatomy of the arm. The use of ultrasound guidance during the removal should be considered.
If the implant cannot be found in the arm after comprehensive localization attempts, consider applying imaging techniques to the chest as events of migration to the pulmonary vasculature have been reported. If the implant is located in the chest, surgical or endovascular procedures may be needed for removal; healthcare professionals familiar with the anatomy of the chest should be consulted.
If at any time these imaging methods fail to locate the implant, etonogestrel blood level determination can be used for verification of the presence of the implant. For details on etonogestrel blood level determination, call 1-844-674-3200 for further instructions.
If the implant migrates within the arm, removal may require a minor surgical procedure with a larger incision or a surgical procedure in an operating room. Removal of deeply inserted implants should be conducted with caution in order to help prevent injury to deeper neural or vascular structures in the arm. Non-palpable and deeply inserted implants should be removed by healthcare professionals familiar with the anatomy of the arm and removal of deeply-inserted implants.
Exploratory surgery without knowledge of the exact location of the implant is strongly discouraged.
2.4 Replacing NEXPLANON
Immediate replacement can be done after removal of the previous implant and is similar to the insertion procedure described in section 2.2 Insertion of NEXPLANON.
The new implant may be inserted in the same arm, and through the same incision from which the previous implant was removed, as long as the site is in the correct location, i.e., 8-10 cm from the medial epicondyle of the humerus and 3-5 cm posterior to (below) the sulcus [see Dosage and Administration (2.2)]. If the same incision is being used to insert a new implant, anesthetize the insertion site [for example, 2 mL lidocaine (1%)] applying it just under the skin along the 'insertion canal.'
Follow the subsequent steps in the insertion instructions [see Dosage and Administration (2.2)].
3. Dosage Forms and Strengths
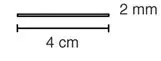
Single, white/off-white, soft, radiopaque, flexible, ethylene vinyl acetate (EVA) copolymer implant, 4 cm in length and 2 mm in diameter containing 68 mg etonogestrel, 15 mg of barium sulfate and 0.1 mg of magnesium stearate.
4. Contraindications
NEXPLANON should not be used in women who have
- Known or suspected pregnancy
- Current or past history of thrombosis or thromboembolic disorders
- Liver tumors, benign or malignant, or active liver disease
- Undiagnosed abnormal genital bleeding
- Known or suspected breast cancer, personal history of breast cancer, or other progestin-sensitive cancer, now or in the past
- Allergic reaction to any of the components of NEXPLANON [see Adverse Reactions (6)]
5. Warnings and Precautions
The following information is based on experience with the etonogestrel implants (IMPLANON and/or NEXPLANON), other progestin-only contraceptives, or experience with combination (estrogen plus progestin) oral contraceptives.
5.1 Complications of Insertion and Removal
NEXPLANON should be inserted subdermally so that it will be palpable after insertion, and this should be confirmed by palpation immediately after insertion. Failure to insert NEXPLANON properly may go unnoticed unless it is palpated immediately after insertion. Undetected failure to insert the implant may lead to an unintended pregnancy. Complications related to insertion and removal procedures, such as pain, paresthesias, bleeding, hematoma, scarring or infection, may occur.
If NEXPLANON is inserted deeply (intramuscular or in the fascia), neural or vascular injury may occur. To help reduce the risk of neural or vascular injury, NEXPLANON should be inserted subdermally just under the skin at the inner side of the non-dominant upper arm overlying the triceps muscle about 8-10 cm (3-4 inches) from the medial epicondyle of the humerus and 3-5 cm (1.25-2 inches) posterior to (below) the sulcus (groove) between the biceps and triceps muscles. This location is intended to avoid the large blood vessels and nerves lying within and surrounding the sulcus. Deep insertions of NEXPLANON have been associated with paresthesia (due to neural injury), migration of the implant (due to intramuscular or fascial insertion), and intravascular insertion. If infection develops at the insertion site, start suitable treatment. If the infection persists, the implant should be removed. Incomplete insertions or infections may lead to expulsion.
Implant removal may be difficult or impossible if the implant is not inserted correctly, is inserted too deeply, not palpable, encased in fibrous tissue, or has migrated.
There have been reports of migration of the implant within the arm from the insertion site, which may be related to deep insertion. There also have been postmarketing reports of implants located within the vessels of the arm and the pulmonary artery, which may be related to deep insertions or intravascular insertion. Some cases of implants found within the pulmonary artery were associated with chest pain and/or respiratory disorders (such as dyspnea, cough, or hemoptysis); others were asymptomatic. In cases where the implant has migrated to the pulmonary artery, endovascular or surgical procedures may be needed for removal.
If at any time the implant cannot be palpated, it should be localized, and removal is recommended.
Exploratory surgery without knowledge of the exact location of the implant is strongly discouraged. Removal of deeply inserted implants should be conducted with caution in order to prevent injury to deeper neural or vascular structures in the arm and be performed by healthcare professionals familiar with the anatomy of the arm. If the implant is located in the chest, healthcare professionals familiar with the anatomy of the chest should be consulted. Failure to remove the implant may result in continued effects of etonogestrel, such as compromised fertility, ectopic pregnancy, or persistence or occurrence of a drug-related adverse event.
5.2 Changes in Menstrual Bleeding Patterns
After starting NEXPLANON, women are likely to have a change from their normal menstrual bleeding pattern. These may include changes in bleeding frequency (absent, less, more frequent or continuous), intensity (reduced or increased) or duration. In clinical trials of the non-radiopaque etonogestrel implant (IMPLANON), bleeding patterns ranged from amenorrhea (1 in 5 women) to frequent and/or prolonged bleeding (1 in 5 women). The bleeding pattern experienced during the first three months of NEXPLANON use is broadly predictive of the future bleeding pattern for many women. Women should be counseled regarding the bleeding pattern changes they may experience so that they know what to expect. Abnormal bleeding should be evaluated as needed to exclude pathologic conditions or pregnancy.
In clinical studies of the non-radiopaque etonogestrel implant, reports of changes in bleeding pattern were the most common reason for stopping treatment (11.1%). Irregular bleeding (10.8%) was the single most common reason women stopped treatment, while amenorrhea (0.3%) was cited less frequently. In these studies, women had an average of 17.7 days of bleeding or spotting every 90 days (based on 3,315 intervals of 90 days recorded by 780 patients). The percentages of patients having 0, 1-7, 8-21, or >21 days of spotting or bleeding over a 90-day interval while using the non-radiopaque etonogestrel implant are shown in Table 1.
| Total Days of Bleeding or Spotting | Percentage of Patients | ||
|---|---|---|---|
| Treatment Days 91-180 (N = 745) | Treatment Days 271-360 (N = 657) | Treatment Days 631-720 (N = 547) |
|
| 0 Days | 19% | 24% | 17% |
| 1-7 Days | 15% | 13% | 12% |
| 8-21 Days | 30% | 30% | 37% |
| >21 Days | 35% | 33% | 35% |
Bleeding patterns observed with use of the non-radiopaque etonogestrel implant for up to 2 years, and the proportion of 90-day intervals with these bleeding patterns, are summarized in Table 2.
| BLEEDING PATTERNS | DEFINITIONS | %† |
|---|---|---|
|
||
| Infrequent | Less than three bleeding and/or spotting episodes in 90 days (excluding amenorrhea) | 33.6 |
| Amenorrhea | No bleeding and/or spotting in 90 days | 22.2 |
| Prolonged | Any bleeding and/or spotting episode lasting more than 14 days in 90 days | 17.7 |
| Frequent | More than 5 bleeding and/or spotting episodes in 90 days | 6.7 |
In case of undiagnosed, persistent, or recurrent abnormal vaginal bleeding, appropriate measures should be conducted to rule out malignancy.
5.3 Ectopic Pregnancies
As with all progestin-only contraceptive products, be alert to the possibility of an ectopic pregnancy among women using NEXPLANON who become pregnant or complain of lower abdominal pain. Although ectopic pregnancies are uncommon among women using NEXPLANON, a pregnancy that occurs in a woman using NEXPLANON may be more likely to be ectopic than a pregnancy occurring in a woman using no contraception.
5.4 Thrombotic and Other Vascular Events
The use of combination hormonal contraceptives (progestin plus estrogen) increases the risk of vascular events, including arterial events (strokes and myocardial infarctions) or deep venous thrombotic events (venous thromboembolism, deep venous thrombosis, retinal vein thrombosis, and pulmonary embolism). NEXPLANON is a progestin-only contraceptive. It is unknown whether this increased risk is applicable to etonogestrel alone. It is recommended, however, that women with risk factors known to increase the risk of venous and arterial thromboembolism be carefully assessed.
There have been postmarketing reports of serious arterial thrombotic and venous thromboembolic events, including cases of pulmonary emboli (some fatal), deep vein thrombosis, myocardial infarction, and strokes, in women using etonogestrel implants. NEXPLANON should be removed in the event of a thrombosis.
Due to the risk of thromboembolism associated with pregnancy and immediately following delivery, NEXPLANON should not be used prior to 21 days postpartum. Women with a history of thromboembolic disorders should be made aware of the possibility of a recurrence.
Evaluate for retinal vein thrombosis immediately if there is unexplained loss of vision, proptosis, diplopia, papilledema, or retinal vascular lesions.
Consider removal of the NEXPLANON implant in case of long-term immobilization due to surgery or illness.
5.5 Ovarian Cysts
If follicular development occurs, atresia of the follicle is sometimes delayed, and the follicle may continue to grow beyond the size it would attain in a normal cycle. Generally, these enlarged follicles disappear spontaneously. On rare occasion, surgery may be required.
5.6 Carcinoma of the Breast and Reproductive Organs
Women who currently have or have had breast cancer should not use hormonal contraception because breast cancer may be hormonally sensitive [see Contraindications (4)]. Some studies suggest that the use of combination hormonal contraceptives might increase the incidence of breast cancer; however, other studies have not confirmed such findings.
Some studies suggest that the use of combination hormonal contraceptives is associated with an increase in the risk of cervical cancer or intraepithelial neoplasia. However, there is controversy about the extent to which these findings are due to differences in sexual behavior and other factors.
Women with a family history of breast cancer or who develop breast nodules should be carefully monitored.
5.7 Liver Disease
Disturbances of liver function may necessitate the discontinuation of hormonal contraceptive use until markers of liver function return to normal. Remove NEXPLANON if jaundice develops.
Hepatic adenomas are associated with combination hormonal contraceptives use. An estimate of the attributable risk is 3.3 cases per 100,000 for combination hormonal contraceptives users. It is not known whether a similar risk exists with progestin-only methods like NEXPLANON.
The progestin in NEXPLANON may be poorly metabolized in women with liver impairment. Use of NEXPLANON in women with active liver disease or liver cancer is contraindicated [see Contraindications (4)].
5.8 Weight Gain
In clinical studies, mean weight gain in U.S. non-radiopaque etonogestrel implant (IMPLANON) users was 2.8 pounds after one year and 3.7 pounds after two years. How much of the weight gain was related to the non-radiopaque etonogestrel implant is unknown. In studies, 2.3% of the users reported weight gain as the reason for having the non-radiopaque etonogestrel implant removed.
5.9 Elevated Blood Pressure
Women with a history of hypertension-related diseases or renal disease should be discouraged from using hormonal contraception. For women with well-controlled hypertension, use of NEXPLANON can be considered. Women with hypertension using NEXPLANON should be closely monitored. If sustained hypertension develops during the use of NEXPLANON, or if a significant increase in blood pressure does not respond adequately to antihypertensive therapy, NEXPLANON should be removed.
5.10 Gallbladder Disease
Studies suggest a small increased relative risk of developing gallbladder disease among combination hormonal contraceptive users. It is not known whether a similar risk exists with progestin-only methods like NEXPLANON.
5.11 Carbohydrate and Lipid Metabolic Effects
Use of NEXPLANON may induce mild insulin resistance and small changes in glucose concentrations of unknown clinical significance. Carefully monitor prediabetic and diabetic women using NEXPLANON.
Women who are being treated for hyperlipidemia should be followed closely if they elect to use NEXPLANON. Some progestins may elevate LDL levels and may render the control of hyperlipidemia more difficult.
5.12 Depressed Mood
Women with a history of depressed mood should be carefully observed. Consideration should be given to removing NEXPLANON in patients who become significantly depressed.
5.13 Return to Ovulation
In clinical trials with the non-radiopaque etonogestrel implant (IMPLANON), the etonogestrel levels in blood decreased below sensitivity of the assay by one week after removal of the implant. In addition, pregnancies were observed to occur as early as 7 to 14 days after removal. Therefore, a woman should re-start contraception immediately after removal of the implant if continued contraceptive protection is desired.
5.15 Contact Lenses
Contact lens wearers who develop visual changes or changes in lens tolerance should be assessed by an ophthalmologist.
5.16 Broken or Bent Implant
There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm. Based on in vitro data, when an implant is broken or bent, the release rate of etonogestrel may be slightly increased.
When an implant is removed, it is important to remove it in its entirety [see Dosage and Administration (2.3)].
6. Adverse Reactions/Side Effects
The following adverse reactions reported with the use of hormonal contraception are discussed elsewhere in the labeling:
- Changes in Menstrual Bleeding Patterns [see Warnings and Precautions (5.2)]
- Ectopic Pregnancies [see Warnings and Precautions (5.3)]
- Thrombotic and Other Vascular Events [see Warnings and Precautions (5.4)]
- Liver Disease [see Warnings and Precautions (5.7)]
6.1 Clinical Trials Experience
Adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice, because clinical trials are conducted under widely varying conditions.
In clinical trials involving 942 women who were evaluated for safety, change in menstrual bleeding patterns (irregular menses) was the most common adverse reaction causing discontinuation of use of the non-radiopaque etonogestrel implant (IMPLANON) (11.1% of women).
Adverse reactions that resulted in a rate of discontinuation of ≥1% are shown in Table 3.
| Adverse Reactions | All Studies N = 942 |
|---|---|
|
|
| Bleeding Irregularities* | 11.1% |
| Emotional Lability† | 2.3% |
| Weight Increase | 2.3% |
| Headache | 1.6% |
| Acne | 1.3% |
| Depression‡ | 1.0% |
Other adverse reactions that were reported by at least 5% of subjects in the non-radiopaque etonogestrel implant clinical trials are listed in Table 4.
| Adverse Reactions | All Studies N = 942 |
|---|---|
| Headache | 24.9% |
| Vaginitis | 14.5% |
| Weight increase | 13.7% |
| Acne | 13.5% |
| Breast pain | 12.8% |
| Abdominal pain | 10.9% |
| Pharyngitis | 10.5% |
| Leukorrhea | 9.6% |
| Influenza-like symptoms | 7.6% |
| Dizziness | 7.2% |
| Dysmenorrhea | 7.2% |
| Back pain | 6.8% |
| Emotional lability | 6.5% |
| Nausea | 6.4% |
| Pain | 5.6% |
| Nervousness | 5.6% |
| Depression | 5.5% |
| Hypersensitivity | 5.4% |
| Insertion site pain | 5.2% |
In a clinical trial of NEXPLANON, in which investigators were asked to examine the implant site after insertion, implant site reactions were reported in 8.6% of women. Erythema was the most frequent implant site complication, reported during or shortly after insertion, occurring in 3.3% of subjects. Additionally, hematoma (3.0%), bruising (2.0%), pain (1.0%), and swelling (0.7%) were reported.
6.2 Postmarketing Experience
Adverse Reactions and Events from Postmarketing Study
Nexplanon Observational Risk Assessment Study (NORA)
A postmarketing prospective active surveillance study was conducted among 7,364 patients in the United States to characterize the frequency of insertion-, localization-, and removal-related events.
Implant Insertion
Insertion difficulty or an insertion-related event occurred in 2.6% of the study participants. The overall incidence of incorrect insertion (unrecognized non-insertion, partial insertion, and deep insertion), reported by healthcare professionals was 12.6 per 1,000 insertions (95% CI, 10.2, 15.5). Table 5 summarizes the types and frequencies of these incorrect insertions.
| Type of Incorrect Insertion Event | Number of Events* | Incidence per 1,000 Insertions (95% CI) |
|---|---|---|
|
||
| (Initially) Unrecognized Non-insertions | 1 | 0.1 (0.0-0.8) |
| Partial Insertions | 27 | 3.7 (2.4-5.3) |
| Deep Insertions | 65 | 8.8 (6.8-11.2) |
| Injury to nerve or blood vessel | 1 | 0.1 (0.0-0.8) |
| Implant located within muscle | 2 | 0.3 (0.0-1.0) |
| Implant located adjacent to fascial tissue | 56 | 7.6 (5.8-9.9) |
| Implant not palpable | 6 | 0.8 (0.3-1.8) |
Implant Removal
Implant removal information from both healthcare professionals and patients was collected for 5,159 patients (70% of the study population). Of these patients, data were available from healthcare professionals regarding 4,373 removal procedures. Healthcare professionals reported removal-related difficulties or complications in 1.5% of removal procedures. Table 6 provides a summary.
| Removal Related Events | Number of Events* | Incidence per 1,000 Removals (95% CI) |
|---|---|---|
|
||
| Any Event † | 60 | 13.7 (10.5-17.6) |
| Encased in Fibrotic Tissue | 29 | 6.6 (4.4-9.5) |
| Implant Too Deep | 11 | 2.5 (1.3-4.5) |
| Implant Migrated ‡ | 6 | 1.4 (0.5-3.0) |
| Multiple Attempts Required | 13 | 3.0 (1.6-5.1) |
| Other § | 14 | 3.2 (1.8-5.4) |
At the time of implant removal, eighteen implants (0.4% of all localizations or removals) were not palpable by the healthcare professionals. Of these eighteen, eleven were localized and removed, and one was localized but left in situ. Removal was not attempted for six non-palpable implants due to underlying health conditions, administrative problems, or unspecified reasons.
There were no reports of implants having migrated more than a few centimeters from the insertion site and no reports of implants localized at a site other than the arm. No neurovascular injuries were reported by healthcare professionals.
Adverse Reactions Reported by Patients
Table 7 provides a summary of adverse reactions reported by patients at the time of implant insertion and after removal.
| Patient Reported Adverse Reactions | At Insertion | After Removal | ||
|---|---|---|---|---|
| N* | Incidence per 1000 insertions (95% CI) | N* | Incidence per 1000 insertions (95% CI) | |
|
||||
| Any Event† | 49 | 6.7 (4.9-8.8) | 42‡ | 5.7 (4.1-7.7) |
| Pins and Needles/Numbness (arm/hand/fingers) | 17 | 2.3 (1.4-3.7) | 24 | 3.3 (2.1-4.9) |
| Severe Pain | 10 | 1.4 (0.7-2.5) | 11 | 1.5 (0.8-2.7) |
| Altered Strength/Movement | 3 | 0.4 (0.1-1.2) | 8 | 1.1 (0.5-2.1) |
| Injury to Blood Vessels or Blood Clots in Arm § | 2 | 0.3 (0-1.0) | -- | -- |
| Other ¶ | 22 | 3.0 (1.9-4.5) | 18 | 2.4 (1.5-3.9) |
In summary, this prospective active surveillance study showed that the frequency of insertion-, localization-, and removal-related events is consistent with results previously reported from clinical trials.
Adverse Reactions from Postmarketing Spontaneous Reports
The following additional adverse reactions have been identified during post-approval use of IMPLANON and NEXPLANON. It is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure because these reactions are reported voluntarily from a population of uncertain size.
Gastrointestinal disorders: constipation, diarrhea, flatulence, vomiting.
General disorders and administration site conditions: edema, fatigue, implant site reaction, pyrexia.
Immune system disorders: anaphylactic reactions.
Infections and infestations: rhinitis, urinary tract infection.
Investigations: clinically relevant rise in blood pressure, weight decreased.
Metabolism and nutrition disorders: increased appetite.
Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal pain, myalgia.
Nervous system disorders: convulsions, migraine, somnolence.
Pregnancy, puerperium and perinatal conditions: ectopic pregnancy.
Psychiatric disorders: anxiety, insomnia, libido decreased.
Renal and urinary disorders: dysuria.
Reproductive system and breast disorders: breast discharge, breast enlargement, ovarian cyst, pruritus genital, vulvovaginal discomfort.
Skin and subcutaneous tissue disorders: angioedema, aggravation of angioedema and/or aggravation of hereditary angioedema, alopecia, chloasma, hypertrichosis, pruritus, rash, seborrhea, urticaria.
Vascular disorders: hot flush.
Complications related to insertion or removal of the etonogestrel implants reported include: bruising, slight local irritation, pain or itching, fibrosis at the implant site, paresthesia or paresthesia-like events, scarring and abscess. Expulsion or migration of the implant has been reported, including to the chest wall. In some cases, implants have been found within the vasculature, including the pulmonary artery. Some cases of implants found within the pulmonary artery reported chest pain and/or respiratory disorders (such as dyspnea, cough, or hemoptysis); others have been reported as asymptomatic [see Warnings and Precautions (5.1)]. In-patient surgical interventions might be necessary when removing implants associated with complications.
7. Drug Interactions
Consult the labeling of concurrently-used drugs to obtain further information about interactions with hormonal contraceptives or the potential for enzyme alterations.
7.2 Effects of Hormonal Contraceptives on Other Drugs
Hormonal contraceptives may affect the metabolism of other drugs. Consequently, plasma concentrations may either increase (for example, cyclosporine) or decrease (for example, lamotrigine). Consult the labeling of all concurrently-used drugs to obtain further information about interactions with hormonal contraceptives or the potential for enzyme alterations.
8. Use In Specific Populations
8.2 Lactation
Data
The amount of etonogestrel contained within breast milk was measured in 38 lactating women who began using IMPLANON during the fourth to eighth week postpartum. The study evaluated Implanon versus another contraceptive, was not randomized and data were considered observational and exploratory; therefore, comparisons could not be made. Based on the findings of this study, during the first months after insertion of IMPLANON, when maternal blood levels of etonogestrel are highest, about 100 ng of etonogestrel may be ingested by the child per day based on an average daily milk ingestion of 658 mL. Based on daily milk ingestion of 150 mL/kg, the mean daily infant etonogestrel dose one month after insertion of IMPLANON is about 2.2% of the weight-adjusted maternal daily dose, or about 0.2% of the estimated absolute maternal daily dose. Adverse reactions were not observed in breastfed infants exposed to etonogestrel through breast milk. No adverse effects on the production or quality of breast milk were detected.
8.4 Pediatric Use
Safety and efficacy of NEXPLANON have been established in women of reproductive age. Safety and efficacy of NEXPLANON are expected to be the same for postpubertal adolescents. However, no clinical studies have been conducted in women less than 18 years of age. Use of this product before menarche is not indicated.
8.5 Geriatric Use
This product has not been studied in women over 65 years of age and is not indicated in this population.
8.6 Hepatic Impairment
No studies were conducted to evaluate the effect of hepatic disease on the disposition of NEXPLANON. The use of NEXPLANON in women with active liver disease is contraindicated [see Contraindications (4)].
8.7 Overweight Women
The effectiveness of the etonogestrel implant in women who weighed more than 130% of their ideal body weight has not been defined because such women were not studied in clinical trials. Serum concentrations of etonogestrel are inversely related to body weight and decrease with time after implant insertion. It is therefore possible that NEXPLANON may be less effective in overweight women, especially in the presence of other factors that decrease serum etonogestrel concentrations such as concomitant use of hepatic enzyme inducers.
10. Overdosage
Overdosage may result if more than one implant is inserted. In case of suspected overdose, the implant should be removed.
11. Nexplanon Description
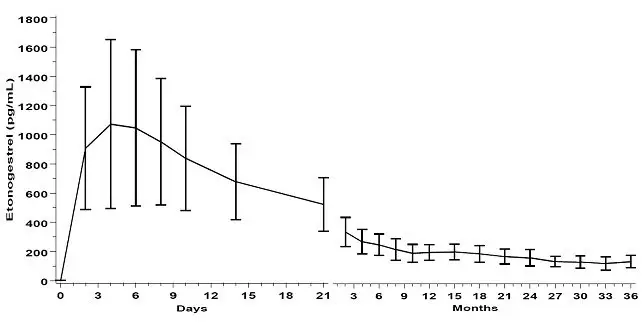
NEXPLANON is a radiopaque, progestin-only, soft, flexible implant preloaded in a sterile, disposable applicator for subdermal use. The implant is white/off-white, non-biodegradable and 4 cm in length with a diameter of 2 mm (see Figure 19). Each implant consists of an ethylene vinyl acetate (EVA) copolymer (28% vinyl acetate, 43 mg) core, containing 68 mg of the synthetic progestin etonogestrel, barium sulfate ((15 mg), radiopaque ingredient), and magnesium stearate (0.1 mg), surrounded by an EVA copolymer skin. Once inserted subdermally, the release rate is 60-70 mcg/day in week 5-6 and decreases to approximately 35-45 mcg/day at the end of the first year, to approximately 30-40 mcg/day at the end of the second year, and then to approximately 25-30 mcg/day at the end of the third year. NEXPLANON is a progestin-only contraceptive and does not contain estrogen. NEXPLANON does not contain latex.
 |
| Figure 19 (Not to scale) |
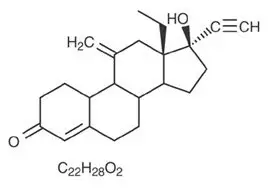
Etonogestrel [13-Ethyl-17-hydroxy-11-methylene-18,19-dinor-17α-pregn-4-en-20-yn-3-one], structurally derived from 19-nortestosterone, is the synthetic biologically active metabolite of the synthetic progestin desogestrel. It has a molecular weight of 324.46 and the following structural formula (Figure 20).
 |
| Figure 20 |
12. Nexplanon - Clinical Pharmacology
12.1 Mechanism of Action
The contraceptive effect of NEXPLANON is achieved by suppression of ovulation, increased viscosity of the cervical mucus, and alterations in the endometrium.
13. Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
In a 24-month carcinogenicity study in rats with subdermal implants releasing 10 and 20 mcg etonogestrel per day (equal to approximately 1.8-3.6 times the systemic steady state exposure in women using NEXPLANON), no drug-related carcinogenic potential was observed. Etonogestrel was not genotoxic in the in vitro Ames/Salmonella reverse mutation assay, the chromosomal aberration assay in Chinese hamster ovary cells or in the in vivo mouse micronucleus test. Fertility in rats returned after withdrawal from treatment.
14. Clinical Studies
14.1 Pregnancy
In clinical trials of up to 3 years duration that involved 923 subjects, 18-40 years of age at entry, and 1756 women-years of use with the non-radiopaque etonogestrel implant (IMPLANON), the total exposures expressed as 28-day cycle equivalents by study year were:
Year 1: 10,866 cycles
Year 2: 8,581 cycles
Year 3: 3,442 cycles
The clinical trials excluded women who:
- Weighed more than 130% of their ideal body weight
- Were chronically taking medications that induce liver enzymes
In the subgroup of women, 18-35 years of age at entry, 6 pregnancies during 20,648 cycles of use were reported. Two pregnancies occurred in each of Years 1, 2, and 3. Each conception was likely to have occurred shortly before or within 2 weeks after removal of the non-radiopaque etonogestrel implant. With these 6 pregnancies, the cumulative Pearl Index was 0.38 pregnancies per 100 women-years of use.
14.2 Return to Ovulation
In clinical trials with the non-radiopaque etonogestrel implant (IMPLANON), the etonogestrel levels in blood decreased below sensitivity of the assay by one week after removal of the implant. In addition, pregnancies were observed to occur as early as 7 to 14 days after removal. Therefore, a woman should re-start contraception immediately after removal of the implant if continued contraceptive protection is desired.
14.3 Implant Insertion and Removal Characteristics
Out of 301 insertions of the NEXPLANON implant in a clinical trial, the mean insertion time (from the removal of the protection cap of the applicator until retraction of the needle from the arm) was 27.9 ± 29.3 seconds. After insertion, 300 out of 301 (99.7%) NEXPLANON implants were palpable. The single, non-palpable implant was not inserted according to the instructions.
For 112 out of 114 (98.2%) subjects in 2 clinical trials for whom insertion and removal data were available, NEXPLANON implants were clearly visible with use of two-dimensional x-ray after insertion. The two implants that were not clearly visible after insertion were clearly visible with two-dimensional x-ray before removal.
16. How is Nexplanon supplied
16.1 How Supplied
NEXPLANON is supplied as follows:
NDC 78206-145-01
One NEXPLANON package consists of a single implant containing 68 mg etonogestrel, 15 mg of barium sulfate and 0.1 mg of magnesium stearate that is 4 cm in length and 2 mm in diameter, which is pre-loaded in the needle of a disposable applicator. The sterile applicator containing the implant is packed in a blister pack.
17. Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information).
- Counsel women about the insertion and removal procedure of the NEXPLANON implant. Provide the woman with a copy of the Patient Labeling and ensure that she understands the information in the Patient Labeling before insertion and removal. A USER CARD and consent form are included in the packaging. Have the woman complete a consent form and retain it in your records. The USER CARD should be filled out and given to the woman after insertion of the NEXPLANON implant so that she will have a record of the location of the implant in the upper arm and when it should be removed.
- Counsel women to contact their healthcare professional immediately if, at any time, they are unable to palpate the implant.
- Counsel women that NEXPLANON does not protect against HIV infection (AIDS) or other sexually transmitted diseases.
- Counsel women that the use of NEXPLANON may be associated with changes in their normal menstrual bleeding patterns so that they know what to expect.
FDA-Approved Patient Labeling
NEXPLANON® (etonogestrel implant)
Radiopaque
Subdermal Use Only
NEXPLANON® does not protect against HIV infection (the virus that causes AIDS) or other sexually transmitted diseases.
Read this Patient Information leaflet carefully before you decide if NEXPLANON is right for you. This information does not take the place of talking with your healthcare provider. If you have any questions about NEXPLANON, ask your healthcare provider.
What is NEXPLANON?
NEXPLANON is a hormone-releasing birth control implant for use by women to prevent pregnancy for up to 3 years. The implant is a flexible plastic rod about the size of a matchstick that contains a progestin hormone called etonogestrel. It contains a small amount of barium sulfate (15 mg), so that the implant can be seen by X-ray, an ethylene vinyl acetate (EVA) copolymer (28% vinyl acetate, 43 mg) core, and magnesium stearate (0.1 mg). Your healthcare provider will insert the implant just under the skin of the inner side of your upper arm. You can use a single NEXPLANON implant for up to 3 years. NEXPLANON does not contain estrogen.

What if I need birth control for more than 3 years?
The NEXPLANON implant must be removed after 3 years. Your healthcare provider can insert a new implant under your skin after taking out the old one if you choose to continue using NEXPLANON for birth control.
What if I change my mind about birth control and want to stop using NEXPLANON before 3 years?
Your healthcare provider can remove the implant at any time. You may become pregnant as early as the first week after removal of the implant. If you do not want to get pregnant after your healthcare provider removes the NEXPLANON implant, you should start another birth control method right away.
How does NEXPLANON work?
NEXPLANON prevents pregnancy in several ways. The most important way is by stopping the release of an egg from your ovary. NEXPLANON also thickens the mucus in your cervix and this change may keep sperm from reaching the egg. NEXPLANON also changes the lining of your uterus.
How well does NEXPLANON work?
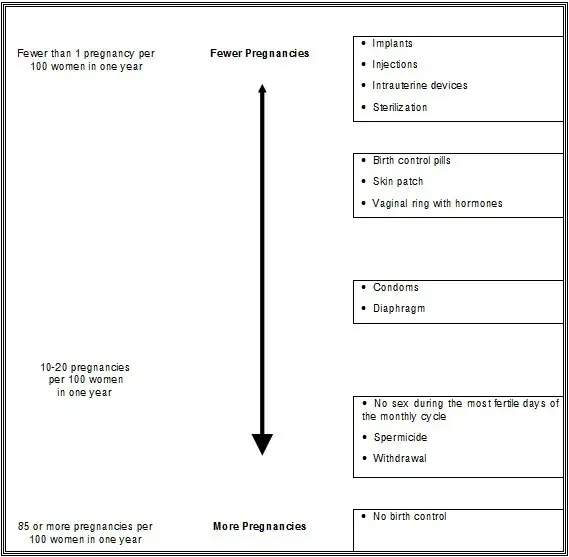
When the NEXPLANON implant is placed correctly, your chance of getting pregnant is very low (less than 1 pregnancy per 100 women who use NEXPLANON for 1 year). It is not known if NEXPLANON is as effective in very overweight women because studies did not include many overweight women.
The following chart shows the chance of getting pregnant for women who use different methods of birth control. Each box on the chart contains a list of birth control methods that are similar in effectiveness. The most effective methods are at the top of the chart. The box on the bottom of the chart shows the chance of getting pregnant for women who do not use birth control and are trying to get pregnant.
Who should not use NEXPLANON?
Do not use NEXPLANON if you:
-
Are pregnant or think you may be pregnant
- Have, or have had blood clots, such as blood clots in your legs (deep venous thrombosis), lungs (pulmonary embolism), eyes (total or partial blindness), heart (heart attack), or brain (stroke)
- Have liver disease or a liver tumor
- Have unexplained vaginal bleeding
- Have breast cancer or any other cancer that is sensitive to progestin (a female hormone), now or in the past
- Are allergic to anything in NEXPLANON
Tell your healthcare provider if you have or have had any of the conditions listed above. Your healthcare provider can suggest a different method of birth control.
In addition, talk to your healthcare provider about using NEXPLANON if you:
- Have diabetes
- Have high cholesterol or triglycerides
- Have headaches
- Have gallbladder or kidney problems
- Have a history of depressed mood
- Have high blood pressure
- Have an allergy to numbing medicines (anesthetics) or medicines used to clean your skin (antiseptics). These medicines will be used when the implant is placed into or removed from your arm.
Interaction with Other Medicines
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription medicines, vitamins and herbal supplements. Certain medicines may make NEXPLANON less effective, including:
- aprepitant
- barbiturates
- bosentan
- carbamazepine
- felbamate
- griseofulvin
- oxcarbazepine
- phenytoin
- rifampin
- St. John's wort
- topiramate
- HIV medicines
- Hepatitis C Virus medicines
Ask your healthcare provider if you are not sure if your medicine is one listed above.
If you are taking medicines or herbal products that might make NEXPLANON less effective, you and your healthcare provider may decide to leave NEXPLANON in place; in that case, an additional non-hormonal contraceptive should be used. Because the effect of another medicine on NEXPLANON may last up to 28 days after stopping the medicine, it is necessary to use the additional non-hormonal contraceptive for that long.
When you are using NEXPLANON, tell all of your healthcare providers that you have NEXPLANON in place in your arm.
How is the NEXPLANON implant placed and removed?
Your healthcare provider will place and remove the NEXPLANON implant in a minor surgical procedure in his or her office. The implant is placed just under the skin on the inner side of your non-dominant upper arm.
The timing of insertion is important. Your healthcare provider may:
- Perform a pregnancy test before inserting NEXPLANON
- Schedule the insertion at a specific time of your menstrual cycle (for example, within the first 5 days of your regular menstrual bleeding). If the implant is placed after the fifth day of menses, then you should use an additional contraceptive method (such as a condom) for the first 7 days after insertion.
Your healthcare provider will cover the site where NEXPLANON was placed with 2 bandages. Leave the top bandage on for 24 hours. Keep the smaller bandage clean, dry, and in place for 3 to 5 days.
Immediately after the NEXPLANON implant has been placed, you and your healthcare provider should check that the implant is in your arm by feeling for it.
If you cannot feel the implant immediately after insertion, the implant may not have been inserted, or it may have been inserted deeply. A deep insertion may cause problems with locating and removing the implant. Once the healthcare provider has located the implant, it should be removed.
If at any time you cannot feel the NEXPLANON implant, contact your healthcare provider immediately and use a non-hormonal birth control method (such as condoms) until your healthcare provider confirms that the implant is in place. You may need special tests to check that the implant is in place or to help find the implant when it is time to take it out. If the implant cannot be found in the arm after a thorough search, your healthcare provider may use x-rays or other imaging methods on your chest.
Depending on the exact position of the implant, removal may be difficult and may require surgery.
You will be asked to review and sign a consent form prior to inserting the NEXPLANON implant. You will also get a USER CARD to keep at home with your health records. Your healthcare provider will fill out the USER CARD with the date the implant was inserted and the date the implant is to be removed. Keep track of the date the implant is to be removed. Schedule an appointment with your healthcare provider to remove the implant on or before the removal date.
Be sure to have checkups as advised by your healthcare provider.
What are the most common side effects I can expect while using NEXPLANON?
• Changes in Menstrual Bleeding Patterns (menstrual periods)
The most common side effect of NEXPLANON is a change in your normal menstrual bleeding pattern. In studies, one out of ten women stopped using the implant because of an unfavorable change in their bleeding pattern. You may experience longer or shorter bleeding during your periods or have no bleeding at all. The time between periods may vary, and in between periods you may also have spotting.
Tell your healthcare provider right away if:
- You think you may be pregnant
- Your menstrual bleeding is heavy and prolonged
Besides changes in menstrual bleeding patterns, other frequent side effects that caused women to stop using the implant include:
- Mood swings
- Weight gain
- Headache
- Acne
- Depressed mood
Other common side effects include:
- Headache
- Vaginitis (inflammation of the vagina)
- Weight gain
- Acne
- Breast pain
- Viral infections such as sore throats or flu-like symptoms
- Stomach pain
- Painful periods
- Mood swings, nervousness, or depressed mood
- Back pain
- Nausea
- Dizziness
- Pain
- Pain at the site of insertion
Implants have been reported to be found in a blood vessel, including a blood vessel in the lung which can be associated with shortness of breath, cough and/or the coughing up of blood or blood-stained mucus.
This is not a complete list of possible side effects. For more information, ask your healthcare provider for advice about any side effects that concern you. You may report side effects to the FDA at 1-800-FDA-1088.
What are the possible risks of using NEXPLANON?
• Problems with Insertion and Removal
The implant may not be placed in your arm at all due to a failed insertion. If this happens, you may become pregnant. Immediately after insertion, and with help from your healthcare provider, you should be able to feel the implant under your skin. If you can't feel the implant, tell your healthcare provider.
Location and removal of the implant may be difficult or impossible because the implant is not where it should be. Special procedures, including surgery in the hospital, may be needed to remove the implant. If the implant is not removed, then the effects of NEXPLANON will continue for a longer period of time.
Implants have been found in the pulmonary artery (a blood vessel in the lung). If the implant cannot be found in the arm, your healthcare provider may use x-rays or other imaging methods on the chest. If the implant is located in the chest, surgery may be needed.
Other problems related to insertion and removal are:
- Pain, irritation, swelling, or bruising at the insertion site
- Numbness and tingling at the insertion site
- Scarring, including a thick scar called a keloid around the insertion site
- Infection
- Scar tissue may form around the implant making it difficult to remove
- The implant may come out by itself. You may become pregnant if the implant comes out by itself. Use a back-up birth control method and call your healthcare provider right away if the implant comes out.
- The need for surgery in the hospital to remove the implant
- Injury to nerves or blood vessels in your arm
- The implant breaks making removal difficult
• Ectopic Pregnancy
If you become pregnant while using NEXPLANON, you have a slightly higher chance that the pregnancy will be ectopic (occurring outside the womb) than do women who do not use birth control. Unusual vaginal bleeding or lower stomach (abdominal) pain may be a sign of ectopic pregnancy. Ectopic pregnancy is a medical emergency that often requires surgery. Ectopic pregnancies can cause serious internal bleeding, infertility, and even death. Call your healthcare provider right away if you think you are pregnant or have unexplained lower stomach (abdominal) pain.
• Ovarian Cysts
Cysts may develop on the ovaries and usually go away without treatment but sometimes surgery is needed to remove them.
• Breast Cancer
It is not known whether NEXPLANON use changes a woman's risk for breast cancer. If you have breast cancer now, or have had it in the past, do not use NEXPLANON because some breast cancers are sensitive to hormones.
• Serious Blood Clots
NEXPLANON may increase your chance of serious blood clots, especially if you have other risk factors such as smoking. It is possible to die from a problem caused by a blood clot, such as a heart attack or a stroke.
Some examples of serious blood clots are blood clots in the:
- Legs (deep vein thrombosis)
- Lungs (pulmonary embolism)
- Brain (stroke)
- Heart (heart attack)
- Eyes (total or partial blindness)
The risk of serious blood clots is increased in women who smoke. If you smoke and want to use NEXPLANON, you should quit. Your healthcare provider may be able to help.
Tell your healthcare provider at least 4 weeks before if you are going to have surgery or will need to be on bed rest. You have an increased chance of getting blood clots during surgery or bed rest.
• Other Risks
A few women who use birth control that contains hormones may get:
- High blood pressure
- Gallbladder problems
- Rare cancerous or noncancerous liver tumors
• Broken or Bent Implant
Breakage or bending of the implant may occur due to external forces (e.g., manipulation of the implant or contact sports). A broken implant may move from the insertion site. If you feel that the implant may have broken or bent while in your arm, contact your healthcare provider.
When should I call my healthcare provider?
Call your healthcare provider right away if you have:
- Pain in your lower leg that does not go away
- Severe chest pain or heaviness in the chest
- Sudden shortness of breath, sharp chest pain, or coughing blood
- Symptoms of a severe allergic reaction, such as swollen face, tongue or throat; trouble breathing or swallowing
- Sudden severe headache unlike your usual headaches
- Weakness or numbness in your arm, leg, or trouble speaking
- Sudden partial or complete blindness
- Yellowing of your skin or whites of your eyes, especially with fever, tiredness, loss of appetite, dark colored urine, or light-colored bowel movements
- Severe pain, swelling, or tenderness in the lower stomach (abdomen)
- Lump in your breast
- Problems sleeping, lack of energy, tiredness, or you feel very sad
- Heavy menstrual bleeding
What if I become pregnant while using NEXPLANON?
You should see your healthcare provider right away if you think that you may be pregnant. It is important to remove the implant and make sure that the pregnancy is not ectopic (occurring outside the womb). Based on experience with other hormonal contraceptives, NEXPLANON is not likely to cause birth defects.
Can I use NEXPLANON when I am breastfeeding?
If you are breastfeeding your child, you may use NEXPLANON if 4 weeks have passed since you had your baby. A small amount of the hormone contained in NEXPLANON passes into your breast milk. The health of breast-fed children whose mothers were using the implant has been studied up to 3 years of age in a small number of children. No effects on the growth and development of the children were seen. If you are breastfeeding and want to use NEXPLANON, talk with your healthcare provider for more information.
Additional Information
This Patient Information leaflet contains important information about NEXPLANON. If you would like more information, talk with your healthcare provider. You can ask your healthcare provider for information about NEXPLANON that is written for healthcare providers. You may also call 1-844-674-3200 or visit www.nexplanon.com.

| NEXPLANON
etonogestrel implant |
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
|
||||||||||||||||||||
| Labeler - Organon LLC (117494753) |
